Article Text

Abstract
Aims Programmed death-1/programmed death ligand 1 (PD-1/PD-L1) inhibitor therapy is accompanied by companion or complementary PD-L1 testing in some tumour types. We investigated utilisation of the Dako PD-L1 IHC 28-8 and 22C3 pharmDx assays and the Ventana PD-L1 (SP142) assay and evaluated concordance between the 28-8 and 22C3 assays in a real-world cohort of patients tested at a single US national reference laboratory.
Methods NeoGenomics Laboratories performed PD-L1 testing on tumour samples between October 2015 and March 2018. PD-L1 test results were matched with patient characteristics using unique identifiers. Concordance between the 28-8 and 22C3 assays was evaluated in matched tumour samples. Data were evaluated across multiple tumour types and in subgroups of patients with lung cancer, melanoma, squamous cell carcinoma of the head and neck, and urothelial carcinoma.
Results 62 180 individual PD-L1 tests were conducted on samples from 55 652 patients. PD-L1 test volume increased ~10-fold over the period evaluated. Test failure rates were typically low, and test turnaround time (TAT) ranged between 2 and 4 days. Concordance between the 28-8 and 22C3 assays was strong in the overall population and across tumour type subgroups (Kendall’s tau correlations of 0.94 and 0.92–0.98, respectively).
Conclusions Test failure rates for PD-L1 tests were low and TAT remained reasonable despite marked increases in test volume. Concordance was high between the 28-8 and 22C3 assays across a range of tumour types and biopsy locations. These findings add to the literature showing high concordance between the 28-8 and 22C3 assays.
- diagnostics
- histopathology
- immunohistochemistry
- oncology
- tumour markers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Various checkpoint inhibitors, including multiple programmed death-1/programmed death ligand 1 (PD-1/PD-L1) inhibitors, have been approved in the USA and around the world for the treatment of a range of tumour types. Their introduction has improved outcomes in patients with historically poor survival, such as those with metastatic melanoma or non-small cell lung cancer (NSCLC).1 2 Assays to assess PD-L1 expression have evolved alongside the development of PD-1/PD-L1 inhibitors. These assays are approved by the US Food and Drug Administration (FDA) as companion diagnostic assays (tests that provide information essential for the safe and effective use of a corresponding drug)3 or complementary diagnostic assays (tests that aid in benefit–risk decision-making about the use of a therapeutic product).4
Clinical trials that investigated PD-1/PD-L1 inhibitors have shown that PD-L1 expression may be associated with enhanced clinical benefit in some tumour types. For example, the KEYNOTE-010 trial of pembrolizumab versus docetaxel in patients with previously treated advanced NSCLC who had PD-L1 expression on ≥1% of tumour cells found that overall survival (OS) was prolonged in the pembrolizumab arm.5 KEYNOTE-042 demonstrated an improvement in OS for the pembrolizumab arm compared with standard chemotherapy in patients with advanced or metastatic NSCLC whose tumours had a PD-L1 tumour proportion score ≥1%.6 The CheckMate 057 trial demonstrated that second-line treatment with nivolumab improved OS, progression-free survival and objective response rates compared with docetaxel in patients with non-squamous (NSQ) NSCLC, with enhanced clinical responses seen at tumour cell membrane PD-L1 expression cut-offs of ≥1%, ≥5% and ≥10%.7 Thus, PD-L1 testing may help clinicians evaluate the likelihood that a patient will benefit from PD-1/PD-L1 inhibitor therapy in some tumour types. Conversely, PD-1/PD-L1 inhibitors can provide a meaningful benefit regardless of PD-L1 expression in some tumour types,8 9 and patients may be treated with PD-1/PD-L1 inhibitors without testing for PD-L1 expression in some instances.10–15
Treatment with pembrolizumab or atezolizumab in certain tumour types and therapeutic settings is restricted to patients with tumours that express PD-L1 at levels above specified cut-offs only, as assessed using approved PD-L1 companion diagnostic assays.14 15 Thus, testing with an approved companion diagnostic is required before treatment with pembrolizumab or atezolizumab in patients with these tumour types. As of September 2019, two PD-L1 assays have been approved as companion diagnostics by the US FDA. The Dako PD-L1 immunohistochemistry (IHC) 22C3 pharmDx assay (Agilent Technologies, Santa Clara, California, USA) is approved as a companion diagnostic for use with pembrolizumab in NSCLC, gastric/gastro-oesophageal junction adenocarcinoma, oesophageal squamous cell carcinoma, cervical cancer, squamous cell carcinoma of the head and neck (SCCHN) and cisplatin-ineligible urothelial carcinoma (UC).16 The Ventana PD-L1 (SP142) assay (Ventana Medical Systems, Tucson, Arizona, USA) is approved as a companion diagnostic for use with atezolizumab in patients with triple-negative breast cancer and patients with cisplatin-ineligible UC.17
As of September 2019, three PD-L1 assays have been approved by the US FDA as complementary diagnostic assays for use with nivolumab, durvalumab and atezolizumab. The Dako PD-L1 IHC 28-8 pharmDx assay (Agilent Technologies, Santa Clara, California, USA) is approved as a complementary diagnostic for use with nivolumab in NSQ NSCLC, SCCHN and UC and was approved for use in melanoma until the removal of this indication from the assay label in 2019.18–20 The Ventana PD-L1 (SP263) assay (Ventana Medical Systems, Tucson, Arizona, USA) is approved as a complementary diagnostic for use with durvalumab in patients with locally advanced or metastatic UC.21 The SP142 assay is also approved for use as a complementary diagnostic to atezolizumab in patients with metastatic NSCLC who have disease progression during or following platinum-containing chemotherapy and in patients with locally advanced or metastatic UC.17
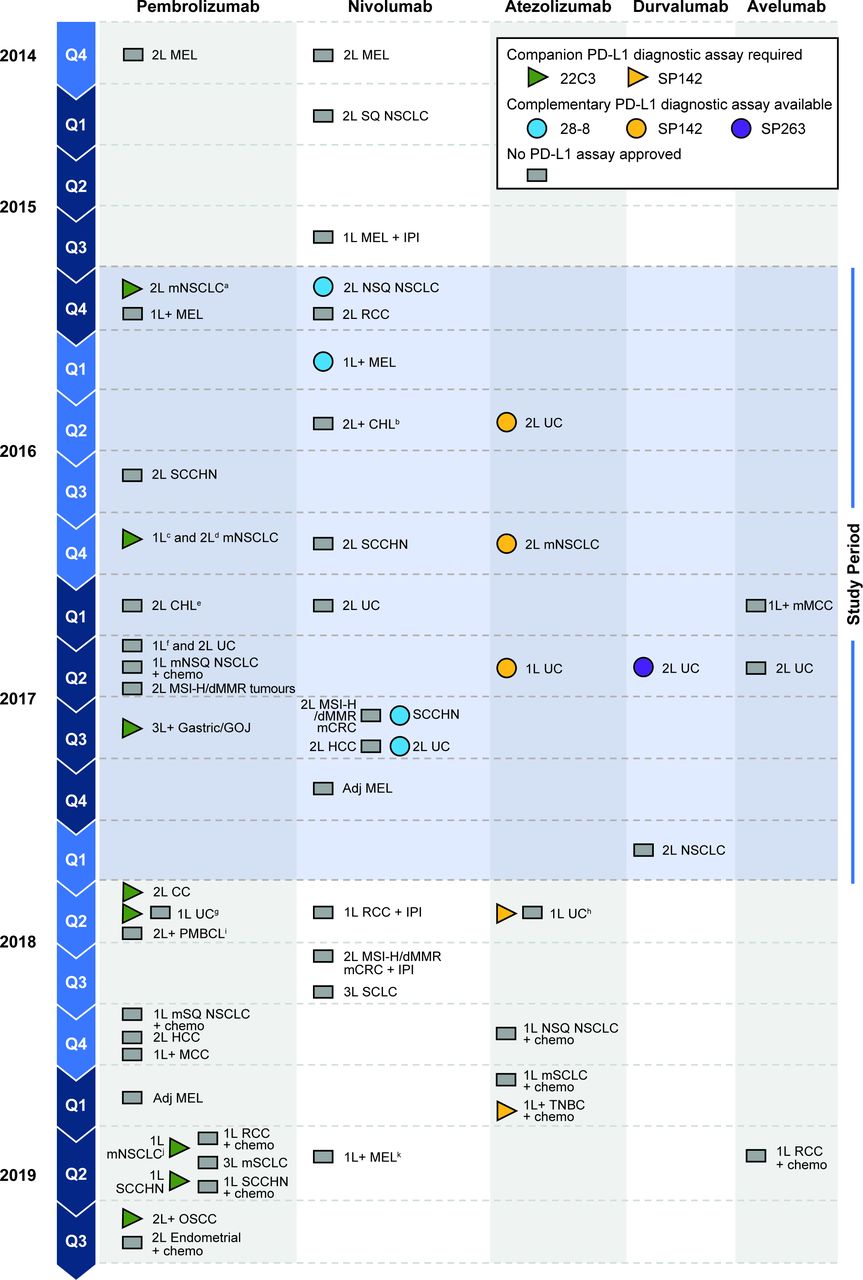
The PD-1/PD-L1 treatment landscape evolved rapidly from 2015 to 2018 (the period covered by the current real-world utilisation study), with multiple PD-1/PD-L1 inhibitor approvals accompanied by approvals of companion and complementary PD-L1 tests in various tumour types (figure 1). Because use of anti–PD-1/PD-L1 therapies in clinical practice has increased, it would be expected to have a marked effect on the uptake of PD-L1 testing.
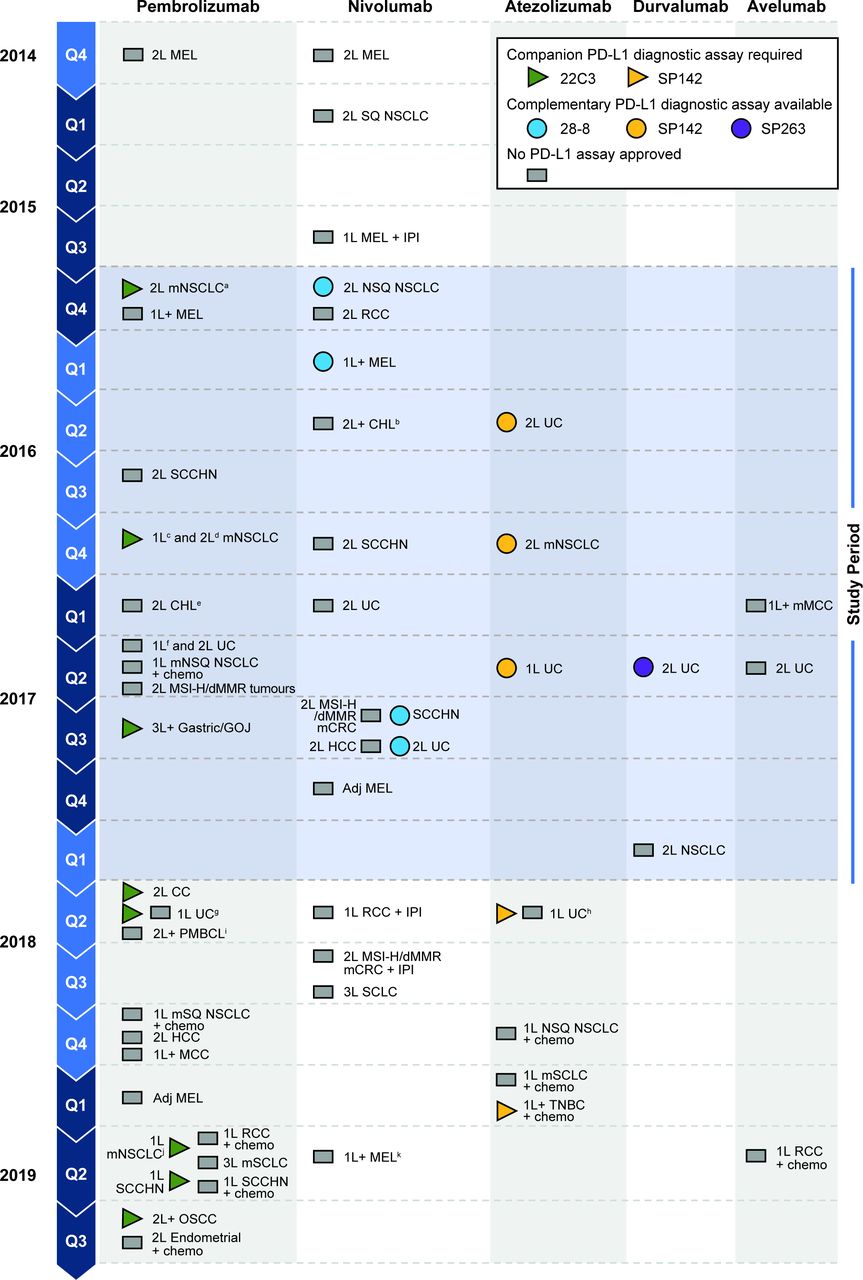
Timeline of key US FDA approvals of PD-1/PD-L1 inhibitors and PD-L1 diagnostic assays between October 2015 and September 2019.53–57 aAccelerated approval based on tumour response and PFS in patients whose tumours have a TPS ≥1%. bIn patients with CHL that has relapsed or progressed after autologous HSCT and brentuximab vedotin or ≥3 lines of systemic therapy that includes autologous HSCT. cIn patients whose tumours have a TPS ≥50%. dFinal approval based on OS in patients whose tumours have a TPS ≥1%. eIn adult and paediatric patients with refractory CHL or who have relapsed after ≥3 lines of therapy. fIn patients with cisplatin-ineligible locally advanced or metastatic disease. gIn patients with locally advanced or metastatic cisplatin-ineligible UC with PD-L1 CPS ≥10, or platinum-ineligible UC regardless of PD-L1 status. hIn patients with locally advanced or metastatic cisplatin-ineligible UC and PD-L1 stained tumour-infiltrating immune cells covering ≥5% of tumour area, or platinum-ineligible UC regardless of PD-L1 status. iIn adult or paediatric patients with refractory PMBCL or who have relapsed after two or more lines of therapy. jIn patients whose tumours have a TPS ≥1%. kComplementary status for the 28-8 assay in melanoma withdrawn. The blue shaded area corresponds to the period covered by this study (October 2015 to March 2018). 1L, first line; 2L, second line; adj, adjuvant; CC, cervical cancer; chemo, chemotherapy; CHL, classic Hodgkin lymphoma; CRC, colorectal cancer; dMMR, mismatch repair deficient; GOJ, gastro-oesophageal junction adenocarcinoma; HCC, hepatocellular carcinoma; HSCT, haematopoietic stem cell transplant; IPI, ipilimumab; m, metastatic; MCC, Merkel cell carcinoma; MEL, melanoma; MSI-H, microsatellite instability-high; NSCLC, non-small cell lung cancer; NSQ, non-squamous; OS, overall survival; OSCC, oesophageal squamous cell carcinoma; PD-1, programmed death-1; PD-L1, programmed death ligand 1; PFS, progression-free survival; PMBCL, primary mediastinal large B-cell lymphoma; RCC, renal cell carcinoma; SCCHN, squamous cell carcinoma of the head and neck; SCLC, small cell lung cancer; SQ, squamous; TNBC, triple-negative breast cancer; TPS, tumour proportion score; UC, urothelial carcinoma.
The interchangeability of PD-L1 assays, particularly in real-world clinical practice, remains an unresolved question.22 Many studies have assessed the analytical concordance of approved PD-L1 assays in various tumour types, most prominently lung cancers, with the 28-8 and 22C3 assays being among the most frequently evaluated.23–26 The analytical concordance of the 28-8 and 22C3 assays in clinical practice has also been evaluated across a range of tumour types, with real-world studies to date showing results consistent with those of studies conducted under controlled conditions.27 28 However, few studies evaluating real-world PD-L1 test uptake have been published.27 29
In the current real-world study, we evaluated testing volume, test failure and turnaround times (TATs) for the 28-8, 22C3 and SP142 assays. In addition, we assessed analytical concordance between the 28-8 and 22C3 assays across a range of tumour types tested in routine clinical practice and at clinically relevant cut-offs for tumour cell PD-L1 expression. The focus was on tumour types for which the 28-8 assay is approved, or was approved during the period in which PD-L1 testing was performed.
Methods
Samples
NeoGenomics Laboratories (Fort Myers, Florida, USA) performed PD-L1 testing on tumour samples in routine clinical practice between October 2015 and March 2018, based on the manufacturers’ protocols at the time. Clinical characteristics of patients who underwent PD-L1 testing were provided by a third-party vendor, Symphony Health Solutions (Phoenix, Arizona, USA). International Statistical Classification of Diseases and Related Health Problems (ICD)-9/10 diagnostic and treatment codes for individual tumour types30 were matched with PD-L1 test results. PD-L1 test data recorded included test order date, test used, test result and test-report availability date.
All samples were included in the overall analysis regardless of diagnosis, including patients with an unconfirmed diagnosis; analyses in individual tumour types (lung cancer, melanoma, SCCHN and UC) were based on the ICD-9/10 diagnostic code recorded, as well as other clinical characteristics documented in the database. Lung cancers were grouped into a single category because of difficulty separating the ICD-9/10 codes for NSCLC and small cell lung cancer (SCLC).
PD-L1 testing
Samples were tested using one or more of the following assays: Dako PD-L1 IHC 28-8 pharmDx, Dako PD-L1 IHC 22C3 pharmDx and Ventana PD-L1 (SP142). Testing was performed using manufacturers’ protocols that were current at the time.16 17 20 31–37
PD-L1 expression was evaluated as indicated in the diagnostic labels for assays at the time of testing. The 28-8 and 22C3 assays evaluated tumour cell PD-L1 expression,16 31 whereas the SP142 assay evaluated PD-L1 expression on tumour cells and/or immune cells.17 Tests were scored by a pathologist according to the manufacturer’s instructions. Selected pathologists employed by NeoGenomics Laboratories were trained in interpretation of PD-L1 assays by the assay manufacturers. These pathologists subsequently coordinated in-house training and online training provided by the manufacturer. Tests were typically scored by a single pathologist, with challenging results reviewed by a second pathologist.
Values for PD-L1 expression on tumour cells were pooled to compare the proportion of patients in each PD-L1 expression category. Patients with a single uniform value, defined as one quantifiable PD-L1 expression value or two or more identical PD-L1 expression values for the 28-8 or 22C3 assays, were included in the analysis. Patients with two or more discrepant PD-L1 expression values were excluded to avoid potential misclassification.
Analysis of test usage
Test utilisation was assessed using the number of tests carried out for all three assays, pooled and individually, and is shown as the total number of tests in each 3-month period (quarter). Test failure was defined as the absence of adequate sample with measurable PD-L1, and is shown as the percentage of tests that failed in each quarter for all three assays pooled. TAT was defined as the time from sample receipt by the laboratory to test-report availability, and is presented by quarter for all three assays pooled.
Concordance analysis
Concordance between the 28-8 or 22C3 assays and the SP142 assay was not evaluated due to differences in the PD-L1 scoring between these assays. Patients with two or more discrepant PD-L1 expression values from a single assay were excluded from concordance analyses to avoid potential misclassification, and only patients with a confirmed diagnosis were included.
Assay concordance was evaluated using Passing-Bablok regression, Kendall’s tau correlation and Spearman’s rank correlation, and 95% CIs were constructed using Wilson’s score interval. Bland-Altman plots with summary statistics were constructed to describe the differences between assays across the dynamic range. Overall, positive and negative percentage agreement (OPA, PPA and NPA, respectively) were evaluated at multiple PD-L1 expression cut-offs (≥1%, ≥5%, ≥10%, ≥25%, ≥50%) for tumour cell staining to reflect the range of PD-L1 thresholds under clinical evaluation across tumour types. Cohen’s kappa coefficient statistics were used to assess percentage agreement.
Results
Sample disposition and patient characteristics
A total of 62 180 individual PD-L1 tests conducted for 55 652 patients were included in the analysis, of which 28 412 tests for 25 658 patients had a PD-L1 test result and a confirmed diagnosis. A total of 3050 patients had matched samples tested once with both the 28-8 and 22C3 assays, and were included in concordance analyses (online supplementary figure 1). The majority of patients for whom diagnosis information was available had a diagnosis of lung cancer (table 1). Across all tumour types, 60% of patients had a single uniform value ≥1% for PD-L1 expression on tumour cells with the 28-8 or 22C3 assays. Details of patient and sample characteristics are shown in table 1, and patient and sample disposition are shown in online supplementary figure 1.
Supplemental material
Patient and sample characteristics
Test volume
The number of PD-L1 tests performed by NeoGenomics Laboratories increased over the study period. There was a marked increase in test volume across all tumour types between Q3 2016 and Q2 2017, and overall testing volume appeared to plateau between Q2 2017 and Q1 2018 (figure 2). The pattern of use in the lung cancer, melanoma, SCCHN and UC subgroups was generally similar to that in the overall population.

Pooled PD-L1 test volume in (A) the overall population, and in patients with (B) lung cancer, (C) melanoma, (D) SCCHN and (E) UC. PD-L1, programmed death ligand 1; SCCHN, squamous cell carcinoma of the head and neck; UC, urothelial carcinoma.
The 22C3 assay was the most frequently used assay, making up 89% of all tests performed, and the number of 22C3 tests performed increased by approximately 10-fold over the study period (figure 3). Small increases were observed in the volume of the 28-8 and SP142 tests over the study period, but the number of tests performed remained low compared with that for 22C3.

PD-L1 assay-specific testing volumes for the 28-8, 22C3 and SP142 assays in the overall population. PD-L1, programmed death ligand 1.

Concordance between the 28-8 and 22C3 assays in matched sample pairs in the overall population using (A) Passing-Bablok analysis. Passing-Bablok regression with PD-L1 28-8 as reference: slope=1, intercept=0. Identity line (dashed) and regression line (solid) are coincident in the figure. Dashed grey line indicates PD-L1 expression of 50% in the left panel. Symbol size scaled by sample size as indicated in the figure key. Spearman’s correlation=0.97 (95% CI 0.97 to 0.97). (B) Bland-Altman analysis. Solid line indicates the median (0.0) and the dashed lines represent the lower 2.5th and upper 97.5th percentiles for the difference between both readings (97.5% CI 10; 2.5% CI −20). Symbol size scaled by sample size as indicated in the figure key. N=3050. PD-L1, programmed death ligand 1.
Test concordance
A strong correlation between the 28-8 and 22C3 assays was observed in the overall population, with a Kendall’s tau correlation of 0.936 (95% CI 0.928 to 0.944) and a Spearman’s correlation of 0.97 (95% CI 0.97 to 0.97) (figure 4 and online supplementary table 1). Bland-Altman analysis demonstrated agreement between assays, with the differences in PD-L1 expression in matched samples clustered around 0% difference. PD-L1 IHC scores for the 28-8 and 22C3 assays were identical for 82% of matched samples, and the difference between PD-L1 IHC scores for the two assays was ≤10% for 95% of matched samples. PD-L1 expression was lower for the 22C3 assay than for the 28-8 assay in 5.8% of tests, and greater in 12.5% of tests. OPA, PPA and NPA were >95% with both the 28-8 and 22C3 assays as reference at the 1% cut-off for tumour cell PD-L1 expression (table 2). OPA between the 28-8 and 22C3 assays was consistently >95% over a range of PD-L1 expression cut-offs (1%, 5%, 10%, 25% and 50%; Cohen’s kappa 0.93–0.94; online supplementary table 2).
Agreement between the 28-8 and 22C3 assays in matched sample pairs* in the overall population at the ≥1% tumour cell PD-L1 expression cut-off
Analytical concordance in matched pairs of lung, melanoma, SCCHN and UC samples (Kendall’s tau correlations of 0.92–0.98) was consistent with concordance in the overall population, as was concordance in the most frequently biopsied sites with matched sample pairs (bone, brain, lung, liver, lymph node and pleural fluid; Kendall’s tau correlations of 0.92–0.97; online supplementary table 1). Agreement between the 28-8 and 22C3 assays was high across all tumour type subgroups (table 3).
Agreement between the 28-8 and 22C3 assays in matched sample pairs* from patients with lung cancer, melanoma, SCCHN and UC at the ≥1% tumour cell PD-L1 expression cut-off
Test failure rates and TAT
Test failure rates were low in the overall population and remained generally stable over the period from Q1 2016 to Q1 2018 (online supplementary figure 2). Patterns of test failure in the individual tumour-type subgroups were consistent with the overall population (data not shown). TAT in the overall tumour population initially increased as test volume increased, and stabilised at approximately 3 days (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PD-L1 test volume and TAT in the overall population. PD-L1, programmed death ligand 1; TAT, turnaround time.
Discussion
This analysis of 62 180 PD-L1 tests performed on biopsy samples from 55 652 patients tested at a single reference laboratory demonstrated an approximately 10-fold increase in PD-L1 test volume from October 2015 to March 2018. This pattern was generally consistent across all four tumour types examined (lung, melanoma, SCCHN and UC). Despite the increased use of PD-L1 tests, test failures decreased from 9.4% at the beginning of the study, after which the proportion of test failures remained low, ranging between approximately 3% and 6% over the period from January 2016 to March 2018. Average TAT varied between 2 and 4 days. These data suggest that PD-L1 test performance and TAT were not markedly affected by increases in the volume of tests performed at NeoGenomics Laboratories.
The majority of PD-L1 tests performed at NeoGenomics Laboratories were carried out with the 22C3 assay, and the sharp increase in testing volume after Q3 2016 in the lung cancer subgroup coincided with key US FDA approvals for pembrolizumab in metastatic NSCLC.38 PD-L1 testing did not appear to be frequently requested for patients with melanoma, SCCHN or UC, which each made up approximately 1% or less of tests in this dataset. However, these data should be interpreted with caution due to the high proportion of samples in the dataset for which tumour diagnosis information was missing.
High concordance between the 28-8 and 22C3 assays was observed in the overall study population, with a Kendall’s tau correlation of 0.94 (95% CI 0.93 to 0.94). Concordance in the lung cancer, melanoma, SCCHN and UC subgroups (Kendall’s tau correlations 0.92–0.98) was consistent with that observed in the overall population, as was concordance in samples from the most frequent biopsy sites for which matched samples were available (Kendall’s tau correlations 0.92–0.97). The concordance results from this study are consistent with, and add to, the literature showing good concordance between the 28-8 and 22C3 assays in lung cancer25 26 39–43 and UC.44 45 Furthermore, data supporting concordance between the 28-8 and 22C3 assays in melanoma and SCCHN may be of particular relevance because concordance in these tumour types has not been widely reported. Data from pleural fluid biopsies were included in this analysis because they represent one of the most common biopsy sites in patients with lung cancer or lung metastases. Similarly, bone is a frequent site of metastasis in many tumour types.46 However, neither the 28-8 nor the 22C3 assays have been validated for assessment of PD-L1 expression in decalcified samples, fine-needle aspirates or cytology specimens, so care should be taken when comparing data from bone and pleural fluid biopsies with other concordance results.16 31 Further evaluation of PD-L1 assays in prospective clinical trials is required to validate the clinical utility of these assays in tumour and sample types for which they have not been approved.
It should be noted that the tumour types for which PD-L1 testing was approved and the PD-L1 expression cut-offs in use at the time our data were collected do not reflect the current landscape for approved PD-L1 tests. The licensed indication for pembrolizumab for the first-line treatment of patients with metastatic NSCLC was expanded to include all patients with PD-L1 expression on ≥1% of tumour cells in April 2019.47 Similarly, the licensed indication for pembrolizumab in SCCHN has also been updated since its initial approval in 2016, with pembrolizumab approved by the US FDA in June 2019 for the first-line treatment of patients with SCCHN whose tumours express PD-L1 at a combined positive score ≥1, as determined using the 22C3 assay.15 48 Finally, the product label for the 28-8 assay, which was approved as a complementary diagnostic for the assessment of PD-L1 expression at a cut-off of ≥1% in patients with melanoma during the testing period evaluated here, was revised in April 2019 to remove melanoma from the list of approved indications in which the assay could be used.18
This study is subject to a number of limitations related to its design and methodology, and the setting in which data were collected. Because samples were analysed at a single laboratory (with uniformity in pathologist training), the data may not fully reflect the interlaboratory variations in PD-L1 testing protocols and interobserver variations in test interpretation that would be experienced in a multicentre study.39 40 49–52 Limitations inherent in the use of real-world data include the use of ICD-9/10 information for establishing tumour type, which in our study led to the pooling of NSCLC and SCLC into a single subgroup due to the coding not providing sufficient detail to categorise these diagnoses separately. Furthermore, diagnosis information was missing for a substantial portion of the study population, limiting the ability of this study to assess tumour type-specific uptake of PD-L1 testing. Reasons for test failure were also unavailable, with specific information not recorded at the time of testing. PD-L1 testing performed using the SP263 assay was excluded from this study because this assay was not approved by the US FDA until May 2017.21 Analyses of concordance in the SCCHN and UC subgroups were also limited by the small sample sizes for these subgroups, although the observed concordance was consistent with that seen in the overall population. Despite these limitations, this study evaluated a large sample of patients and PD-L1 tests across a range of tumour types in a real-world setting, which supports the generalisability of these data.
Conclusion
In this study, analytical concordance between the 28-8 and 22C3 PD-L1 assays was high when tested in matched samples from a large cohort of patients across various tumour types. Concordance was also high when evaluated in subgroups based on tumour type and biopsy location. This finding highlights the utility of real-world data in evaluating diagnostic assay concordance. Furthermore, evaluation of PD-L1 test utilisation showed that test failure rates remained relatively low and TAT remained reasonable despite increases in PD-L1 test volume over the period analysed. These findings support the potential interchangeability of the 28-8 and 22C3 assays for evaluating tumour cell PD-L1 expression in patients with lung and other cancers, and provide context on the evolution of PD-L1 testing.
Take home messages
Approvals of immunotherapies targeting the programmed death-1/programmed death ligand 1 (PD-1/PD-L1) pathway across various tumour types have been accompanied by increased use of PD-L1 diagnostic assays to aid selection of patients for treatment.
Despite the large increase in volume of PD-L1 immunohistochemistry (IHC) tests performed, assay turnaround time remained reasonable and test failure rates were generally low over the period evaluated in this study.
Analytical concordance and agreement between the Dako PD-L1 IHC 28-8 and 22C3 pharmDx assays were high across all PD-L1 cut-offs assessed, both in the overall study population and in subgroups based on tumour type and biopsy site, supporting the potential interchangeability of these assays.
Acknowledgments
Writing and editorial assistance was provided by John Copier, PhD, and Jay Rathi, MA, of Spark Medica Inc, funded by Bristol-Myers Squibb Company. Statistical analysis was conducted by Derrick Gallagher, PhD, of BioStat Solutions Inc, funded by Bristol-Myers Squibb Company.
References
Footnotes
Handling editor Runjan Chetty.
Contributors DH, GK, JN, JWR and VC contributed to the design of the study. JWR and VC performed PD-L1 staining and interpretation. All authors contributed to data analysis and interpretation. All authors critically reviewed and approved the manuscript.
Funding This study was supported by Bristol-Myers Squibb Company.
Competing interests DH, EAP, JN and JP are employees of Bristol-Myers Squibb Company. GSK was employed by Bristol-Myers Squibb Company at the time of the study. JWR and VC are employees of NeoGenomics Laboratories Inc. DH, EAP, GSK, JN and JP hold stock and/or stock options in Bristol-Myers Squibb Company. VC holds stock options in NeoGenomics Laboratories Inc and owns stock in Seattle Genetics. JN owns stock in Merck, AstraZeneca, Bristol-Myers Squibb Company and GlaxoSmithKline.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Bristol-Myers Squibb Company's policy on data sharing can be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.