Article Text

Abstract
Background Coronavirus disease-2019 (COVID-19) has caused a great global threat to public health. The World Health Organization (WHO) has declared COVID-19 disease as a pandemic, affecting the human respiratory and other body systems, which urgently demands for better understanding of COVID-19 histopathogenesis.
Objective Data on pathological changes in different organs are still scarce, thus we aim to review and summarise the latest histopathological changes in different organs observed after autopsy of COVID-19 cases.
Materials and methods Over the period of 3 months, authors performed vast review of the articles. The search engines included were PubMed, Medline (EBSCO & Ovid), Google Scholar, Science Direct, Scopus and Bio-Medical. Search terms used were ‘Histopathology in COVID-19’, ‘COVID-19’, ‘Pathological changes in different organs in COVID-19’ or ‘SARS-CoV-2’. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 guidelines were used for review writing.
Result We identified various articles related to the histopathology of various organs in COVID-19 positive patients. Overall, 45 articles were identified as full articles to be included in our study. Histopathological findings observed are summarised according to the systems involved.
Conclusion Although COVID-19 mainly affects respiratory and immune systems, but other systems like cardiovascular, urinary, gastrointestinal tract, reproductive system, nervous system and integumentary system are not spared, especially in elderly cases and those with comorbidity. This review would help clinicians and researchers to understand the tissue pathology, which can help in better planning of the management and avoiding future risks.
- pathology
- molecular
- immunohistochemistry
- microscopy
- electron
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Coronavirus disease 2019 (COVID-19), which is zoonotic in origin and most commonly spread through respiratory droplets or aerosol transmission, has caused a big threat to mankind.1 The disease was originated in the seafood market of Wuhan, Hubei, China, in early December 2019 with clinical presentations greatly resembling viral pneumonia.2 This disease has affected most of the countries in the period of 2 months itself. The outbreak of COVID-19 has been declared a pandemic by World Health Organization (WHO) and presents a great challenge for the healthcare communities across the globe.
The presently identified causative agent for COVID-19, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), has shared 82% genome sequence similarity to previously identified SARS-CoV-1, which also originated in China in 2002.3 4 The structure of the enveloped single-stranded RNA virus consists of spike protein, which is mainly responsible for the pathogenesis in the human species. The spike protein of the virus, through its receptor binding domain (RBD) gets attached to a human cell surface receptor protein Angiotensin Converting Enzyme -2 (ACE-2), encoded by the ACE2 gene, followed by its priming through auxiliary protein TMPRSS2 (transmembrane protease, serine 2), a cell-surface protein that is expressed by epithelial cells of specific tissues including those in the aerodigestive tract. ACE-2, which acts as a viral host cell entry receptor, has ubiquitous distribution on the organs, therefore SARS-CoV-2 in severe cases causes a systemic disease, with possible involvement of the kidneys, the heart and blood vessels, the liver, the pancreas and also regulates alterations in circulating lymphocytes and the immune system.5–7 The maximum expression of the ACE-2 receptors according to the consensus dataset from the human protein atlas is found in small intestine, duodenum and colon followed by kidney, testis, gall bladder, heart, thyroid gland, adipose tissue, rectum and lungs.8
The lungs are affected the most, with patients presenting symptoms related to the respiratory system such as sore throat, fever, malaise, and respiratory distress, and in worst cases may proceed to respiratory failure. Mice-related studies show that there is no gender difference in ACE-2 activity in lungs and heart but an expression of ACE-2 is more in male kidneys as compared with female kidneys, making the males more prone to kidney-related disorders, due to SARS infection.9
The entry of virus in the host cells induces immune response with wide secretion of inflammatory cytokines and chemokines. Because SARS-CoV-1 and SARS-CoV-2 have the same mechanism of action, both can cause rapid production of multiple cytokines in body fluids following infection, leading to acute respiratory distress and multiple organ failure. This also explains why most patients with COVID-19 have mild symptoms at the onset of the disease, while conditions of a few affected patients are suddenly worsened after being diagnosed in hospital, which may be related to the body producing excessive cytokines after the disease, leading to ‘cytokine storm’ in the body.10 The association of viral infection with any comorbid conditions such as hypertension, diabetes and renal failure has shown more severe form of clinical presentations such as respiratory failure to multiple organ failure.8 9 To understand the effects, presenting symptoms and the pathophysiology of SARS-CoV-2 on various organs, it is of utmost need to understand the pathological findings related to the coronavirus disease, depending on the localisation of the ACE-2 receptors in various organs.
Materials and methods
Objective
Data on histopathological changes in different organs are still scarce, thus we aim to review and summarise the latest histopathological findings observed in different organs related to the infection following autopsy of patient’s corpse who died following SARS-CoV-2 infection.
Information sources and search strategy
Over the period of 3 months, the authors performed vast review of the articles. The search engines used included PubMed, Medline (EBSCO & Ovid), Google Scholar, Science Direct, Scopus and Bio Medical. Search terms used were ‘Histopathology in COVID-19’, ‘COVID-19’, ‘Coronavirus’, ‘Pathological changes in different organs in COVID-19’ or ‘SARS-CoV-2’, ‘Lung pathology in COVID-19’, ‘Liver pathology in COVID-19’, ‘Cardiac involvement in COVID-19’, ‘Kidney pathology in COVID-19’, ‘Neuropathology in COVID-19’, ‘Endothelium and COVID-19’ and so on. All the authors were asked to take one system and to extract all the data related to that particular system. Titles and abstracts were screened independently and reviewed with inclusion/exclusion criteria. After data extraction, findings were summarised and reported in table 1 according to the objective of the study.
Important histopathogical findings of systems/organs observed by authors in different studies
Protocol followed
Systematic review writing was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 guidelines (online supplementary table).
Supplemental material
Inclusion and exclusion criteria
Articles (original, review, case series, case reports, published and preprints) that reported histopathological findings of organs in patients with COVID-19 after autopsy or endoscopic biopsy, from 31 December 2019 to 15 June 2020, were included in the study. Exclusive articles of SARS and MERS related to histopathological findings and a very few studies on animal models related to the topic were also included. Articles that did not mention about histopathology of organs, unavailable full text, no target observations and other article types (letters, comments, news and so on) as well as studies reporting cases with incomplete information were excluded. As the study was a systematic review of the literature, institutional ethical committee approval and informed consent were not obtained as we limited our study to published information and human subjects were not involved directly.
Results and discussion
In this review, authors identified various articles related to the histopathology of different organs in COVID-19 positive patients. Overall, 45 articles were identified using different databases as full articles to be included in our study. Histopathological findings observed are summarised according to the systems involved.
Pathological features
The early pathological findings identified in the COVID-19 suggested that SARS-CoV-2 can widely spread in the epithelial lining of the respiratory tract, digestive tract, distal convoluted tubules of the kidney, the sweat glands of the skin and testicular epithelium including spermatogonia and sertoli cells. Now, it has been found that, in addition to respiratory transmission, the virus might also be transmitted through faeces, urine and skin. The new findings have also necessitated new ways to prevent the transmission of disease. Many studies on epidemiology and clinical characteristics of COVID-19 have been published but data on pathological changes in different organs are still scanty.11 Hence, the histopathological findings in details have been described below according to the body systems involved.
Histopathological findings in respiratory system
Patients with affected upper respiratory tract usually present with mild to moderate symptoms but patients with lower respiratory tract infection show features of pneumonia and land up with organ failure. The severity increases with presence of comorbidities like hypertension, chronic kidney disease, obstructive sleep apnoea and metabolic diseases like diabetes and obesity,11 12 and the pathological changes may even vary between right and left lung.11 Macroscopically, lungs appear congestive, with patches of haemorrhagic necrosis.11 Alveolitis with atrophy, vacuolar degeneration, proliferation, desquamation and squamous metaplasia of alveolar epithelial cells (figure 1A), with presence of exudative monocytes and macrophages (figure 2E) are prominent features microscopically. There may be presence of massive fibrinous exudate, multinucleate giant cells and intracytoplasmic viral inclusion bodies and presence of epithelial cells in the lumen suggesting necrotic changes (necrotising bronchiolitis).11 There may be presence of diffuse alveolar damage (DAD), hyaline membrane formation and vascular congestion with occasional inflammatory cells, damaged pneumocytes with focal sloughing and formation of syncytial giant cells, along with focal infiltration of immune cells in the form of lymphocytes, monocytes and increased stromal cells (figure 1A).12 Additional findings included intra-alveolar haemorrhages, cluster or plug formation due to the accumulated fibrin (figure 1D) and degraded hyaline membrane remnants in some of the alveoli, type II pneumocyte hyperplasia, fibrinoid necrosis of the small vasculature and abundant intra-alveolar neutrophil infiltration (suggestive of superimposed bacterial infection) leading to bronchopneumonia (figure 1F).5 There may be presence of patchy and sparse chronic inflammation, composed mainly of lymphocytes, along with thrombi in branches of pulmonary artery and focal areas of congestion in alveolar septal capillaries along with septal capillary injury with mural and luminal fibrin deposition.10 13 Inflammatory oedema in the respiratory mucosa6 along with CD3+, CD4+ T cells, CD20+ B-lymphocytes and presence of CD68+ macrophages highlight the presence of inflammatory changes.13 There is also evidence of significant deposits of terminal complement components C5b-9 (membrane attack complex), C4d, and mannose binding lectin (MBL)-associated serine protease (MASP)-2, in the microvasculature, consistent with sustained, systemic activation of the alternative and lectin-based complement pathways.14 Pneumocytes may contain the virus within the cytoplasm and may show nucleomegaly and prominent nucleoli with small basophilic and larger eosinophilic cytoplasmic inclusions. Ultrastructural examination can reveal more details regarding the viral particles. Type II pneumocytes harbour numerous autophagosomes, characterised by double membranes and presence of organelles, in the cytoplasm (figure 2). These autophagosomes which contain viral aggregates, may also be present in tracheal epithelial cells and within the extracellular mucus in the tracheal lumen.5 Presence of virus particles has been shown by immunohistochemical staining using monoclonal antibody against SARS-CoV-2 nucleocapsid protein (figure 2C).15

Histopathological changes in lungs of COVID-19 patients. (A) Infiltration of lung tissue by mononuclear inflammatory cells, along with desquamation of alveolar epithelium and formation of hyaline membrane (arrow). (B) Hyaline membrane formation with no signs of inflammatory cell infiltrate. (C) Interstitial thickening with hyperplasia of type II alveolar epithelium. (D) Red blood cells present in alveolar lumen (asteriskd) along with formation of fibrin plugs. (E) Diffuse hyperplasia of type II alveolar epithelium and presence of fibrinoid vascular necrosis (inset). (F) Infiltration of inflammatory cells, predominantly neutrophils into the alveolar lumen,indicative of broncho-pneumonia. (Courtesy: Tian S, Xiong Y, Liu H, Niu L, Guo J, Liao M, et al. Pathological study of the 2019 novel coronavirus disease (COVID) through postmortem core biopsies. Mod Pathol. 2020 Apr 14;1–8.)
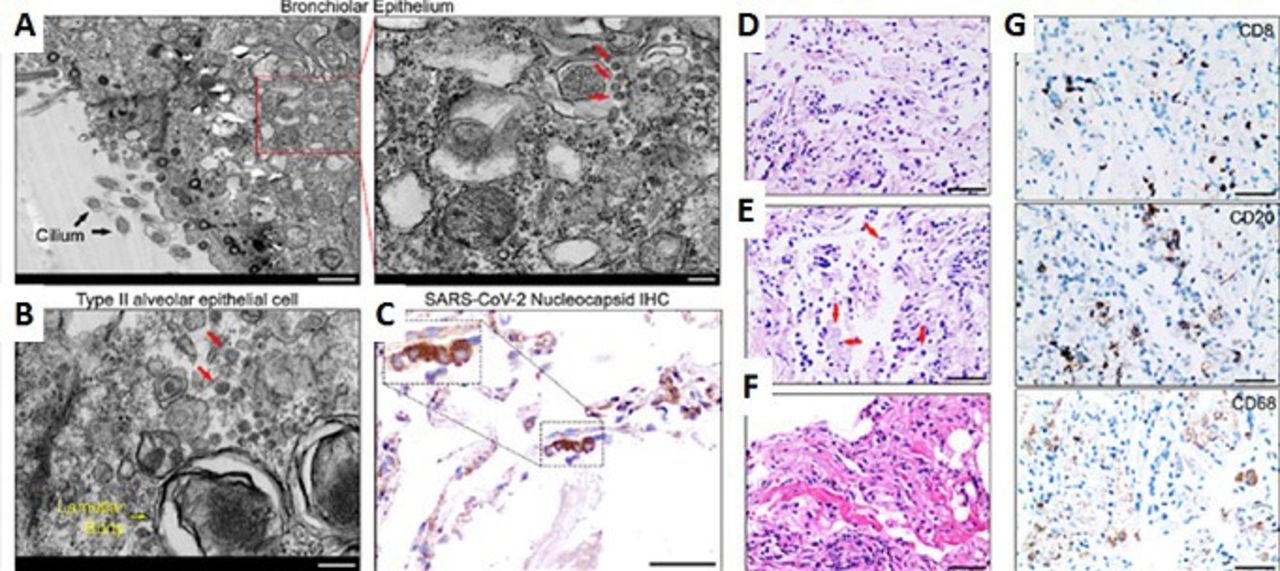
Histopathological changes in lungs of COVID-19 patients. (A) Ultrastructure of an epithelial cell of a bronchiole. Left panel shows organelle within epithelial cell while right panel shows viral particles. (B) Ultrastructure of a type II pneumocyte shows presence of organelle (yellow arrow) and viral particles (red arrows). (C) Positive (dark brown signals) SARS-CoV-2 nucleoprotein (N) in pulmonary tissue, confirmed by immunohistochemistry (IHC) and nuclei counter stained with hematoxylin. Inset shows magnified selected area. (D) Enlarged epithelial cells with areas of desquamation, stained with H & E. (E) Alveoli shows signs of exudation and infiltration by macrophages along with monocytes. (F) Formation of hyaline membrane within the lung tissue. (G) Infiltration of lung tissue with immune cells, which, immunohistochemically detected as CD68+ macrophages, CD20+ B cells, and CD8+ T cells. Scale bar: 50 μm.(Courtesy: Yao X-H, He Z-C, Li T-Y, Zhang H-R, Wang Y, Mou H, et al. Pathological evidence for residual SARS-CoV-2 in pulmonary tissues of a ready-for-discharge patient. Cell Res. 2020;30(6):541–3.)
Most of the histopathological findings are similar to those described in severe acute respiratory syndrome corona virus-1 (SARS-CoV-1) and Middle East respiratory syndrome coronavirus (MERS-CoV).16 These data suggest similarities in the pathogenesis and the mechanisms of tissue damage in lung tissue and inflammatory response to coronavirus infections, highlighting that the successful methodology in managing SARS and MERS could be referred to patients with COVID-19. Microscopic study of the COVID-19 lung tissue raises a possibility that nasopharyngeal swab showing negative result might not reflect the actual viral load in lung tissue.13 This study is important for the clinicians and virologists dealing with patients with COVID-19 as this study provides the pathological evidence for residual virus in the lungs for a patient with three consecutive negative PCR test results for the virus. Hence, PCR detection of SARS-CoV-2 nucleic acid on bronchoalveolar lavage fluid, extension of quarantine time and timely follow-up medical examination on discharged patients, especially older or immunocompromised patients, should be preferred.
Histopathological findings in urinary system (kidney)
ACE-2 is found to be upregulated in patients with COVID-19, and immunostaining with SARS-CoV-2 nucleoprotein antibody is positive in tubules. In addition to the direct virulence of SARS-CoV-2, factors contributing to acute kidney injury (AKI) includes systemic hypoxia, abnormal coagulation and possible drug or hyperventilation-relevant rhabdomyolysis.17 In some patients, pigmented casts is observed to be associated with high creatine phosphokinase levels possibly representing rhabdomyolysis.18
Clinically, the incidence of AKI in COVID-19 varies from 0.9% to 29%12 with new onset proteinuria. Microscopic changes in adult may range from diffuse proximal tubule injury with loss of brush border, non-isometric vacuolar degeneration to even frank necrosis.17 Other changes seen are swollen glomerular endothelial cells with small amount of protein exudate in the balloon cavity, and presence of thrombus in the capillaries, tubular epithelial cell oedema, vacuolar degeneration (figure 3A,B),18 with occasional cellular swelling and oedematous expansion of the interstitial spaces in distal collecting tubules and collecting ducts.15 Non-specific fibrosis along with lymphocytic infiltrates may be found beneath the renal capsule.15 Absence of interstitial haemorrhage or vasculitis differentiates this type of tissue injury from other causative factors like Hanta virus or injury by anti-neutrophil cytoplasmic antibodies.15 16 There can be presence of prominent erythrocyte aggregates, obstructing the lumen of capillaries, without platelet or fibrinoid material, with occasional hemosiderin granules and pigmented casts (figure 3E,F). Electron microscopic (EM) examination shows clusters of viral particles with distinctive spikes, in the tubular epithelium and podocytes.14

Histopathological changes in kidneys of COVID-19 patients (A) Epithelium of proximal convoluted tubules shows decreased/loss of the brush border. (B)Tubular epithelial cells show vacuolar degeneration (arrows), leading to collection of necrotic debris in the lumen (asterisks). Blocked peritubular capillaries due to erythrocytic aggregates (arrowheads). (C,D) Inflammatory cells (arrowhead) infiltrate the tubules and arcuate artery (arrows), Bacterial foci (asterisks) is also observed. (E,F) Tubular deposition of hemosiderin granules, calcium deposits (arrowhead) and pigmented cast (arrow). (G,H) Glomeruli show ischaemic contraction (arrows) and fibrin thrombi (arrowhead). Bowman’s space show presence of leaked accumulated plasma; hematoxylin and eosin. Bars = (F) 50 μm, (A–C, E, G, H)100 μm, and (D) 250 μm. (Courtesy: Su H, Yang M, Wan C, Yi L-X, Tang F, Zhu H-Y, et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020 Jul;98(1):219–2.)
Microscopic changes associated with the comorbid conditions such as diabetes and hypertension show characteristic findings in glomeruli, which include nodular mesangial expansion and hyalinosis of arterioles (associated with diabetic nephropathy) and arteriosclerosis of medium-sized arteries with ischaemic glomeruli.17Occasional findings include segmental fibrin thrombus, podocyte vacuolation, focal segmental glomerulosclerosis and shrinkage of capillary loops with accumulation of plasma in Bowman’s space (ischaemic changes)(figure 3G,H).18
Histopathological findings in digestive system (liver)
Although microscopic changes of hepatic tissue in COVID-19 have not been reported much, hepatic injuries cannot be ignored as the ACE-2 receptors have also been detected in the hepatobiliary system where cholangiocytes (59.7%) showed higher expression of ACE-2 cell surface receptor compared to hepatocytes (2.6%).19 Considering the fact that cholangiocytes expressed ACE-2 in the same manner as the type-2 alveolar cells, there is every possibility for the liver to be a potential target for SARS-CoV-2.19 Besides, concomitant use of medications also has effect on the hepatobiliary system. Hepatic injury mostly occurs in those with moderate to severe illness.20
Hepatic cell degeneration and focal necrosis in addition to presence of some biliary plugs in the small bile duct21 has been observed in light microscopic study. Although endothelial cells show positive ACE-2 expression, the endothelial lining of the liver sinusoids may be negative for ACE-2 along with Kupffer cells and hepatocytes.22 However, it cannot be denied that apart from the SARS-CoV-2 infection, parallel use of hepatotoxic drugs, pre-existing chronic liver disease and COVID-19 related hyperinflammatory conditions can lead to hepatic injury, particularly when the patient is in hypoxic state.
Microscopically, a liver, injured due to SARS-CoV-2 infection, may show signs of cirrhosis and regeneration with macrovesicular steatosis and glycogen accumulation in the liver cells along with atypical lymphocytic infiltration in the portal tract (figure 4A,B). Sinusoidal dilatation in zone 3, mild lymphocytic infiltration and patchy hepatic necrosis have also been observed in the area of portal triad and centrilobular areas20 (figure 4E,F).
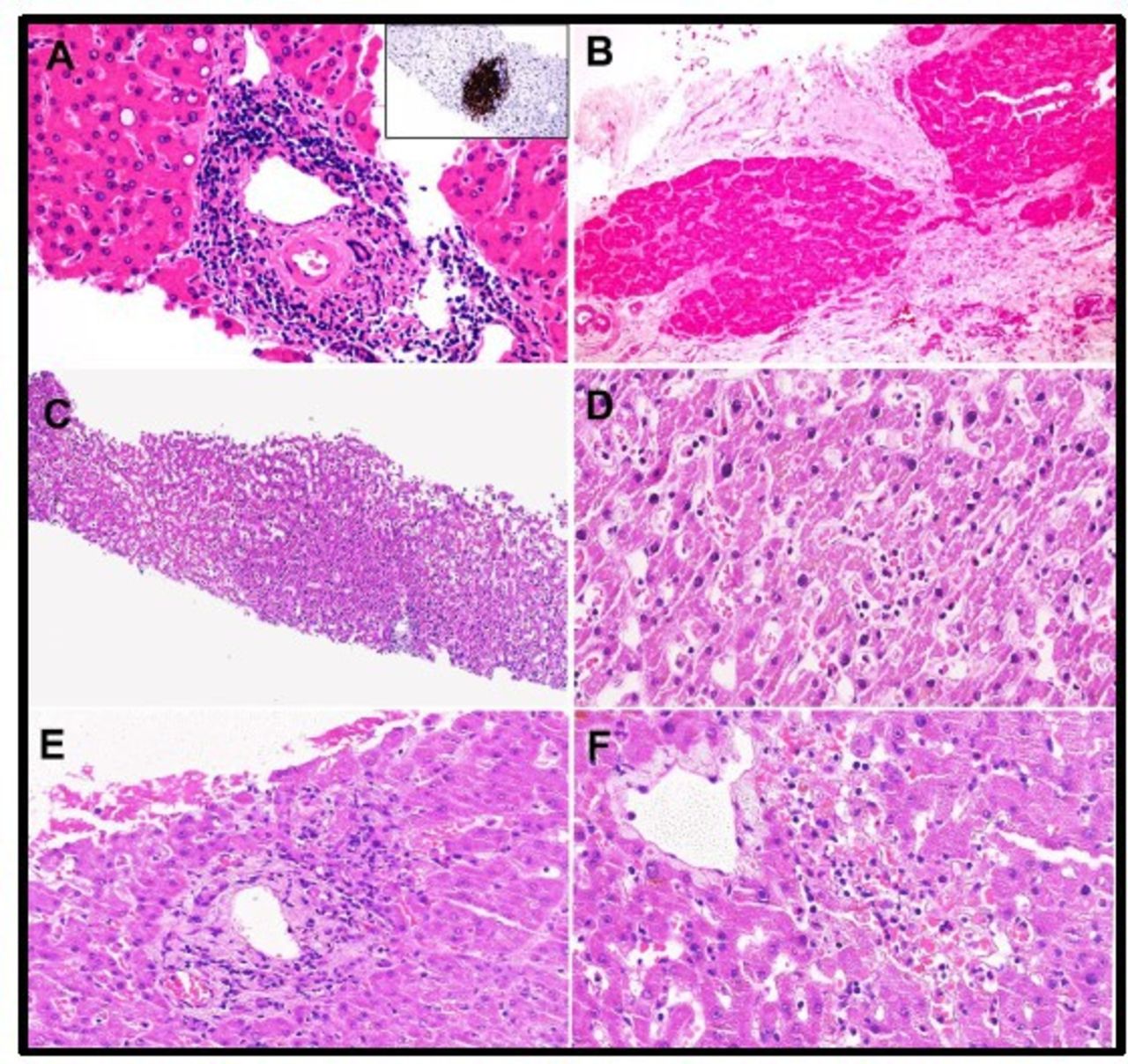
(A) Hepatocytes showing glycogenated nuclei and atypical small lymphocytes densely infiltrating the area of portal triad and showing CD20 positivity (inset). Dense portal infiltration by atypical small lymphocytes (inset: CD20 immunostaining) and focal glycogenated nuclei in hepatocytes have also been observed. (B) Hepatic nodules showing fibrosis, indicative of chirrosis.Cirrhotic nodules with thick fibrosis. (C) Hepatic sinusoids are dilated and filled with lymphocytes.Mild sinusoidal dilatation with increased lymphocytic infiltration. (D) High power view showing sinusoidal lymphocytes. (E,F) Periportal and centrilobular areas show necrosis, indicative of injury. (Courtesy: Tian S, Xiong Y, Liu H, Niu L, Guo J, Liao M, et al. Pathological study of the 2019 novel coronavirus disease (COVID) through postmortem core biopsies. Mod Pathol. 2020 Apr 14;1–8.)
Histopathological findings in other parts of digestive system (gastrointestinal tract)
Common gastrointestinal symptoms with which COVID-19 positive patients presented were diarrhoea, decreased appetite, nausea, vomiting, abdominal pain and gastrointestinal bleeding during the onset and subsequent hospitalisation.12
There are pieces of evidence of stenosis of the small intestine and segmental dilatation along with varying degrees of degeneration, necrosis and shedding in the gastrointestinal mucosa.23 Gastric tissue may show epithelial degeneration, necrosis and shedding of the mucosa with the presence of dilated and congested small blood vessels in lamina propria and submucosa along with infiltration of lymphocytes, monocytes and plasma cells. Endocrine pancreas may show evidence of tissue degradation.21 However, mucosal epithelial cells of the gastrointestinal tract may be apparently normal with occasional inflammatory infiltrates.24
Histopathological findings in cardiovascular system
Cardiac pathology
Viral infections being one of the most common causes of infectious myocarditis, cardiac involvement by SARS-CoV-2 cannot be ruled out.25 Endomyocardial biopsy from a 69-year-old COVID-19 positive patient, who died of septic shock, depicted low-grade myocardial inflammation and viral particles in the myocardial interstitial cells but not in cardiomyocytes or endothelial cells.26 However, involvement of cardiomyocytes cannot be ruled out as there are reports of hypertrophied cardiomyocytes along with inflammatory infiltrates, focal oedema, interstitial hyperplasia, fibrosis, degeneration, necrosis and signs of lymphocytic myocarditis.18 Besides ultrastructural changes like swelling of myocardial fibres, myocardium also shows presence of CD4 T cells along with other inflammatory infiltrates. However, pre-existing morbidity cannot be ruled out like hypertension-associated myocardial hypertrophy and past ischaemic injury.5 9 21
Endomyocardial biopsy from non-ischaemic heart showed endocarditis and inflammation of interstitial tissue and viral particles have been observed in interstitial cells with damaged cell membrane, but myocytes were apparently normal with no viral particles.26 Viral particles may be absent while other signs of inflammation may be present within the cardiac tissue like leucocyte infiltration and presence of CD4+ T cells22 23 indicating indirect injury to the cells by the virus.
Blood vessels
Due to the presence of ACE-2 receptor in the vascular endothelial cells, these are easy target for the SARS-CoV-2 virus.22 Studies show presence of viral inclusions along with inflammatory cells and apoptotic bodies in the endothelial cells.24 There are pieces of evidence of oedematous changes in alveolar capillaries and small vessels with the presence of fibrin thrombi, neutrophils and CD61+ megakaryocytes.27 Histological findings in purpuric papulovesicular rash of skin showed dense perivascular lymphocytic infiltration around the swollen blood vessels with extravasation of red blood cells.28 While punch biopsy from a case showed plump endothelial cells in lymphoplasmacytic infiltrate surrounded venules without intraluminal thrombi.29
Histopathological findings in nervous system
Neurological symptoms in COVID-19 have been frequently reported; however, the histopathological studies that investigated central nervous system (CNS) lesions are currently very limited.10 Dizziness and headache were most common CNS manifestations, while taste and smell impairment were the most common peripheral nervous system symptoms.30 Stroke, acute encephalopathy, convulsions, ataxia or nerve demyelination symptoms were occasional neurological presentations in some patients.31 Based on the analysis of spectrum of neurological symptoms, possible routes of CNS entry for SARS-COV-2 virus have been proposed through the hematogenous route by breaching blood–brain barrier or retrograde neuronal spread involving olfactory nerves.31 Olfactory route of viral entry into CNS were shown in mice models of SARS-CoV-1 and MERS-CoV which also showed widespread brain lesions following olfactory inoculation of the virus; however, no such evidence is specifically available at present for SARS-CoV-2.32 33 A recent postmortem examination study in patients with COVID-19 who displayed neurological symptoms showed widespread brain lesions.34 Autopsied brain tissue showed signs of acute hypoxic ischaemic injury like hyperaemia, oedema and neuronal degeneration.31 33 Neuroimaging scans (CT and MRI) for patients with COVID-19 presenting with acute neurological symptoms showed signs of ischaemia and/or haemorrhage, and enhanced cortical/subcortical grey matter and fibre tracts.35 SARS-CoV-2 RNA was detected in the brain tissue and cerebrospinal fluid of some autopsied patients with COVID-19 who had presented with neurological symptoms.36 37
Histopathological findings in genital system (testis)
Evidence has been found between the association of coronavirus family and orchitis in humans.38 ACE2 is present in seminiferous tubules, leydig cells, sertoli cells and spermatogonia.39 Binding of the virus with the testicular cells expressing ACE2 receptors not only damages the testicular tissue but also forms a potential safehouse for the virus. These hidden hotbeds for the virus may form an important cause for infertility worldwide.
Studies show hat sertoli cells are more susceptible than germ cells as more than 90% of the sertoli cells expressed ACE-2 receptors. Also, spermatogonia stem cells show higher expression of TMPRSS2 but lower expression of ACE-2, while the sertoli cells show higher expression of ACE-2 but lower expression of TMPRSS2, suggesting the mutual role of spermatogonia and somatic cells or sertoli cells for the invasion of the virus.40
All SARS-infected testes demonstrate histological findings with extensive germ cell destruction and decreased spermatogenesis in the seminiferous tubules. The basement membrane gets thickened with peritubular fibrosis along with leucocyte infiltration and vascular congestion in the interstitial tissue. Sertoli cells show swelling, vacuolation and cytoplasmic rarefaction (figure 5A,B). TUNEL assay shows increased apoptosis in the spermatogenetic cells and leydig cells of the SARS patients’ testes.40 One of the evident phenomena in the COVID-19 testis is leucocyte infiltration (figure 5D). These cells could affect the function of leydig cells and thus responsible for decreased production of testosterone (figure 5C). These infiltrated cells especially the lymphocytes and histiocytes, also damage the blood–testis barrier and destroy the seminiferous tubules directly(figure 5E,F).41

Pathological changes observed in testes from patients with COVID-19. (A,B) Defoliated and oedematous sertoli cells with vacuoles along with reduced spermatogenesis and scattered Leydig cells (arrow). (C) Tubular cells shows sloughing into the lumen (asterisks) indicative of injury. There is marked interstitial oedema. (D) Non-Covid testis with protracted disease showing interstitial edema with infiltration of inflammatory cells. (E) Immunohistochemical findings showing CD3-positive+T lymphocytes and (F) CD68-positive+ histiocytes. (Courtesy: Yang M, Chen S, Huang B, Zhong J-M, Su H, Chen Y-J, et al. Pathological Findings in the Testes of COVID-19 Patients: Clinical Implications. Eur Urol Focus.2020 May 31; pp 1–6.)
Similar to other viruses like HIV, mumps and hepatitis B virus, SARS-CoV-2 also may lead to activation of inflammatory cytokines, which may potentiate the autoimmune response. They may cause orchitis by several mechanisms, which may result in the testicular damage leading to infertility and sterility, which may further increase the chances of testicular tumours.38 Hence, it is a point of concern for patients suffering from testicular cancers with superadded SARS-CoV-2 infection. According to Song et al, no positive RT-PCR result was found in the semen or testicular biopsy specimen, hence suggesting that possibly it will not be transmitted through the sexual route.42
Histopathological findings in skin
The virus reaches the cutaneous tissue through the blood vessels. Since the endothelium abundantly expresses ACE-2, it can easily bind to the viral spike protein and facilitate viral invasion into the skin tissue thus initiating the pathogenesis. Inflammatory response caused by the viral invasion leads to inflammatory cell infiltrates, giving the pathological feature of vasculitis. Immune response leads to activation of Langerhans cells causing a cascade of reactions.43 With the usual common manifestations in COVID-19 positive cases, the dermatological manifestations may go unnoticed and a person may be a source of infection without his or her knowledge. As any other viral infection, the skin manifestations of a COVID-19 positive person may also show signs of erythematous rash, dermatitis, urticaria, chicken pox-like vesicles purpuric papulovesicular rash which may even be painful, pseudo-chilblains on fingertips and toes, macular/maculopapular exanthems, livedo reticularis lesions, petechiae and so on (figure 6). Since there is no correlation with disease severity or duration,44 an apparently normal person with positive test may come with only dermatological complaints, with the dermatological lesions mostly in trunk, hands and feet, as they are the most exposed regions of the body.45 Most of the skin lesions heal without any residual signs.45 Knowledge of skin manifestation may aid in early diagnosis of an asymptomatic COVID-19 patient.

Histopathological changes in skin of COVID-19 patients. (A) Arrow showing telangiectatic blood vessels in early exanthematous rash. (B) Epidermis (arrow) showing groups of Langerhans cells in the laterphase of exanthematous rash. Superficial dermis also shows perivascularinfiltration of lymphocytes. (C) An intraepidermal group of Langerhans cell seen in apapulo-vescicular rash. (D) Micrographic feature ina Maculo-papular erruption. (E) Capillary thrombosis (arrow) along with diffusehaemorrhage in an exanthemous (Courtesy: Raffaele Gianotti, Clinical and histopathological study of skin dermatoses in patients affected by COVID-19 infection in the Northern part of Italy. Letter to the Editor. Journal of Dermatological Science. G Model DESC 3594 No. of Pages 3.)
In the epidermis of the skin, the ACE-2 expression is oberved in the stratum basale. ACE- 2 expression has also been identified in smooth muscle cells of the skin along with the cells around the hair follicle.22 Although not very strong, the cytoplasm of the cells of sebaceous glands also expresses ACE- 2 along with its strong expression in the cells of eccrine glands.22 Dense perivascular lymphocytic and plasmacytic infiltration has also been observed around the swollen blood vessels with extravasation of red blood cells and intraluminal thrombi.28 29 Parakeratosis, acanthosis, dyskeratotic keratinocytes, necrotic keratinocytes, acantholytic clefts along with lymphocytes satellitisms have also been observed in biopsy samples of COVID-19 positive patients (figure 7).28 Presence of COVID-19 cutaneous manifestations may not be specific to SARS-CoV-2, but may be secondary to the various chains of events taking place due to the viral invasion. But keeping the features in mind will be a good approach towards determining the clinical value of the medical examinations required.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 7Histopathological changes in skin of COVID-19 patients(A) Acanthosis with presence of cleft (arrow) observed in skin of COVID-19 patients. Parakeratosis is also observed along with abnormal keratinization. (B) Localized necrotic keratinocytes (arrow) with abnormal keratinization InsetInset, with lymphocytic infiltration (arrow). (C) Acantholytic cleft with an adjacent apoptotic keratinocyte (arrow). (D) Pseudoherpetic features (arrow) along with apoptotic keratinocytes (double arrow). (Courtesy: Raffaele Gianotti, Clinical and histopathological study of skin dermatoses in patients affected by COVID-19 infection in the Northern part of Italy. Letter to the Editor. Journal of Dermatological Science. G Model DESC 3594 No. of Pages 3.)
Conclusions
Information regarding the pathological findings in COVID-19 is limited, although the virus mainly affects respiratory and immune systems, but other systems like cardiovascular, urinary (kidneys), gastrointestinal tract,reproductive (testes), and nervous system are not spared, especially in elderly patients, more often if comorbidities are also present. This review would definitely help clinicians and researchers to understand the tissue pathology, which can further help in better planning of the disease management and avoiding future health risks.
Take home messages
COVID-19 mainly affects respiratory and immune systems.
Other systems like cardiovascular, urinary, gastrointestinal tract, reproductive, nervous and integumentary systems are also not spared, indicating that it is a multi-system disease.
The elderly and those with comorbidities are affected more severely.
References
Footnotes
Handling editor Runjan Chetty.
AK, CK and KR contributed equally.
Contributors RM: Contribution in writing abstract, tables and histopathology of respiratory system and gastrointestinal system, and image collection. VD: Contribution in writing abstract, tables and histopathology of genital system, and arrangement of references using software. AK, CK and KR: Equally contributed in writing of histopathology of cardiovascular system, nervous system and skin, and contributed to tables and images of respective system.Final review is done by all authors individually.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.