Article Text

Abstract
Objective: To evaluate the genetic influence of PvuII and XbaI polymorphisms of oestrogen receptor α (ORα) in patients with systemic lupus erythematosus (SLE) in Korea.
Methods: Genomic DNA from 268 female controls and 137 female SLE patients (41 childhood onset and 96 adult onset) were analysed using PvuII and XbaI restriction fragment length polymorphism. Comparison of the frequencies of alleles and genotypes was made in control and patient groups and in childhood onset and adult onset SLE subgroups.
Results: Although the Pp genotype occurred more often in SLE patients than in controls (pc = 0.017), ORα genotype distributions of adult onset SLE did not differ significantly from controls. The PP, Pp, and xx genotypes occurred less often in childhood onset SLE (pc = 0.0045, 0.0498, and 0.0255, respectively) than in controls. Additionally, the PP genotype was less common in childhood onset than in adult onset SLE (pc = 0.016). SLE patients with the PP genotypes were older at disease onset than those with the other genotypes (p = 0.001). Patients with the Xx genotype had an earlier onset of SLE than those with the xx genotype (p = 0.025). The frequency of the combined ppXx genotype was greater in childhood onset SLE than in controls (pc = 0.0009) or adult onset SLE (pc = 0.027). The same trend was supported by subgroup analyses according to age at menarche and logistic multivariate analyses.
Conclusions: ORα polymorphisms are significantly associated with the age at disease onset in Koreans with SLE.
- systemic lupus erythematosus
- oestrogen receptor α
- polymorphism
- PvuII
- XbaI
Statistics from Altmetric.com
Systemic lupus erythematosus (SLE) is an idiopathic systemic inflammatory disease with diverse manifestations. Although the aetiopathology of SLE is not clearly understood, sex hormones are considered to affect the pathogenic mechanism. Epidemiologically, a female predominance is consistently demonstrated—about 90% of adult SLE patients are female. The peak incidence of SLE occurs in the reproductive period, and a postmenopausal onset of SLE is relatively uncommon.1
Experimentally, the progression of lupus and mortality are different in female and male mice, and exogenous oestrogen reduces longevity and accelerates nephritis in the NZB/NZW lupus model.2 Oestradiol stimulates the production of autoantibody to dsDNA in peripheral blood mononuclear cells (PBMC),3 and decreases apoptosis of PBMC from SLE patients.4 In addition, oestrogen augments SS-A/Ro and SS-B/La antigen expression on the cell surface of human keratinocytes,5 and stimulates macrophages from SLE patient to produce IL-10, the levels of which increase in sera of SLE patients.6 Recently, it was reported that oestrogen increased calcineurin and CD40 ligand in SLE T cells.7 Some epidemiological studies have suggested that women taking postmenopausal hormone replacement or oral contraceptives could be at increased risk of developing SLE.8,9
Oestrogen acts through two nuclear receptors—ORα (oestrogen receptor α) and ORβ—and the activity of these receptors may affect the actions of oestrogen. PvuII and XbaI polymorphisms of ORα have been studied in many diseases, and there are reports that these polymorphisms are associated with breast cancer, endometrial cancer, generalised osteoarthritis, osteoporosis, and the effects of oestrogen replacement on lipid metabolism.10–,16
There are few studies of ORα polymorphisms in SLE,17,18 and ORα polymorphism in childhood onset SLE has never been reported. We hypothesised that ORα polymorphisms are associated with SLE, and we analysed PvuII and XbaI restriction fragment length polymorphisms (RFLP) of ORα in patients with childhood and adult onset of SLE in Korea.
METHODS
Study subjects
We recruited 137 female patients with SLE (mean age, 23.2 years (range 3 to 67); 41 with age at onset <16 years) and 268 sex and age matched controls (mean age, 31.4 years (range 3 to 70); 48 aged <16 years). Healthy adult controls were enrolled from subjects attending routine medical check ups; child controls were children admitted for elective surgery or transient acute infection. There was no significant difference in the allele and genotype frequencies of PvuII or XbaI RFLPs between adult and child control groups. SLE was diagnosed according to the criteria proposed by the American College of Rheumatology (ACR) in 1997.19 Childhood onset SLE was arbitrarily defined as lupus beginning before the age of 16 years, and patients with pre-menarche onset were those diagnosed with lupus before the menarche. Clinical and laboratory features were defined according to the criteria of the ACR and collected during the whole follow up period, or were derived from well documented medical records.
Only one patient had a family history of SLE. Among 64 SLE patients who underwent renal biopsy, 46 (71.9%) had diffuse or focal proliferative lesions. Neuropsychiatric manifestations other than seizures and psychosis included cerebrovascular accidents (3.6%), chorea (2.2%), cranial neuropathy (0.7%), aseptic meningitis (0.7%), and transverse myelitis (0.7%). Six patients (4.4%) had hypertension, and five (3.6%) had thyroid disease. Eight patients had overlap with Sjogren’s syndrome (4), rheumatoid arthritis or juvenile chronic arthritis (3), and juvenile dermatomyositis (1). The demographic and clinical features of the SLE group are summarised in table 1⇓. The only significant differences between manifestations of childhood onset and adult onset subgroups were mucocutaneous manifestations, proteinuria, and proliferative lupus nephritis.
Characteristics of the patients with SLE
DNA isolation and genotyping
Genomic DNA was extracted from the peripheral blood using the QIAamp® DNA blood kit (Qiagen, Valencia, California, USA). Polymerase chain reaction (PCR) primers for the restriction fragment length polymorphic site in ORα were designed as reported previously: forward, 5′-CTGCCACCCTATCTGTATCTTTTCCTATTCTCC-3′ and reverse, 5′-TCTTTCTCTGCCACCCTGGC-GTCGATTATCTGA-3′.11 Genomic DNA (100 ng) was amplified in 50 μl of buffer solution (20 pmol of each primer, 0.2 mM dNTPs, 2 mM MgCl2, and 2.0 U of Taq polymerase (Promega, Madison, Wisconsin, USA)). Thirty cycles of PCR were carried out as follows: denaturation at 94°C for 30 seconds, annealing at 55°C for 60 seconds, and extension at 72°C for 90 seconds. PCR products were digested using 20 U of either PvuII or XbaI restriction endonucleases (Promega) and electrophoresed on a 2.0% agarose gel. The presence of restriction sites for these endonucleases is indicated with a lower case letter (p or x, for PvuII or XbaI, respectively) and the absence of restriction site is indicated by an upper case letter (P or X).
Statistical analysis
Comparisons of the allele and genotype frequencies of patients and controls were made using the χ2 test or Fisher’s exact test as applicable. In case of multiple comparisons, the probability value (p) was corrected (pc) for the number of comparisons made, and results were considered significant at pc <0.05. Mean differences in continuous variables were evaluated using Student’s t test or one way analysis of variance (ANOVA) with Tukey’s multiple comparison tests. Polychotomous logistic regression analysis with a generalised logit model was conducted to test for an interaction between ORα polymorphisms and clinical manifestations in the patient groups. Variables with p or pc <0.05 from univariate analyses were considered as independent variables in the multivariate logistic regression model. Results were expressed as odds ratios (OR) with 95% confidence intervals (CI). All statistical analyses were done with SAS v8.1.
RESULTS
There was no significant difference in the allele frequency of PvuII or XbaI RFLPs between control and SLE groups. However, significantly fewer patients with childhood onset SLE had x alleles compared with the control subjects (p = 0.003, OR = 0.46 (95% CI, 0.27 to 0.80)) or adult onset SLE patients (p = 0.021, OR = 0.47 (0.25 to 0.90); table 2⇓). Additionally, there were significantly fewer SLE patients with pre-menarche onset who had x alleles compared with either the controls (65.6% v 83.2%, p = 0.0006; OR = 0.39 (0.21 to 0.70)) or the post-menarche SLE group (65.6% v 82.9%, p = 0.006; OR = 0.40 (0.20 to 0.78)).
Allele and genotype frequencies of ORα polymorphism in controls and SLE patients
The Pp genotype frequency was greater in SLE patients (pc = 0.017, OR = 1.79 (1.16 to 2.77)) and childhood onset SLE patients (pc = 0.0498, OR = 2.24 (1.09 to 4.64)) than in the controls. The PP genotype was significantly less common in childhood onset SLE than in the controls (pc = 0.0045, OR = 0 (0 to 0.63)) or adult onset cases (pc = 0.016, OR = 0 (0 to 0.71); table 2⇑). In addition, SLE patients with pre-menarche onset had a lower PP genotype frequency than the control group (pc = 0.021, OR = 0 (0 to 0.81)). However, there was no difference in the genotype frequency of PvuII between childhood onset SLE and child control subgroups. For the XbaI polymorphism, SLE patients did not show any difference from the control group in the distribution of xx, Xx, and XX genotypes. In the subgroup analysis, the xx genotype was significantly less common in childhood onset SLE than in the whole control group (pc = 0.026, OR = 0.42 (0.20 to 0.85)) or the child controls (51.2% v 77.1%, pc = 0.032, OR = 0.31 (0.11 to 0.85)). The SLE patients with pre-menarche onset had a lower frequency of the xx genotype (43.8% v control 71.7%, pc = 0.0039, OR = 0.31 (0.14 to 0.69); 43.8% v post-menarche group 71.4%, pc = 0.024, OR = 0.31 (0.13 to 0.76)), and a higher frequency of Xx genotype (43.8% v control 23.1%, pc = 0.034, OR = 2.58 (1.14 to 5.83)).
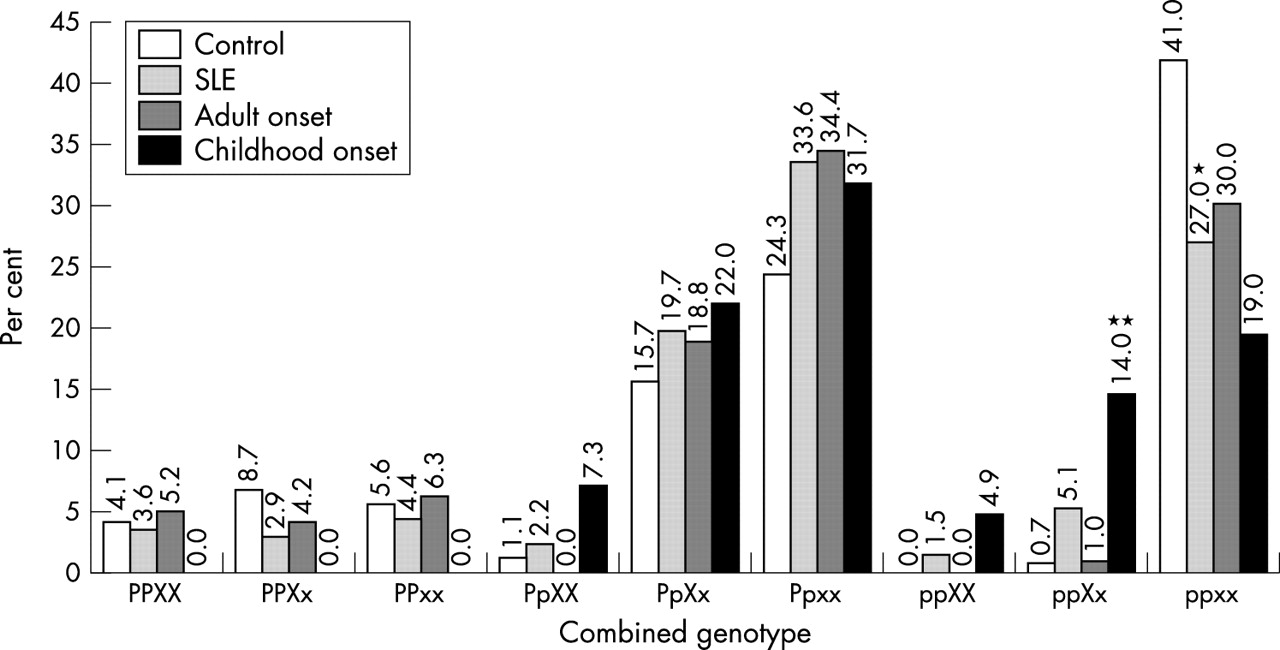
For the combination of the PvuII and XbaI polymorphisms, all combinations of genotype were observed in SLE patients, and the three major combined genotypes in the study groups were ppxx, Ppxx, and PpXx. SLE patients less often had the ppxx genotype than controls (pc = 0.032, OR = 0.52 (0.32 to 0.83); fig 1⇓). The frequency of the ppXx genotype was greater in the childhood onset SLE subgroup than in the control group or the adult onset subgroup (pc = 0.0009, OR = 22.80 (3.94 to 170.36) v controls; pc = 0.027, OR = 16.29 (1.83 to 371.63) v adult onset SLE; fig 1⇓). Moreover, the same tendency was detected in SLE patients with pre-menarche onset (pc = 0.0009, OR = 24.63 (3.96 to 193.51) v controls; pc = 0.018, OR = 9.54 (1.51 to 75.71) v SLE patients with post-menarche onset).

{kind=link}
Combined genotype of oestrogen receptor α polymorphism in controls and patients with systemic lupus erythematosus (SLE). For the combination of the PvuII and XbaI polymorphisms, all combinations of genotypes were observed in SLE patients and the three major combined genotypes: ppxx, Ppxx, and PpXx. SLE patients were less likely to have the ppxx genotype than controls (*pc = 0.032, OR = 0.52 (95% CI, 0.32 to 0.83)). The frequency of the ppXx genotype was significantly higher in the childhood onset SLE subgroup than in the control group or the adult onset subgroup (**pc = 0.0009, OR = 22.80 (3.94 to 170.36) v controls; pc = 0.027, OR = 16.29 (1.83 to 371.63) v adult onset SLE). CI, confidence interval; OR, odds ratio.
When clinical manifestations in SLE patients were analysed according to PvuII or XbaI polymorphisms, oral ulcer was associated with the pp genotype (pc = 0.015, OR = 2.88 (1.27 to 6.54)) and discoid rash was related to the xx genotype (pc = 0.032, OR = 0.34 (0.14 to 0.86)). Age at disease onset differed significantly in SLE patients according to the presence of PvuII or XbaI polymorphisms. SLE patients with the PP genotypes (mean (SEM), 38.1 (2.9) years old) were significantly older at disease onset than the other genotypes (p = 0.001, v 23.8 (2.0) years in the pp genotype, v 24.6 (1.5) in the Pp genotype; table 3⇓). The patients with the xx genotype had a later onset of SLE than those with the Xx genotype (p = 0.025; 28.1 (1.5) v 21.0 (1.6) years; table 3⇓). In the childhood onset SLE subgroup, patients with the pp genotype developed disease earlier than those with the Pp genotype (at 10.3 (0.9) v 12.4 (0.4) years, p = 0.046). However, in the adult onset SLE subgroup, the age at disease onset did not differ according to ORα RFLPs. The distributions of the other clinical and laboratory manifestations were not significantly skewed.
Association between the age at disease onset and ORα polymorphism in patients with systemic lupus erythematosus
To confirm the relation of ORα polymorphisms with disease onset in the SLE group, a logistic multivariate analysis was conducted (table 3⇑). The models for PvuII or XbaI polymorphisms included a continuous variable, age at disease onset, and some dichotomous variables such as oral ulcer, discoid rash, malar rash, photosensitivity, proteinuria, proliferative lupus nephritis, and anti-dsDNA. For the PvuII polymorphism, the variables of oral ulcer and age at disease onset interacted significantly (p = 0.047). A significant difference in the age at onset between the PP and pp genotypes was observed (adjusted OR = 1.10 (1.03 to 1.18)) under the condition of the absence of oral ulcer. When the adjusted OR for oral ulcer was calculated using first quartile, median, and third quartile age groups, there was no statistical significance. For the XbaI polymorphism, patients with the Xx genotype showed a younger onset than those with the xx genotype (adjusted OR = 0.95 (0.91 to 0.98)).
DISCUSSION
SLE is a multifactorial autoimmune disease, and genetic factors are thought to contribute to its pathogenesis. In human lupus studies, associations of SLE with some major histocompatibility class II alleles, complement deficiencies, and polymorphisms of Fcγ receptor genes, a complement related gene, and cytokine genes have been described. The biological actions of oestrogens are mediated through the oestrogen receptors, which function as a ligand inducible transcription factor and convey signals by binding as a complex of accessory proteins to specific DNA sequences in the promoters of oestrogen dependent genes. Thus oestrogen receptor polymorphism has been a target in the genetic study of diseases in which oestrogen may play a pathogenic role. However, although ORα polymorphism has been extensively investigated in many disorders, its association in SLE has not been fully examined. PvuII and XbaI RFLPs are representative among polymorphisms of the ORα gene and they have been reported to be associated with breast cancer, endometrial cancer, generalised osteoarthritis, bone mineral density, and lipid metabolism.10–,16
Previously, Liu et al reported the different distribution of ORα gene polymorphism in both male and female SLE patients, and showed a higher frequency of the PpXx genotype in male patients with lupus nephritis than in normal controls and female patients.17 In our study group, we examined ORα RFLPs in female patients to minimise the effect of the sex variable and did not observe a relation between renal disease and ORα polymorphism. The frequency of the ppxx genotype was lower in SLE patients than in controls, and ORα genotype distributions of adult onset SLE did not differ significantly from controls. Chang and his colleagues showed that ORβ microsatellite polymorphism was not associated with SLE.18 Whether oestrogenic effects are mediated through ORα or ORβ remains unclear, but sex hormones influence both humoral and cell mediated immune response in SLE patients. There was a recent report that ORα is predominantly responsible for mediating oestradiol induced haematopoietic and B cell changes in mice.20
In our study, we found that SLE patients with the Pp, pp, or Xx genotypes of ORα showed an earlier onset of disease and, in univariate analysis, childhood onset SLE patients were more likely to have ppXx genotypes than adult onset patients. Linear regression analysis confirmed that those with the pp or Xx genotype developed disease earlier than the others. However, in multivariate analysis, there were no significant associations between ORα RFLPs and the other clinical or laboratory manifestations.
Several studies have shown the effect of ORα polymorphism on the oestrogen action. Menarche occurs earlier in girls with the Xx, xx, Pp, and pp genotypes than in those with the ORα XX or PP genotypes.14 Without hormone replacement therapy, the lumbar spine bone mineral density decreases significantly less in postmenopausal Finnish women with the pp genotype than in those with the PP and Pp genotypes.15 In addition, there was a greater increase in bone mineral density after hormone replacement in Japanese women with the pp genotype than in those with the Pp or PP genotypes.12 Recently, it was observed that postmenopausal women with ORα IVS1-401 C/C—that is, the pp genotype—had greater increments in high density lipoprotein cholesterol after hormone replacement.16 Considering that the oestradiol level in prepubertal girls is lower than in women, and there was a skewed distribution of the pp and Xx genotypes in these studies, it may be speculated that the pp and Xx genotypes in our patients are oestrogen sensitive.
Some polymorphisms observed in SLE were previously reported to be related to disease onset. Reveille et al showed that early onset SLE patients (⩽20 years old) have a high frequency of HLA-DRw8,21 and Manger et al reported that SLE patients with Fcγ IIA-R/R131 and IIA/IIIA-R/R131, F/F158 polymorphisms have a younger onset of disease.22 However, the number of early onset SLE subjects was very small (18 patients in the former study), or not mentioned. Our study included more childhood onset SLE patients than the previous studies, and an association between ORα polymorphism and disease onset was confirmed by both univariate and multivariate analyses. These results suggest that the ORα gene may be a susceptibility locus for childhood onset SLE in Korea.
The mechanism whereby the PvuII or XbaI polymorphisms in intron 1 of the ORα gene affect SLE remains unclear. Polymorphisms in the ORα gene are likely to affect the expression or activity of the receptor. The restriction sites are near the transactivating factor 1 domain of the ORα gene, which is an important portion for promoting transcription from oestrogen responsive promoters, and there is some evidence that protein expression or function can be influenced by polymorphisms in the first intron.23–,25 Another explanation is that these polymorphisms can be in linkage disequilibrium with those of other genes.
Our study had some limitations. The number of childhood onset SLE patients was not large and some manifestations were different between the childhood onset and adult onset subgroups. Sample size is a common obstacle to polymorphism studies of a disease with low incidence. Although SLE is predominantly found in young women of reproductive age, 8–15% of patients were diagnosed in children younger than 16 years.26 The overall incidence of SLE is between 2.0 and 7.6 per 100 000 per year, and that of childhood onset SLE, 0.36 to 0.6 per 100 000 per year.27 However, the true prevalence of childhood onset SLE among SLE patients is unknown. The persuasive reason is that there is so far no strict or adopted definition of childhood onset SLE. The most used cut off ages are 1426 or 16 years at onset of disease.28 In our study, childhood onset SLE was defined as SLE beginning before the age of 16 years. With concerns about the different manifestations in the two subgroups, childhood onset SLE appears to have more frequent renal involvement, fever, and lymphadenopathy, and more severe organ involvement than adult onset disease.28,29 However, it is unknown whether this difference reflects age related factors, the disease itself, genetic factors, environmental factors, or a combination of these.30 We therefore tried to minimise the sampling bias by using multivariate analyses, and the results of linear regression analysis were similar to those of univariate analysis.
Conclusions
ORα polymorphism was found to be associated with age at disease onset in Korean SLE patients, and its relation may indirectly support the concept that oestrogen affects the pathogenesis of SLE. To establish the relation between ORα polymorphisms and SLE firmly, further large scale studies of patients, including those with childhood onset SLE, are required in other populations.
Acknowledgments
We acknowledge the excellent technical assistance of Ji Hee Kim MSc. This work was supported partially by Annual Research Grants 2002 from Gyeongsang National University Hospital, Korea.