Article Text

Abstract
BACKGROUND K-rasmutation is one of the first genetic alterations in classical colorectal carcinogenesis.
AIMS To investigate the role of K-ras mutations in carcinogenesis, in long standing ulcerative colitis.
METHODS A total of 161 microdissected and 100 DNA samples from 13 patients were analysed for K-ras codons 12 and 13 mutations by means of a combination of enriched polymerase chain reaction amplification and temporal temperature gradient electrophoresis.
RESULTS K-rasmutations were found in 21/161 (13%) microdissected samples in 7/13 large bowels (16 and five in codons 12 and 13, respectively), and in 10/100 (10%) mucosal DNA samples (six and four, respectively). One of four patients with six adenocarcinomas had a K-ras mutation in a carcinoma, as well as one of two patients with large dysplasia associated lesion or mass (DALM). Eight of 13 (61%) areas with villous architecture and large, distended goblet cells, had a K-rasmutation, which was significantly more frequent than in low grade dysplasia (one of 23, 4%) but did not reach significance versus high grade dysplasia (four of 14, 28.5%). K-rasmutations were found in one of 20 (5%) flat lesions indefinite for dysplasia, two of 14 (14%) in non-villous, hypermucinous mucosa, and in one of 57 flat areas negative for dysplasia.
CONCLUSION The highest K-ras mutation frequency was found in villous, hypermucinous mucosa. We suggest that this entity should be investigated further as a potential risk lesion for cancer development. It may represent a pathway directly from non-classical dysplasia to cancer, not previously described.
- K-ras mutations
- ulcerative colitis
- dysplasia
- dysplasia associated lesion or mass
Abbreviations used in this paper
- DALM
- dysplasia associated lesion or mass
- PCR
- polymerase chain reaction
- TTGE
- temporal temperature gradient electrophoresis
Statistics from Altmetric.com
According to the multistep route of genetic alterations in the colorectal adenoma-carcinoma sequence, K-rasmutation is one of the first alterations to occur.1 The frequency of K-ras mutation in adenomas increases with size, adenoma type, and grade of dysplasia, and different authors report mutations in 40–70% of adenomas larger than 2 cm, and in 39–58% of adenomas with high grade dysplasia.2-4 In colorectal adenocarcinomas several groups have found the frequency of K-rasmutation to be about 40%.5-8
There is no unanimous agreement concerning the succession of genetic alterations developing in ulcerative colitis—that is, whether the mutations accumulate gradually in parallel to the grade of dysplasia. Carcinomas in ulcerative colitis have many of the same mutations as sporadic colorectal adenocarcinomas, but they have been found in various frequencies in different investigations. Concerning K-ras mutations, some groups have found mutations in carcinomas and dysplasia in ulcerative colitis to be lower than in sporadic adenocarcinoma and adenomas,9-13 while others showed K-ras mutation frequency in carcinoma in ulcerative colitis to be about the same as in sporadic adenocarcinoma.8 ,14-16
The aim of this study was to relate classical histopathological methods for the grading of dysplasia in ulcerative colitis to a genetic marker of known distribution in other precancerous lesions, for instance, in large bowel adenomas.
Materials and methods
PATIENTS
Thirteen patients who underwent coloproctectomy consecutively in the period from June 1992 to September 1994 were chosen for these investigations. Ten patients were men and three were women, median age 41 years (29–75 years). They suffered from long standing ulcerative colitis (10–30 years) and were followed up with regular biopsies for evaluation of dysplasia. Nine of the patients were resected because of persisting dysplastic changes, whereas four had developed carcinoma. Three of them had been followed up in other hospitals, dropped out of the surveillance programme for a period of two to three years, and then returned with carcinoma. The fourth patient developed a Dukes’s stage A carcinoma between two control visits 12 months apart. Two patients with a dysplasia associated lesion or mass (DALM)17 had been followed up in other cities until the lesions were detected.
COLECTOMY SPECIMENS
The proctocolectomy specimens showed different types of epithelial changes, including dysplasia and cancer. All specimens displayed more or less inactive colitis with little active inflammation. Four patients had adenocarcinomas: one had a Dukes’s A carcinoma in the caecum, another a Dukes’s C in the sigmoid, a third patient presented a multifocal and mucinous Dukes’s C carcinoma with three tumours in the transverse and descending colon, and the fourth had a Dukes’s D adenocarcinoma with primary tumour in the transverse colon. One patient had a large DALM (diameter 8 cm) with intramucosal carcinoma in the transverse colon, and one patient showed a DALM (4 cm) with high grade dysplasia in the rectum (table 1).
Clinical and pathological data of patients with ulcerative colitis
All colectomy specimens were opened longitudinally and rinsed in ice cold phosphate buffered saline (PBS), pH 7.6, immediately after removal, and thereafter placed in a bucket of PBS which was immersed in ice. Within eight hours tissues from eight or nine segments were removed; neighbouring tissue blocks were either fixed in 96% ethanol at 4°C18 or formalin, embedded in paraffin wax or OCT preservative (Miles Inc., Elkhart, Indiana, USA) for freezing. Finally, mucosa samples in close proximity to the tissue blocks were scraped off and prepared as single cell suspensions for subsequent DNA extraction.
HISTOPATHOLOGICAL LESIONS
For each colectomy sample, the histopathological lesions of interest were first identified on routinely stained slides and classified according to Riddell et al.19 In addition, two variants with hypermucinous epithelium were defined, one of them described by Morsonet al: villous surface with high number of goblet cells, but without nuclear atypia.20 The other variant had abundant goblet cells, no nuclear atypia, but a flat surface. Altogether, 161 mucosal lesions were selected (table2).
Distribution of K-ras mutations according to histological evaluation and grade of dysplasia in microdissected areas
MICRODISSECTION
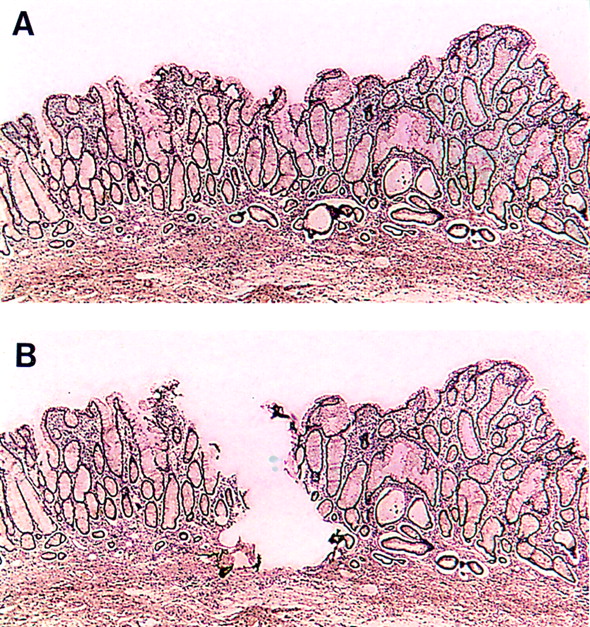
Parallel sections were cut with the microtome set at 6 μm, and the slides dried overnight at 37°C. Corresponding areas of interest were delineated and microdissected under a Leica dissection stereomicroscope after rapid staining with haematoxylin and eosin. Thereafter the tissue was scraped off the slide (the sections were covered by 25 μl Tris buffer, 0.05 mol), with the tip of a sealed glass pipette and then sucked into a microcapillary. Figures 1A and B show the same slide before and after microdissection. Tissue samples were then put into Eppendorf tubes and incubated with proteinase K at 37°C overnight. Proteinase K activity was inactivated by heating to 95°C for 10 minutes, and the resulting solutions were used directly as templates for K-rasanalyses.

Section from large bowel mucosa of patient 2, rich in goblet cells, but without dysplasia, (A) before and (B) after microdissection.
DNA EXTRACTION
For DNA extraction from fresh mucosa in close vicinity to the tissue blocks, standard methods were used: after incubation with proteinase K at 37°C overnight the mucosa was extracted twice in phenol and twice in chloroform, followed by ethanol precipitation.
K-ras MUTATION ANALYSIS
K-ras mutations in codons 12 and 13 were identified in DNA from each of the microdissected areas, as well as in mucosa extracted from neighbouring areas, by means of a modification of the “enriched PCR method”7 combined with temporal temperature gradient electrophoresis (TTGE).21
Briefly, the initial PCR reaction (A) was performed in 25 μl of PCR amplification buffer (50 mmol/l potassium chloride, 10 mmol/l Tris HCl, 1.5 mmol/l magnesium chloride), with either 1 μl of template from microdissection or 50 ng of extracted DNA, 25 μmol of each deoxynucleoside triphosphate, 0.28 μgTaqStart Antibody (Clontec, Palo Alto, California, USA), 1.25 U of Taq DNA polymerase (Promega, Madison, Wisconsin, USA), and 0.04 μmol and 0.2 μmol of the oligonucleotide primers (Genosys Biotechnology, Houston, Texas, USA) 5K1 and 3K1 respectively: 5′-ACTGAATATAAACTTGTGGTCCATG GAGCT-3′ and 5′-TTATCTGTATCAAAGAA TGGTCCTGCACCA-3′. These primers give a PCR product of 170 bp. The 5K1 primer was designed (modified, mismatching bases are underlined) to induce two restriction sites in the wild type (WT) amplification product (N = any base): 5′-CCANNNNNNTGG-3′ which is recognised by endonucleaseBstXI, and involves WT codon 12. 5′-CCANNNNNNNNNTGG -3′ is recognised by endonucleaseXcmI, and involves WT codon 13.
The amplification was performed in a GeneAmp PCR System 9600 (Perkin-Elmer, Foster City, California, USA). The reaction was run for 20 cycles consisting of 30 seconds denaturation at 94°C, one minute annealing at 50°C, and two minutes elongation at 72°C. After the last cycle the tubes were kept at the elongation temperature for 10 minutes. A 5 μl aliquot of the amplification product was incubated with either 10 U of BstXI or 2 U ofXcmI. Digestion was performed as recommended by the supplier of both the endonucleases (New England Biolabs, Beverly, Massachusetts, USA), in a volume of 20 μl. A 5 μl aliquot of the digested amplification product was used directly as a template in an amplification reaction (PCR B) of 25 μl. This time the following primers were used: 5′-ATGACTGAATATAAACTTGTG and 5′-GCCCCGCGCCCGTCCCGCCGCCCCC GCCCG CTC TAT TGT TGG ATC ATA in final concentrations of 0.32 and 0.16 μmol each, together with PCR amplification buffer, 100 μmol of each deoxynucleoside triphosphate, and 1 U of Taqpolymerase.
The reverse GC clamped primer is nested to 3′K1, and these two primers give a PCR product of 111 bp.
After the first annealing step of two minutes at 95°C, the reaction was run for 35 cycles consisting of 30 seconds denaturation at 95°C, 30 seconds annealing at 58°C, and 30 seconds elongation at 72°C. After the last cycle the tubes were kept at the elongation temperature for five minutes. The PCR amplification products were verified on 2% agarose gel containing ethidium bromide, and analysed in ultraviolet light, prior to being subjected to temporal temperature gradient electrophoresis (TTGE).21
TTGE ANALYSIS
The TTGE analyses were performed with the DCode system (Bio-Rad, Hercules, California, USA), using 16 × 16 cm glass plates, with gel containing 10% acrylamide/bis with 6 mol/l urea in 1.25 × TAE buffer (50 mmol/l Tris, 25 mmol/l acetic acid, 1.25 mmol/l EDTA), according to the manufacturer’s recommendations. The PCR B products were electrophoresed at 130 V for five hours with a temperature range of 52–62°C. The gel was then stained in SYBR Green I (Molecular Probes Inc., Eugene, Oregon, USA) and photographed using an ultraviolet transilluminator at 300 nm.
DNA SEQUENCING
All mutation positive samples from the TTGE analysis were sequenced in order to identify the exact base substitution. PCR products were purified using the Qiaquick PCR purification kit (Qiagen, Hilden, Germany) and sequenced using dye primer cycle sequencing and AmpliTaq polymerase FS on an Applied Biosystems 377 DNA sequencer.
CONTROLS
DNA from colon carcinoma cell lines SW480 (Clontech, Palo Alto, California, USA) and HCT116 (American Type Culture Collection, ATCC, Rockville, Maryland, USA) with known K-rasmutations at codon 12 (GTT) and codon 13 (GAC) respectively, were used as positive controls in each of the parallel procedures. Negative controls, without DNA, were run as controls for contamination.
STATISTICAL ANALYSIS
Associations between different variables were examined using the χ2 method with Yates’s correction; p values less than 0.05 were considered statistically significant.
Results
HISTOPATHOLOGY
Each of the 161 microdissected areas was diagnosed by one experienced pathologist (SNA). To check for interobserver reproducibility, 59 adjacent sections were blindly and independently evaluated for different grades of dysplasia according to standard criteria for comparison,19 by two histopathologists (SNA and OPFC) with a κ value of 0.64, which means substantial agreement.22 The remainder of the slides were afterwards agreed on by OPFC. Intraobserver agreement (SNA) after three months was “almost perfect” (κ=0.82).
One third of the microdissected areas (n=57) consisted of carcinoma or high or low grade dysplasia, while 20 showed flat mucosa, indefinite for dysplasia. Thirteen areas from six large bowels contained a villous growth pattern with hypermucinous, distended goblet cells (fig 2), and 14 were non-villous, hypermucinous, and without dysplasia. Table 2shows the different types of lesions.

Mucosal specimen from patient 11, with villous growth pattern and elongated, distended goblet cells without cytological atypia. This area was K-ras mutation positive.
K-ras MUTATIONS
Altogether 261 K-ras analyses were performed on tissue from 13 colectomy specimens: 161 from microdissected tissue and 100 from DNA extracted from nearby mucosa. K-ras mutations were found in 21 (13%) and 10 (10%) of these, respectively. Table 3 shows a survey of microdissected lesions and mucosa specimens in each of the patients, and the number of K-ras mutation positive lesions. Six of the 13 large bowels did not show any K-ras mutation by analysis of microdissected lesions, while DNA from mucosa specimens was K-ras mutation negative in five bowels.
Survey of K-ras mutation positive lesions in each of the 13 patients
Twenty one of the 161 microdissected areas (13%) were K-ras mutation positive, 16 in codon 12 and five in codon 13. Only one of the four patients (25%) with a total of six carcinomas had a tumour containing a K-ras mutation. Four of the 20 carcinoma specimens analysed were from this tumour, taken at different levels of infiltration (table 4), and showing identical mutation. Four of 14 (28.5%) high grade lesions were K-rasmutation positive, while only one of 23 (4%) low grade lesions and one of 20 (5%) lesions indefinite for dysplasia in flat mucosa were positive (table 2).
Distribution and type of 21 K-ras mutations in DNA from microdissected areas
Eight of 13 K-ras mutation positive lesions (61%) were found in mucosa with villous growth pattern with “hypermucinous” epithelium, very rich in large, distended goblet cells, having nuclei without definite cytological atypia. These had previously been defined as “indefinite for dysplasia”, as delineated by Morson et al.20The frequency of K-ras mutations in this entity was significantly higher than in low grade dysplasia (p<0.001, table 2), but did not reach significance versus high grade dysplasia. The mutation frequency in villous, hypermucinous mucosa was also significantly higher than compared with flat mucosa, indefinite for dysplasia (one of 20, p=0.002) and areas negative for dysplasia, with regenerating or atrophic mucosa (one of 57, p=0.001). Two of 14 (14%) flat, hypermucinous lesions without dysplasia were K-ras mutation positive (p=0.03). Figure 2shows one of the K-ras positive lesions in patient 11.
Table 4 shows the distribution and type of K-ras mutations in DNA from microdissected areas. Among the eight villous, hypermucinous lesions, four were from patient 11 and showed an identical mutation (12 AGT—serine), despite considerable distance (several cm) between each of them. The last four were from three different patients, two from patient 9 (with the same 12 AGT mutation), and the two last (patients 10 and 3) showing an aspartate mutation in codons 12 (GAT) and 13 (GAC), respectively.
Among the two patients with DALM, one was K-ras mutation negative (patient 5), and the other K-ras positive (patient 6), shown both in DNA from microdissection and mucosal “slicing”. Figure 3illustrates gels with mutated bands from K-ras investigations, while fig 4 shows DNA sequence analysis of wild type (A) and mutated (B) K-ras.

TTGE gel showing migration patterns of K-ras exon 1 fragments. All lanes show different migration patterns at the upper bands (heteroduplex bands), indicating different K-ras mutations. The lower band is the homoduplex band. Lanes 1–5 show codon 12 mutations: (1) GTT (valine); (2) TGT (cysteine); (3) GAT (aspartate); (4) GCT (alanine); and (5) AGT (serine). Lane 6 shows a codon 13 GAC mutation (aspartate).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Automated sequence analysis of K-ras, showing wild type sequence GGT in codon 12. This is an inverse analysis, and should be read from right to left. (B). K-ras mutation in the second base in codon 12, giving the sequence GAT (aspartate) instead of GGT (glycine).
Discussion
The most intriguing result of this investigation was the high proportion of mucosal lesions with villous, hypermucinous appearance, without cytological dysplasia, which were K-ras mutation positive. As carcinomas may develop in ulcerative colitis without concomitant signs of classical dysplasia (Fenoglio-Preiser, personal communication), this new entity should be studied further with regard to association with malignant development. The percentages of K-rasmutation positive carcinomas, and high and low grade lesions were lower than in corresponding lesions related to sporadic colorectal carcinogenesis, and were in agreement with previous findings.9-13 ,15
At least five groups have investigated K-ras mutations in normal and regenerating mucosa and in mucosa indefinite for dysplasia (table5).9 ,10 ,12 ,14 ,16 Only two of them found K-ras mutations in “normal” mucosa and in lesions indefinite for dysplasia, including so called “villous regeneration” and “serrated lesions”.12 ,16 These had no resemblance to hyperplastic polyps. We were particularly interested in the villous lesions with large, distended goblet cells, without cytological atypia, which we have seen in some patients with long standing ulcerative colitis. These lesions were characterised as a separate entity. As the clinical significance with respect to malignant potential of this growth pattern has not yet been determined, Morsonet al recommend that this entity should be categorised as “indefinite for dysplasia”.20 Riddellet al did not include such lesions in their classical paper about criteria for the classification of dysplasia in inflammatory bowel disease.19
Frequency of K-ras mutations in different lesions in long standing ulcerative colitis (UC)
In 1987 Lee described villous regeneration in three patients among 92 cases of ulcerative colitis.23 In these cases the finger like formations were covered by cuboidal or columnar epithelium with variable degree of maturation towards the lumen, and with enlarged, vesicular nuclei with striking nucleoli. Mucin was absent, although a variable number of goblet cells were present. None of our patients showed this type of mucosa. However, four of our patients (patients 3, 9, 10, and 11) showed variable degrees of villous regeneration, often with large, distended goblet cells (fig 2).
In a recent study only 11 of 278 samples (4%) from seven ulcerative colitis colectomy specimens showed K-rasmutations, among them two of five carcinomas.24 The percentages both in dysplastic and non-dysplastic lesions were about 3%, but the authors have not described the types of non-dysplastic lesions.
Both Chaubert et al 12 and Redston et al 16 found K-ras mutations in epithelium indefinite for dysplasia or showing regenerative changes. Among lesions indefinite for dysplasia were some borderline lesions of uncertain clinical significance, such as hypermucinous epithelium, serrated epithelium, and epithelium with incomplete maturation. In our study we examined 14 flat lesions with hypermucinous epithelium, and found K-ras mutations in two (14%), in patients 2 and 11 (table 4). These were situated several cm apart from the other mutated areas in these patients. None of the former authors’ lesions were identical to what we call “villous, hypermucinous lesion with distended goblet cells”. Two of our patients (table 4; patients 11 and 9) had two and four areas, respectively, with the same GGT to AGT K-ras mutation, coding for serine, whereas the two last lesions in one patient each had different mutations.
It has been suggested that carcinomas in ulcerative colitis might follow an alternative genetic pathway for tumour progression, as relatively few dysplasias and carcinomas contain K-ras mutations.10-13Benhattar and Saraga25 have compiled the results of five reports,10-12 ,14 ,15 and conclude that K-ras mutation plays an important role in ulcerative colitis associated carcinomas, although the prevalence is slightly lower than in sporadic carcinoma (30% versus 40%). Interestingly, a high frequency of K-rasmutation is found in aberrant crypt foci (ACF), a lesion claimed to be a precursor of both hyperplastic polyps and adenomas.26The same authors claim that K-ras mutations are frequent also in hyperplastic polyps, a type of lesion said to have low malignant potential.27 However, we could not find K-ras mutations in any of the 15 hyperplastic polyps which we have examined previously, despite using a more sensitive “enriched PCR method” detecting one mutated K-ras codon 12 or 13 allele in the presence of 104–105 copies of the wild type allele.4 The discrepancy may be due to the possibility that only a small fraction of hyperplastic lesions are really neoplastic, and serve as precursor of a subset of colorectal cancers.28 One possible explanation could be thatras mutations may have little neoplastic potential in the absence of other mutations, such asAPC and p53.29 None of the hypermucinous lesions in the present paper did resemble hyperplastic polyps, but this theory may concern them as well. Therefore,APC and p53 mutations will soon be investigated.
The materials and methods chosen are important. In our study of microdissected lesions, the tissue used was fixed in ethanol which is a good preservative of nucleic acids.30 Our analysis is based on an “enriched PCR method”, combined with TTGE and automated sequencing, and the sensitivity of the TTGE method has been estimated to detect a mutation down to about 1% of the cells.21
The frequency of K-ras mutations in DNA extracted from “sliced” mucosa close to the tissue blocks was about the same as by microdissection (10% versus 13%), but did not always show the same result. This might be explained by the fact that although neighbouring tissue was used, often less than 4 mm apart, the K-ras mutation positive clones may be of even smaller size.
Villous, hypermucinous lesions, previously included among mucosal lesions indefinite for dysplasia, had twice the K-ras mutation frequency compared with high grade dysplasia. We suggest that this new entity should be investigated further as a potential risk lesion for cancer development. Mucinous carcinomas are relatively frequent in patients with ulcerative colitis.31 Perhaps villous, hypermucinous lesions may represent a pathway directly from non-classical dysplasia to cancer, not previously described.
Acknowledgments
The authors are grateful to The Norwegian Cancer Society for financial support. They also wish to thank the staff at the Surgical Department B, the National Hospital, who provided the colectomy specimens, and Iris Arnesen and Ann Kristin Stave for technical help.
Abbreviations used in this paper
- DALM
- dysplasia associated lesion or mass
- PCR
- polymerase chain reaction
- TTGE
- temporal temperature gradient electrophoresis