Article Text

Abstract
Treatable causes of parkinsonian syndromes are rare; Whipple’s disease is one of them. A patient is described who presented with a parkinsonian syndrome and abnormal vertical gaze. Measurement of eye movements showed marked slowing of upward saccades, moderate slowing of downward saccades, a full range of voluntary vertical eye movements, curved trajectories of oblique saccades, and absence of square wave jerks. These features, atypical of progressive supranuclear palsy, suggested the diagnosis of Whipple’s disease, which was subsequently confirmed by polymerase chain reaction analysis of intestinal biopsy material. Precise measurement of the dynamic properties of saccadic eye movements in parkinsonian patients may provide a means of identifying treatable disorders.
- vertical saccades
- parkinsonian syndrome
Statistics from Altmetric.com
Examination of the range of eye movements has proved useful in diagnosing parkinsonian syndromes. Limitation of voluntary vertical gaze is characteristic of progressive supranuclear palsy (PSP)1; it has also been reported in diffuse Lewy body disease.2However, the diagnostic value of restricted vertical gaze is partly confounded by the common finding of limited upgaze in healthy elderly subjects.3 Restricted downgaze may be more relevant, but has not received systematic study. Recent evidence indicates that quantification of vertical saccades—their accuracy, speed, and trajectory—may be more sensitive and reliable for diagnosis than simply observing the range of voluntary vertical gaze.4 Further, slowing of vertical saccades will result in curving of the trajectory of diagonal saccades, due to faster completion of the horizontal component than its vertical counterpart.5
Recently, we encountered a woman with a parkinsonian syndrome and impaired vertical gaze, diagnosed as PSP. Quantitative measurements of her eye movements disclosed findings atypical for PSP, and prompted testing for Whipple’s disease.
Case report
A previously healthy 54 year old woman developed blurred vision and difficulty focusing on objects over a period of 6 months. She became aware of some clumsiness and a sense of imbalance. An episodic pulsating sensation in the left temple was interpreted as paroxysmal hemicrania. There was no history of gastrointestinal complaints, arthralgia, or weight loss. On examination, she was cognitively intact. Blinking was frequent, without overt blepharospasm. Vertical saccades were initiated with difficulty and appeared slow. However, her range of voluntary eye movements was full in all directions. Convergence was poor. Fixation, smooth pursuit, and vestibulo-ocular reflexes seemed normal but were difficult to evaluate clinically because of the frequent blinking and fatiguability of the patient. She had brisk deep tendon reflexes but the plantar responses were flexor. Her speech was hypophonic. Her gait was slightly broad based, with difficulty on turns, impaired tandem, and retropulsion. She showed no tremor, axial rigidity, or postural hypotension. A trial of Sinemet 25/100 twice a day was unsuccessful. A diagnosis of PSP was made by two neurologists.
LABORATORY TESTS
Laboratory tests that included complete blood count, sedimentation rate and blood chemistry were within normal limits. Vitamin E concentration was 5.3 mg/l (normal 5.5–17.0 mg/l).
Brain MRI with gadolinium showed a venous angioma in the left cerebellar hemisphere but was otherwise unremarkable. The patient declined a lumbar puncture.
EYE AND HEAD MOVEMENTS
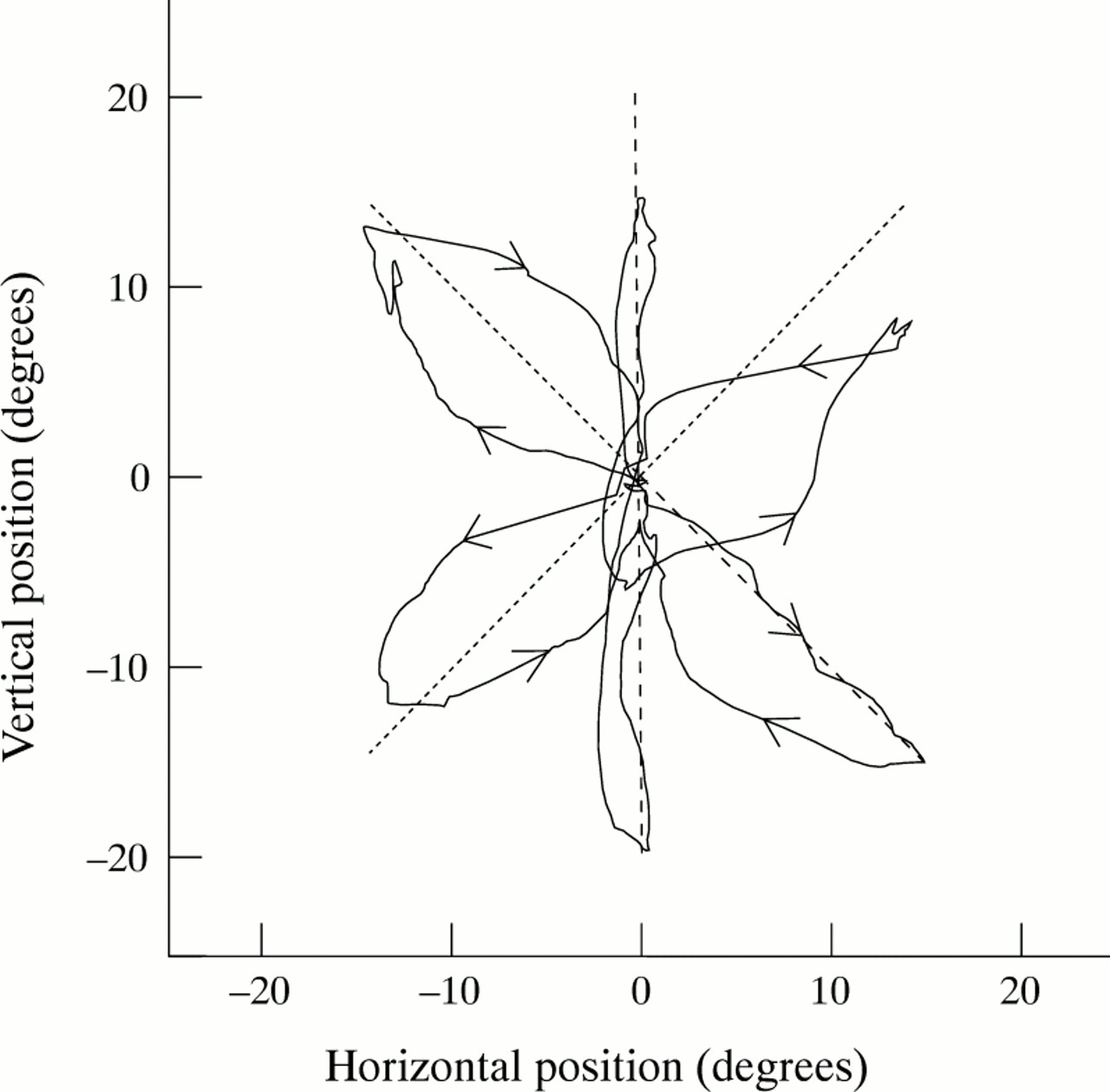
Eye and head movements in the horizontal and vertical plane were measured using the magnetic search coil technique, as previously described.4 Informed consent was obtained from the patient before the recording session. The recording documented that vertical saccades were slow and hypometric, more so in the upward direction (fig1 A and B). For example, velocities of 20–30 degree vertical saccades, made back and forth across the straight ahead position, averaged 60 degrees/s for upward, and 130 degrees/s for downward saccades (95% confidence interval (95% CI) for age >275 degrees/s).4Horizontal saccades of comparable amplitudes (fig 1 C and D) were hypometric but of normal velocity; the velocity of such saccades (as shown in fig 1) exceeded 300 degrees/s (95%CI >285 degrees/s). Trajectories of the oblique saccades were curved (fig 2), indicating desynchronisation of the horizontal and vertical saccadic components; the horizontal component occurred more rapidly and was completed before the vertical. Smooth pursuit and vestibulo-ocular movements (elicited by active quasisinusoidal head rotations) were preserved both horizontally and vertically (gain near unity).4 Fixation was steady and square wave jerks were not seen.
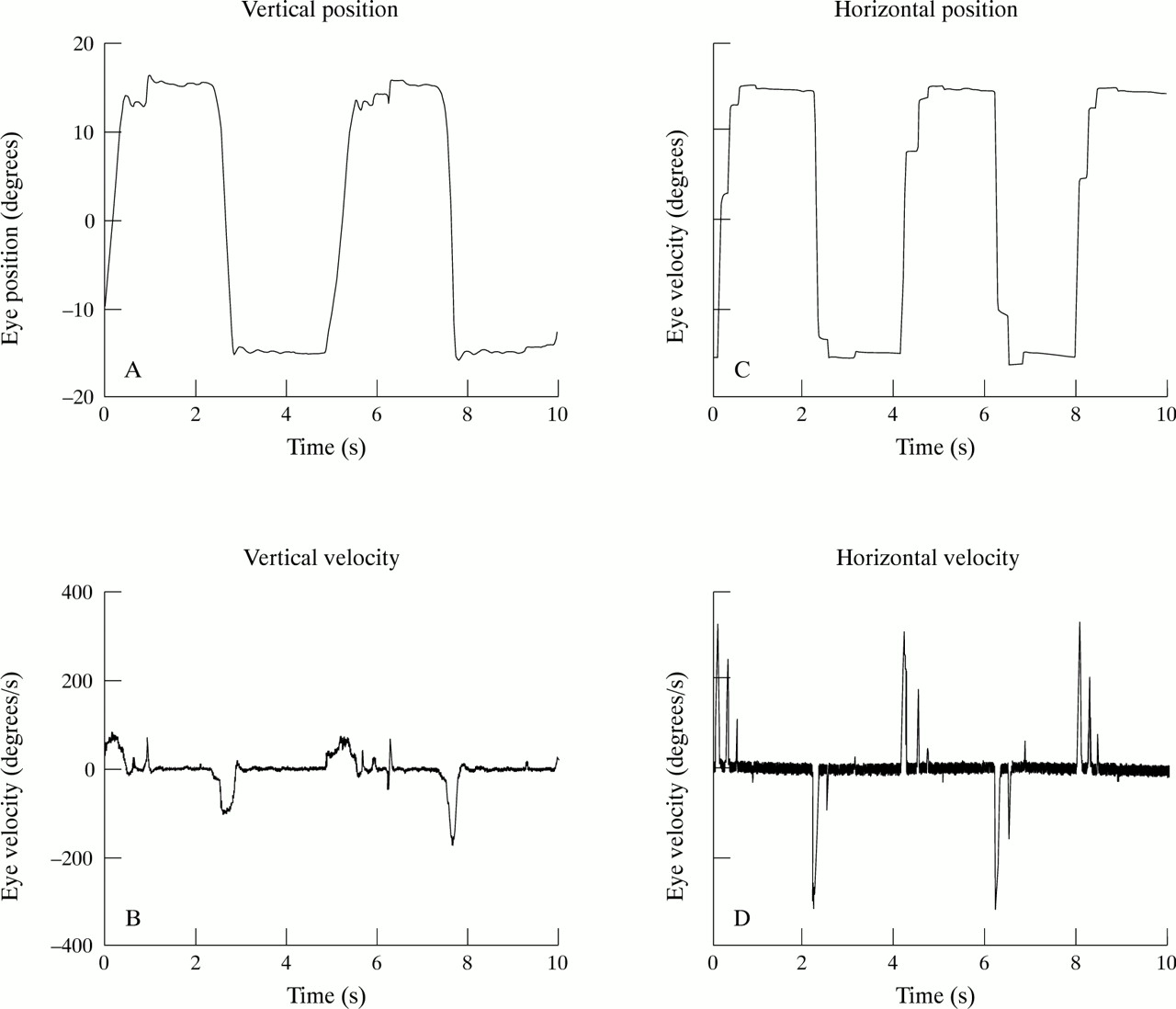
Example of slow vertical saccades. Scleral magnetic search coil recording. Two 10 second segments of right eye recording during vertical saccades (A,B) and horizontal saccades (C,D). Upper panel represents eye position (degrees), lower - eye velocity (degrees/s). Note slow, but not limited, vertical saccades, particularly upward. Both range and velocity profiles of horizontal saccades are within normal limits. Upward deflections correspond to upward or rightward eye rotations.
{kind=link}
{kind=link}
Example of trajectories of diagonal saccades. Two dimensional plot of right eye recording during attempted 20 degree diagonal saccades. Dotted lines represent target jumps. Arrows indicate direction of eye displacement. Note that during diagonal saccades, the horizontal component displacement leads the vertical, producing a curved trajectory. The eye does not always reach the new target position (indicated by outmost ends of the dotted lines) because some saccades are hypometric. Upward deflections correspond to upward eye rotations, rightward deflections to rightward eye rotations.
SMALL BOWEL BIOPSY
A small bowel biopsy specimen was unremarkable on light microscopy (PAS negative; electron microscopy not done). Polymerase chain reaction (PCR) analysis performed on the biopsy material was positive for the Whipple associated bacillus, Tropheryma whippelii.
After the diagnosis, the patient was treated with co-trimoxazole. While taking the medication, she developed bruxism and myorhythmia involving her left shoulder and hand that was synchronous with the pulsating sensation in her left temple. Carbamazepine and valproate were ineffective in controlling the myorhythmia. The treatment was changed to intravenous ceftriaxone, with gradual stabilisation and subsequent improvement in the myorhythmia and in vertical eye movements over a few months. After 2 years of follow up, the patient remains asymptomatic.
Discussion
We present the first reliable records of abnormal vertical and diagonal saccades in Whipple’s disease. The findings consisted of a selective slowing of vertical, particularly upward, saccades that resulted in a curved trajectory of diagonal saccades. We suggest this to be an early and sensitive sign that can be found before the saccadic slowing becomes clinically apparent, in any condition that differentially affects horizontal and vertical gaze. Smooth pursuit and vestibular movements were preserved, and fixation was not disrupted by square wave jerks. These features differed from the usual ocular motor findings in PSP, in which the range of voluntary vertical movements is characteristically limited, horizontal smooth pursuit is commonly impaired, and fixation is disrupted by square wave jerks (small saccadic intrusions).6 These differences may reflect more extensive involvement of brainstem and cerebellar pathways controlling gaze in PSP compared with Whipple’s disease.7 Moreover, in PSP downward eye movements may be more severely affected,4 8-11 unlike the findings in our patient. It was these features, atypical of PSP, that prompted consideration of other disorders, including Whipple’s disease.
Involvement of the CNS occurs only rarely (5%) as the first manifestation of Whipple’s disease,12 and so this disorder often is not considered in the differential diagnosis if patients lack gastrointestinal symptoms. A careful neuro-ophthalmological examination may be useful in suggesting a diagnosis. However, important dynamic properties of eye movements such as greater slowing of upward rather than downward saccades, normal smooth pursuit and the vestibuloocular responses, and the stability of gaze during attempted fixation can be demonstrated with more certainty by measuring the eye movements.
The predilection of Tropheryma whippelii for specific areas of the grey matter accounts for its distinctive neurological manifestations.12 13 In particular, basal ganglia involvement can result in movement disorders, and parkinsonism may be a prominent feature, with the clinical picture resembling PSP because of the common association with vertical ophthalmoplegia.12 14-16 Involvement of the rostral mesencephalon, with abnormal vertical gaze, is found in more than 50% of patients with Whipple’s disease of the CNS, and may be accompanied by oculomasticatory or oculofacioskeletal myorhythmia.17The myorhythmia is virtually pathognomonic for Whipple’s disease; it consists of rhythmic movements of masticatory and occasionally other skeletal muscles synchronised with “pendular vergence oscillations” of the eyes—horizontal, convergent-divergent pendular nystagmus at about 1 Hz.17 However, most patients with Whipple’s disease, such as ours, have no ocular oscillations,12 and in them study of the dynamic properties of eye movements, including vertical saccades, may provide crucial diagnostic information.
The selective deficit of vertical saccades in our patient may be attributed to the involvement of the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF), which is an anatomical substrate for generation of vertical saccades.18 This nucleus, lying at the mesodiencephalic junction, contains neurons that fire for both upward and downward saccades, and for ipsiversive torsional saccades. The isolated finding of slow vertical saccades suggests selective vulnerability of the riMLF compared with the pontine paramedian reticular formation (PPRF), which is important for generation of horizontal saccades. Why the riMLF should be preferentially affected is not clear; one factor may be its proximity to the ventricle making it more susceptible to infection by the bacillus.
The ability to diagnose Whipple’s disease has been enhanced by the recent introduction of a PCR based approach, which is highly sensitive and specific.19 20 Analysis of small bowel biopsy material by PCR can be positive in the absence of clinical signs of gastrointestinal involvement, and even when the intestinal tissue is microscopically negative,21 as in our patient. Moreover, although positive PCR confirms the diagnosis, negative PCR does not exclude it16; therefore, repeat biopsies from multiple sites are indicated. The usefulness of PCR analysis in CSF is not clear16; it may be of value in the presence of pleocytosis.22
In conclusion, we propose that patients presenting with clinical findings suggestive of PSP should be evaluated with measurement of vertical and horizontal eye movements and, if findings are atypical for this condition, that further investigation be instituted, including consideration of PCR testing for Whipple’s disease, even in the absence of overt gastrointestinal involvement.
Acknowledgments
The work was supported by NIH grants EY11714 (to LAH) and EY06717 (to RJL), and the Department of Veterans Affairs and the Evenor Armington Fund (to RJL). We are grateful to Dr David H Persing for providing the PCR analysis of the patient’s biopsy.