Article Text

Abstract
Aims The aim of the study is to correlate p16Ink4a expression with the clinical courses of pleomorphic adenoma (PA), its malignant transformation (CaexPA) and treatment outcomes.
Methods Retrospective analysis (1998–2019) of 47 CaexPA, 148 PA and 22 normal salivary gland samples was performed. PAs were divided into two subsets: clinically ‘slow’ tumours characterised by stable size or slow growth; and ‘fast’ tumours with rapid growth rate.
Results Positive p16Ink4a expression was found in 68 PA and 23 CaexPA, and borderline expression in 80 and 20, respectively. All 22 (100%) normal salivary gland samples presented with no p16Ink4a expression. Significant difference in p16Ink4a expression was observed between normal tissue, PA and CaexPA (χ2 (4)=172,19; p=0.0001). The PA clinical subgroups were also evaluated separately, revealing additional statistical relations: ‘fast’ PA and CaexPA differed significantly in p16Ink4a expression (χ2 (2)=8.06; p=0.01781) while ‘slow’ PA and CaexPA did not (χ2 (2)=3.09; p=0.2129). 3-year, 5-year and 10-year survival among p16Ink4a positive CaexPA patients was 100%, 90.56% and 60.37%, respectively, and in CaexPA patients with borderline p16Ink4a expression was 90.0%, 73.64% and 22.20%, respectively. Statistically significant difference between expression pattern and survival rate was observed (F Cox test – F (16, 24)=2.31; p=0.03075).
Conclusions Our study confirms no p16Ink4a expression in normal tissue, but reveals differences in expression between ‘fast’ and ‘slow’ PA. We suggest that p16Ink4a overexpression is connected to PA proliferation and subsequent malignant transformation to CaexPA. Borderline p16Ink4a staining correlates with worse prognosis of CaexPA.
- immunohistochemistry
- salivary glands
- adenoma
- pleomorphic
- microarray analysis
- head and neck neoplasms
Data availability statement
All data relevant to the study are included in the article. Individual participant data will not be available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pleomorphic adenoma (PA) is the most common salivary gland neoplasm, accounting for approximately 70% of tumours.1 While PA is a benign lesion, its diverse clinical course, recurrences, and risk of malignant transformation comprise a medical challenge.1 2 PAs are usually well circumscribed and encapsulated, often with tongue-like protrusions or occasional satellite nodules.3 Morphological patterns vary with three components: epithelial, mesenchymal and mixed.4–6 Foci of squamous cells are an integral feature of PA; however, extensive squamous metaplasia is uncommon and can be easily misinterpreted as squamous cell carcinoma.7
In this paper, we present a new insight into a single histological unit: PA. Our 20-year experience of 1500 PAs and extensive observation of their individually variable disease courses has prompted us to distinguish two clinically divergent subsets: ‘fast’ and ‘slow’ tumours.8 While ‘fast’ PAs are characterised by a short medical history and rapid growth, ‘slow’ PAs demonstrate very stable biology and long-term growth. Progression, recurrence and malignant transformation are well-established PA behaviours, but the extremely fast growth of this benign tumour has always been a cause of concern for clinicians. Our team proved that the fast clinical course of PA has a great impact on further medical aspects.8 Thus, we undertake to search for immunohistochemical marker alterations among this single, clinically divergent histological unit.
Carcinoma ex PA (CaexPAs) arise from either primary or recurrent PAs, comprising 11.6% of all salivary gland malignancies,1 2 with a prevalence rate of 5.6 per 100 000.9 The clinical history is usually repetitive. After a long asymptomatic period, PAs start to grow rapidly and complaints such as pain, facial nerve palsy, and skin involvement may present.2 Longevity and recurrence seem to increase the risk of malignant transformation.9 10 This rate increases from 1.6% in tumours of <5 years, to 9.6% for tumours of >15 years.11 12 According to the latest WHO classification, CaexPA is no longer considered a stand-alone diagnosis.13 A substantial proportion of CaexPAs are now categorised as salivary duct carcinomas and myoepithelial CaexPAs.14
Little is known about the genetic background and markers that characterise the PA-CaexPA malignant transformation, and the scant available data are inconsistent.12 15 16 Because malignant transformation to CaexPA is mostly derived from the epithelial component of PA,17 it is rational to investigate p16Ink4a expression rather than other tumour suppressor proteins as their role in the development of head and neck squamous cell carcinoma (HNSCC) is proven. p16Ink4a is a tumour suppressor protein that is substantially downregulated in many malignancies.18 Almost 50% of human carcinomas demonstrate loss of p16Ink4a, for example, non-human papillomavirus (HPV)-related head and neck cancers, as well as pancreas, oesophagus, biliary tract, lung, liver, bladder, colon and breast carcinomas.18 On the other hand, p16Ink4a is also known to be overexpressed, namely in high-risk HPV-positive oropharyngeal and urogenital carcinomas.19–21 Oropharyngeal cancers (OPCs) comprise a subset of HNSCCs that arise from the oral cavity, oropharynx, hypopharynx, larynx and sinonasal tract and are anatomically limited to the base of the tongue, tonsils, posterior pharyngeal wall and soft palate.21 OPCs display two variant etiologies: tobacco and alcohol consumption for p16Ink4a-negative cancers, and high-risk HPV infection for p16Ink4a-positive cases.21 p16Ink4a investigation has become a practical alternative to oropharyngeal and urogenital HPV testing.22
The PA neoplastic transformation remains ambiguous, and its progression to its malignant counterpart derives from the epithelial cells of PA. Thus we decided to investigate p16Ink4a immunohistochemical expression in PA and CaexPA. One of the tasks we undertook was to search within the PA group for molecular alterations that may reflect the observed differences in PA proliferation rate. Second, we investigated whether the level of p16Ink4a immunohistochemical protein expression in CaexPA could constitute a prognostic factor of the outcome.
Thus, the main goal of our study is to examine p16Ink4a immunohistochemical protein expression as a biomarker which may have an impact on the rate of proliferation of PA and CaexPA, and their respective clinical courses.
Materials and methods
Multicentre retrospective analyses of 47 CaexPA from four university hospitals in Poland were performed. Formalin-fixed paraffin-embedded (FFPE) blocks and available clinical data were collected from archives dating from 1998 to 2019. The second examined group consisted of 148 parotid PA cases (FFPE blocks and clinical data). The reference group consisted of normal salivary gland tissue (NSGT) (22 FFPE blocks).
Patients diagnosed with CaexPA did not undergo surgery prior to malignant transformation, thus the PA material from these patients was unobtainable. In summary, analyses were performed on 47 samples of CaexPA, 148 of PA and 22 of NSGT.
All patients provided written informed consent for participation. Every patient participated at each stage.
All histopathological examinations were performed by two experienced pathologists. Tissue microarray paraffin blocks were cut on a manual rotary microtome (AccuCut, Sakura, Torrance, USA) into 4 µm thick paraffin sections, and placed on extra-adhesive slides (SuperFrostPlus, MenzelGlasser, Braunschweig, Germany). Immunohistochemistry (IHC) was standardised using a series of positive and negative control (HPV-positive SCC) reactions on FFPE tissue sections.
Immunohistochemical staining was performed using automated slide-processing system Benchmark GX Platform (Ventana Medical Systems, Tuscon, Arizona, USA) with primary mouse monoclonal antibody CINtec p16Ink4a antibody (clone E6H4, cat. no 705–4713; Ventana Medical Systems), and visualisation system UltraView DAB IHC Detection Kit (Ventana Medical Systems) in the procedure recommended by the manufacturer. Finally, the slides were dehydrated, cleared in a series of xylenes, and coverslipped with Tissu-Tek (Sakura, Japan).
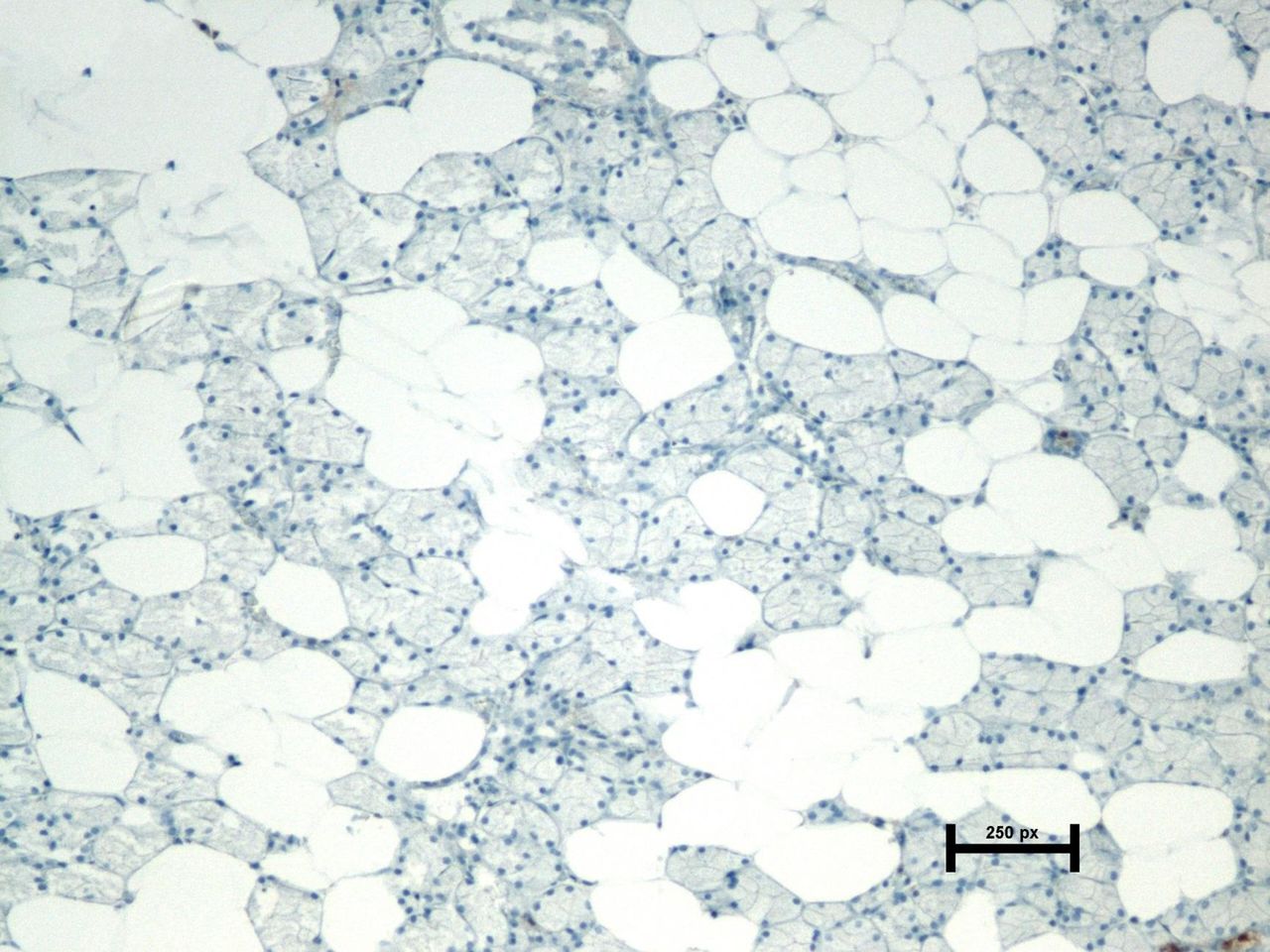
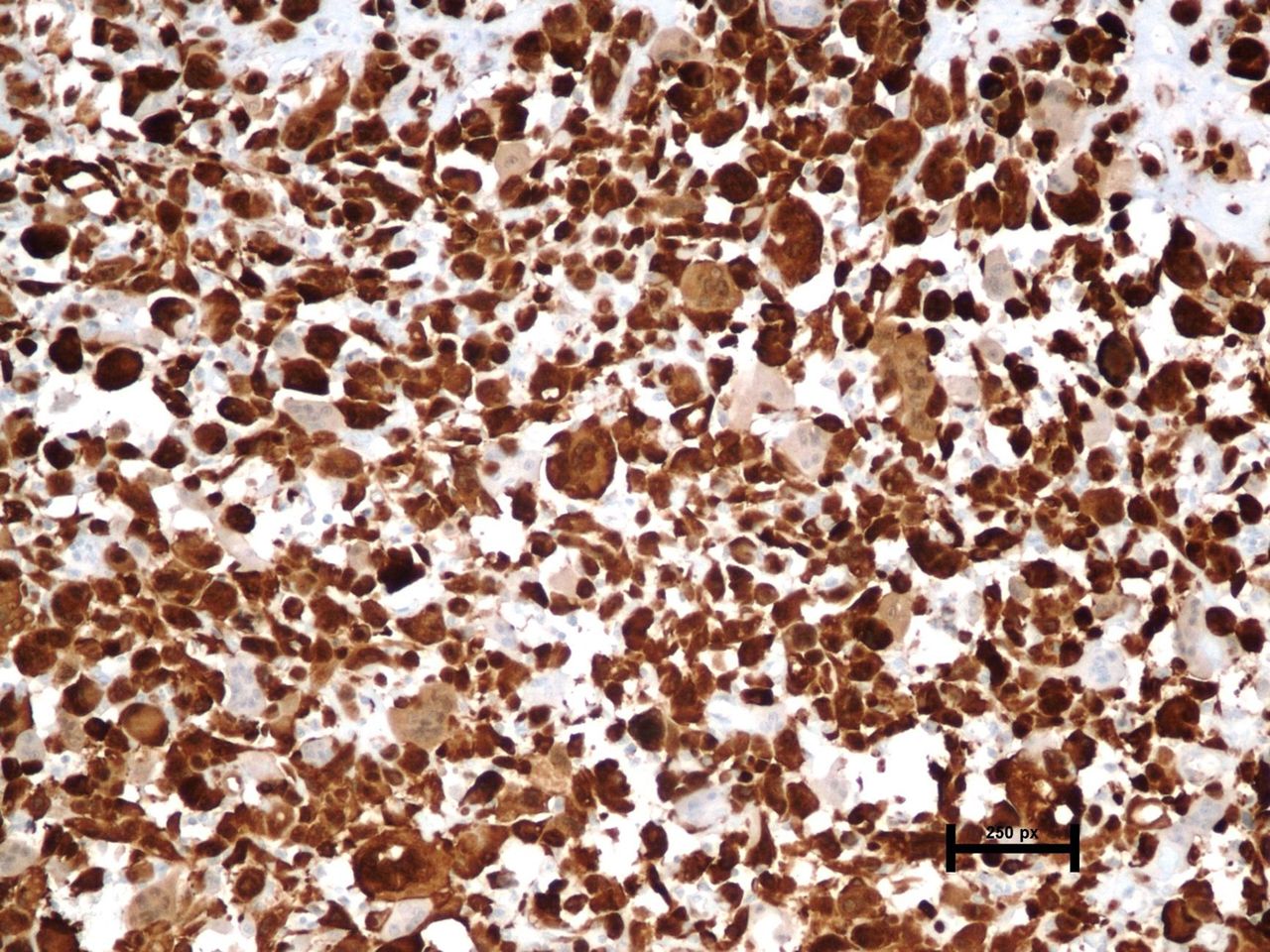
The pathologists independently evaluated the immunohistochemical expression of the examined antigens and were blinded to clinical and other data. In accordance with findings by Jordan et al, Bussu et al, and Cerezo et al, detailed in a systematic review by Prigge et al, we have scored the intensity of strong and diffuse nuclear and cytoplasmic staining of the p16Ink4a protein on a three-stage scale of p16Ink4a protein expression: 0—negative (no p16Ink4a expression) (figure 1), 1—borderline expression (1–69% of p16Ink4a-positive cells) (figure 2) and 2—positive expression (≥70% of p16Ink4a-positive cells)23–27 (figure 3). This division provided a comprehensive assessment of protein expression and a clearer understanding of the role of potential tumour markers in predicting outcome.15 16 Beside positive p16Ink4a expression, characteristic for high-risk HPV infection, we also implemented borderline expression of p16Ink4a following the publications presenting no evidence of HPV infection in the aetiology of salivary gland neoplasms.28 29
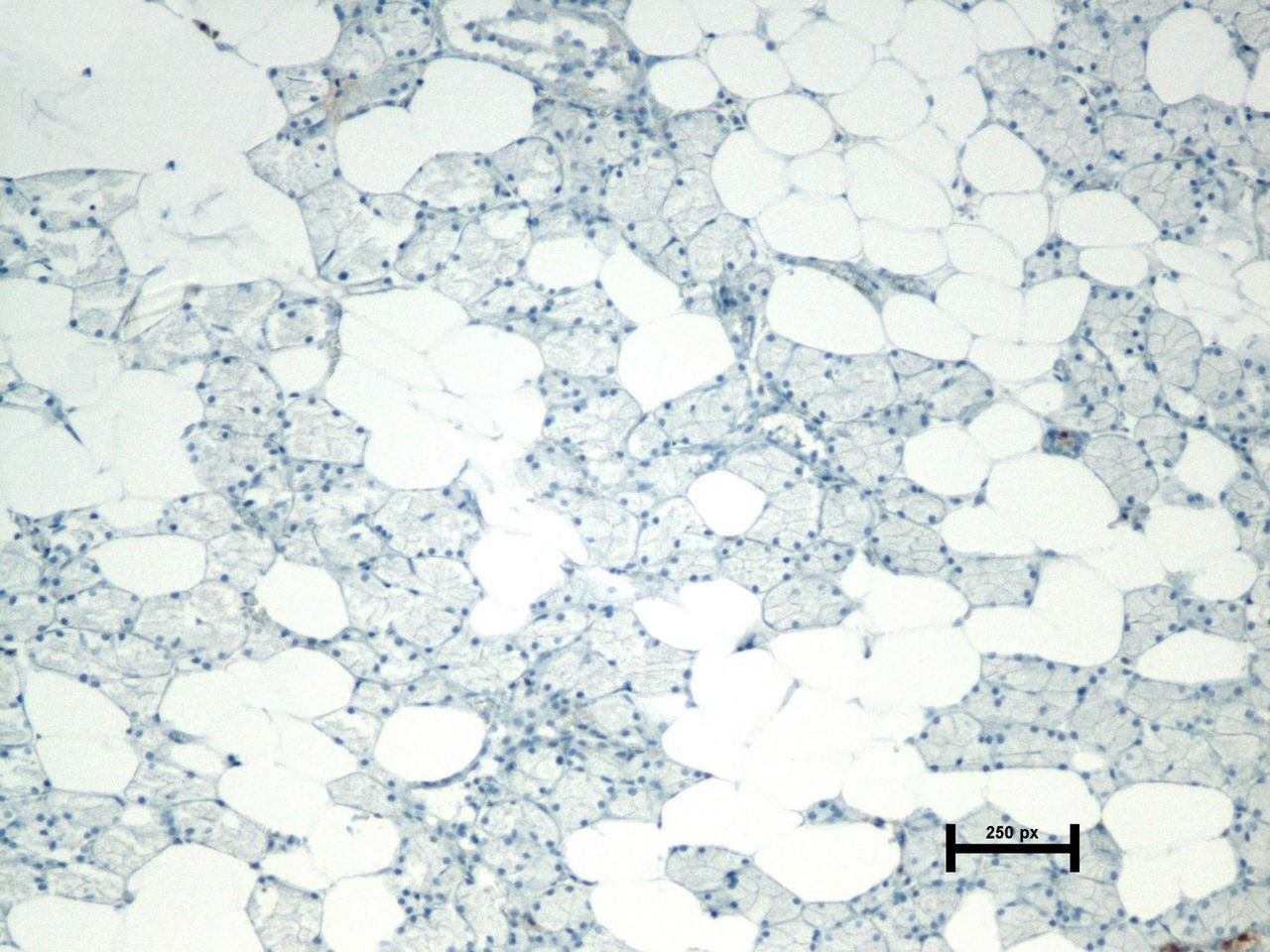
Expression of p16Ink4a protein in normal salivary gland—negative expression; nuclei counterstained with haematoxylin.

Expression of p16Ink4a protein in pleomorphic adenoma—positive expression; nuclei counterstained with haematoxylin.

Expression of p16Ink4a protein in carcinoma ex pleomorphic adenoma—positive expression; nuclei counterstained with haematoxylin.
The primary outcome measure was the evaluation of p16Ink4a expression in tumour tissue, with special regard to CaexPA and the PA group divided into two subsets of ‘fast’ and ‘slow’ tumours. The following outcome measures was p16Ink4a expression with regard to other variables: age, gender, time of complaints, recent acceleration in tumour growth, type of symptoms, recurrence, observation time, distant metastases and death. The final outcome measure was the correlation between p16Ink4a expression and survival of CaexPA.
Statistical analysis was performed using Statistica V.13. Descriptive statistics such as mean, minimum, maximum and SD were calculated for continuous variables. The χ2 test was used for categorical data. Student’s t-test and correlation coefficient were used for continuous data. The level of significance was set at p<0.05. For multiple comparisons, the Bonferoni correction was used on the level p<0.0167.
Patient characteristics
PA group
Of 148 patients with PA there were 46 men (31.08%) and 102 women (68.92%). Mean age was 44.93±13.71 SD years, range 18–78 years. Mean tumour size was 30.05±17.76 SD millimetres, range 10–110 millimetres. Mean duration of symptoms was 48.62±60.23 SD months. Ten patients with deep lobe tumours (6.76%) did not present any clinical manifestations. The maximum duration of symptoms was 240 months, obtained from the patient report. Thirty-four (22.97%) patients reported acceleration of tumour growth over six preceding months, compared with 114 patients (77.03%) who did not notice such a symptom.
Clinically ‘fast’ and ‘slow’ tumours
The PA group was divided into two subsets: ‘fast’ and ‘slow’ tumours.8 ‘Slow’ or ‘stable’ tumours demonstrated: duration of symptoms≥3 years; stable size of the tumour or its slow growth (<5% of tumour mass over the last 6 months); well-visualised tumour capsule in radiological investigation; and tumour homogeneity.30 ‘Fast’ or ‘unstable’ tumours demonstrated: duration of symptoms <3 years; >5% growth of the tumour mass within 6 months; and multipolycyclic budding outline, heterogenic echostructure and loss of capsule echogenicity in radiological investigation. The tumour must meet all clinical criteria: clinical history (cut-off 3 years) and tumour growth rate (cut-off 5% of tumour volume in the last 6 months), and at least one radiological criterion to be included in the study. Of 148 patients with PA, 52 (35.14%) were classified as ‘slow’ and 96 (64.86%) as ‘fast’.
Carcinoma ex PA group
Of 47 CaexPA cases, there were 25 men (53.19%) and 22 women (46.81%). Mean age of the patients was 55.32±11.59 SD years, range 31–81 years. Mean size of the tumour was 44.11±24.90 SD mm, range 9–160 mm. Mean duration of symptoms was 110.57±112.90 SD months, range 60–360 months. Mean time of patient observation was 69 months. All CaexPA cases had occurred in the parotid gland (47 patients, 100%). Thirty patients (63.83%) underwent extended surgery, and 17 (36.17%) underwent surgery restricted to the salivary gland. Thirty-nine patients (82.98%) received adjuvant treatment while 8 (17.02%) did not.
Results
There were 91 patients with positive p16Ink4a expression and 100 with borderline expression. Positive p16Ink4a expression was found in 68 PAs and 23 CaexPAs, and borderline expression in 80 and 20 cases, respectively. None of the 22 (100%) control cases of NSGT presented with p16Ink4a expression. No expression of p16Ink4a was found in the four remaining CaexPA patients (table 1).
Percentage distribution of p16Ink4a immunohistochemical staining in tissue material: NSGT, PA (including division into ‘slow’ and ‘fast’ subsets) and CaexPA
There was a significant difference in p16Ink4a expression between the three analysed groups (NSGT, PA and CaexPA) (χ2 (4)=172,19; p=0.0001). The level of p16Ink4a expression increased gradually through the neoplastic pathway from NSGT via PA to CaexPA. There was a significant difference in p16Ink4a expression between NSGT and PA (χ2 (2)=160.14; p=0.0001) with higher expression in PA. All analysed PAs showed increased p16Ink4a expression (borderline or positive), compared with NSGT where no cases demonstrated expression. There was a significant difference in p16Ink4a expression between PA and CaexPA (χ2 (2)=13.58; p=0.0011) with higher expression in CaexPA. There was also a significant difference in p16Ink4a expression between NSGT and CaexPA (χ2 (2)=48.20; p=0.0001).
Additionally, we analysed p16Ink4a expression in the course from NSGT to CaexPA via ‘slow’ PA, as well as from NSGT to CaexPA via ‘fast’ PA. Both ‘slow’ and ‘fast’ PA compared with unchanged tissue demonstrated a significant difference in p16Ink4a expression (p=0.00001). Analysis of p16Ink4a expression between ‘slow’ PA and CaexPA showed no differences (χ2 (2)=3.09; p=0.2129), while a significant difference between ‘fast’ PA and CaexPA was demonstrated (χ2 (2)=8.06; p=0.01781).
From these results, we conclude that the increased expression of p16Ink4a correlates with PA development, as well as with the malignant transformation from PA to CaexPA. The difference in p16Ink4a expression in the PA-to-CaexPA neoplastic pathway correlates with the clinical course of the benign PA precursor.
PA analysis
There was positive p16Ink4a expression in 68 (45.95%) cases and borderline p16Ink4a expression in 80 (54.05%).
We proved a significant difference in p16Ink4a expression in PA of variable clinical course (χ2 (1)=7.84; p=0.0051). Of the patients with positive p16Ink4a expression, slow growth of the tumour was reported in 32 (47.06%) cases, while fast growth was reported in 36 (52.94%). In patients with borderline expression, slow growth of the tumour was reported in 20 (25.00%), while fast growth was reported in 60 (75.00%). Borderline p16Ink4a expression in PAs is correlated with fast growth pattern. There was a significant difference in duration of symptoms between patients with positive and borderline p16Ink4a expression (Student’s t-test (146)=-2.00; p=0.0478). Mean duration of symptoms in patients with positive and borderline p16Ink4a expression was 59.24 and 39.60 months, respectively.
There was no significant difference between patients with positive and borderline expression of p16Ink4a in any other variables such as: age, gender, tumour size and recent growth acceleration (table 2).
Statistical analysis of p16Ink4a protein expression in reference to clinical data in the PA group
CaexPA analysis
Of the 47 patients with CaexPA, 24 (51.06%) presented with a typical malignant clinical course (facial nerve palsy, pain, skin redness or ulceration), while 23 (48.94%) reported a lump that imitated a benign lesion (asymptomatic swelling only). Positive expression of p16Ink4a was demonstrated in 23 (48.94%), borderline expression in 20 (42.55%) and no expression in 4 (8.51%) patients. There was no significant difference in p16Ink4a expression with regard to any of following variables: age, gender, tumour size, duration of symptoms, type of symptoms, recurrence and distant metastases (table 3).
Statistical analysis of p16Ink4a protein expression in reference to clinical data in the CaexPA group
CaexPA survival analysis
Fifteen (31.91%) patients developed recurrence, and distant metastases were observed in 20 patients (42.55%). Twenty-one patients died (44.68%) and 26 (55.32%) were living at the end of follow-up.
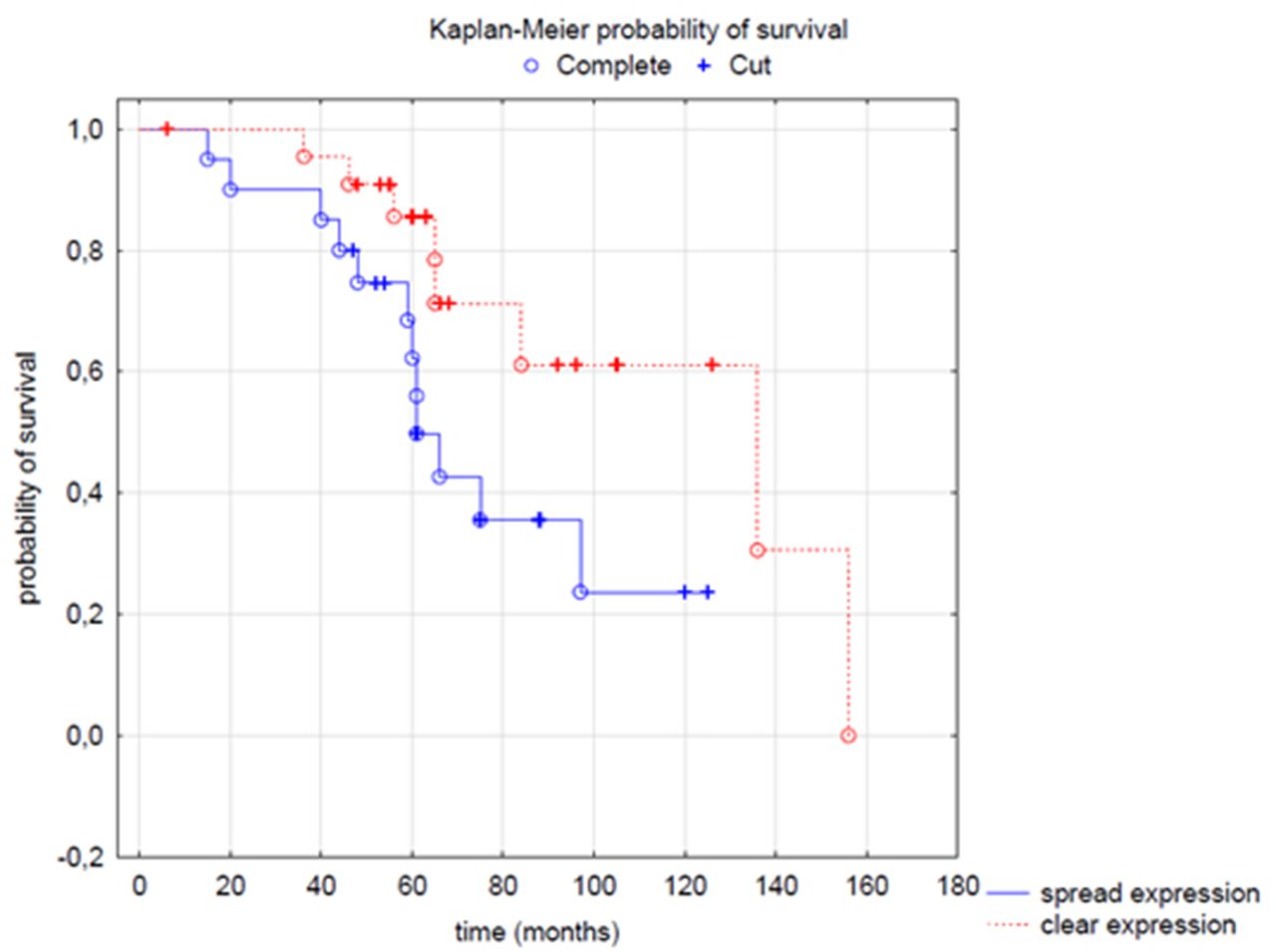
Three-year survival was 93.48%, 5-year survival was 74.76% and 10-year survival was 44.01% for the whole CaexPA group. In patients with positive p16Ink4a expression survival was 100%, 90.56% and 60.37%, respectively; in patients with borderline p16Ink4a expression, 90.0%, 73.64% and 22.20%, respectively; and in patients with no p16Ink4a expression, 100%, 75% and 0%, respectively. A significant difference in CaexPA survival was observed when patients with no p16Ink4a expression (4/47) were excluded from the analyses (F Cox test – F (16, 24)=2.31; p=0.03075). Patients with borderline p16Ink4a expression had worse 3, 5 and 10 years survival. Based on these results, we conclude that borderline p16Ink4a expression is related to bad prognosis (table 4, figure 4).
The percentage distribution of p16Ink4a immunohistochemical staining in the CaexPA group in reference to survival rate
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier probability of survival correlating p16Ink4a expression and CaexPA survival. CaexPA, carcinoma ex pleomorphic adenoma.
Discussion
Our main results are concerned with p16Ink4a expression in NSGT, PA and CaexPA. There are no studies in the available literature comparing p16Ink4a expression with the clinical data of PAs and CaexPAs, or the oncological outcome of patients with CaexPA. Thus we outline the following study aims: to identify p16Ink4a in tumour tissue and correlate its expression with the clinical course of PA with slow growth, PA with fast growth and CaexPA. p16Ink4a is expressed in various salivary gland tumours both benign (PA, Warthin’s tumour) and malignant (polymorphous low-grade adenocarcinoma, acinic cell carcinoma, mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma, salivary duct carcinoma),31 32 but whether p16Ink4a is involved in the rate of PA proliferation and its subsequent progression to CaexPA remains an open question.31 32
There have been several studies exploring p16Ink4a expression in PA and CaexPA, with contradictory results, but the data on CaexPA is restricted to a few isolated cases.12 15 16 The absence of p16Ink4a expression in NSGT was the important outcome that served as a benchmark for benign tumour testing. We proved a statistically significant difference in p16Ink4a expression in the course from normal tissue, via PA, to CaexPA, demonstrating a gradual increase of p16Ink4a expression in this pathway.
Currently, the only known pathomechanism of p16Ink4a-positive tumours is high-risk HPV infection. However, the literature does describe non-HPV-related malignancies demonstrating overexpression of p16Ink4a protein. Skálová et al conducted p16Ink4a IHC analysis and high-risk HPV DNA PCR of 55 benign and malignant salivary gland tumours and found that none of the p16Ink4a-positive cases demonstrated any evidence of high-risk HPV.28 An analogous phenomenon was described in HPV-negative laryngeal squamous cell carcinoma (LSCC) with p16Ink4a-positive IHC, where Larque suggested that CDKN2A mutations played a leading role in the aetiology.33 Regardless of the cause of increased p16Ink4a expression, both HPV-positive and -negative LSCCs demonstrating p16Ink4a immunopositivity were associated with better prognosis and greater sensitivity to radiotherapy than p16Ink4a-negative LSCCs.33 p16Ink4a overexpression is a proven positive prognostic factor in HNSCCs.33 Our analysis of p16Ink4a expression level, in relation to PA clinical course and CaexPA oncological outcomes, supports this hypothesis. Diffuse p16Ink4a expression correlates with a fast course of PA burdened with a higher risk of treatment failure,8 as well as a worse prognosis of patients with CaexPA.
The biology and tumourigenesis of non-HPV-related tumours in relation to p16Ink4a overexpression is a subject of ongoing research. Increased p16Ink4a expression in the HPV-independent pathway was confirmed by the presence of molecular disruptions in the p16Ink4a-Rb signalling pathway.34 35 The molecular basis of this mechanism is the deregulation of Rb activity.36 37 Loss of heterozygosity in the Rb gene results in an increase in p16Ink4a expression in neoplastic cells, resulting in uncontrolled cell proliferation.36 37 The literature reports that p16Ink4a function deregulation may occur through activation (overexpression) of the NF-κB factor.38
Our findings are partially consistent with Patel et al’s findings conducted on a comparable but smaller sample of 29 PAs and 14 CaexPAs.12 Their results did not reveal any expression of p16Ink4a in NSGT, and indicated a significant difference in p16Ink4a expression between NSGT and both PA and CaexPA. They did not prove any significant difference in p16Ink4a expression between PA and CaexPA, possibly because of their small cohort. There were also differences in the applied criteria of immunopositivity: both nuclear and cytoplasmic staining was considered, but altered levels of p16Ink4a expression were not differentiated.12 The levels of differentiation support the ability to compare p16Ink4a expression in PA with CaexPA. On the other hand, Tarakji et al 15 16 revealed a significant difference in p16Ink4a expression between NSGT and CaexPA; they, however, demonstrated higher expression in NSGT and lower in CaexPA. de Souza et al performed p16Ink4a nuclear expression analysis and revealed strong staining in recurrent PA and CaexPA, while PA was weakly staining or negative, suggesting that p16Ink4a may be involved in the recurrence and malignant transformation of PA.39 Others confirm p16Ink4a overexpression in various salivary gland lumps,32 and also show a significant difference in p16Ink4a expression between NSGT and both benign and malignant salivary gland tumours.31
An innovative approach in our work was to divide benign PAs into ‘fast’ and ‘slow’ categories according to clinical features. Our study has confirmed molecular differences between tumours that appear to be histologically identical. Borderline p16Ink4a expression correlates with ‘fast’ PA progression. Most importantly, the difference between CaexPA and ‘fast’ PA, when considered separately from PA as a whole, was statistically significant, while ‘slow’ PA was not. These results indicate that the difference in p16Ink4a expression in the neoplastic pathway between PA and CaexPA correlates with the clinical course of the benign PA precursor.
To summarise, we have successfully implemented the hypothesis of our work comparing the gradual stages of cancer transformation from NSGT, via clinically ‘slow’ and ‘fast’ subsets of PA, to CaexPA. Our results reveal that NSGT did not express p16Ink4a, and that the p16Ink4a expression level in PA correlates with slow or fast PA clinical behaviour. Moreover, the p16Ink4a expression level was revealed to hold prognostic value for patients with CaexPA. Borderline p16Ink4a expression is related to worse survival.
Take home messages
p16Ink4a expression gradually increases in the neoplastic pathway from normal salivary gland tissue via pleomorphic adenoma (PA) to carcinoma ex PAs (CaexPA).
p16Ink4a overexpression correlates with the proliferation of PA and subsequent malignant transformation to CaexPA.
There is a statistically significant difference in p16Ink4a expression among PA with variable clinical courses.
The level of p16Ink4a expression constitutes a prognostic value for patients with CaexPA.
Data availability statement
All data relevant to the study are included in the article. Individual participant data will not be available.
Ethics statements
Patient consent for publication
Ethics approval
Bioethical Resolution No. 704/18 of Poznan University of Medical Sciences was obtained.
References
Footnotes
Handling editor Runjan Chetty.
Contributors Conceptualisation, EB; methodology, MB, PK and AW, software, EB, KP; validation, MW, EB and KP; formal analysis, EB; investigation, EB, KP; resources, EB, KP; data curation, EB, KP, JC; writing—original draft preparation, EB; writing—review and editing, EB, JC, MW; visualisation, EB, KP; supervision, MW; project administration, MW; funding acquisition, EB.
Funding This study was funded by Poznan University of Medical Sciences (Grant No. 502-14-11081320-11154).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.