Article Text

Abstract
Background—Serrated adenoma is a new morphological subtype of colorectal adenoma. The lesion provides a distinct morphological route to carcinoma, but the underlying genetic changes have not yet been investigated.
Aims—To determine the frequency of K-ras mutation in serrated adenoma.
Methods—The frequency of K-ras codon 12 point mutation in 20 serrated adenomas, five atypical hyperplastic polyps, and 58 sporadic polypoid adenomas was investigated by nested polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) methods.
Results—Although most of the serrated adenomas were large (average size 11.4 mm) and polypoid, K-rascodon 12 point mutation was detected in only one of the 20 (5%), which is a significantly lower frequency than that in sporadic polypoid adenomas (18/60; 30%) (p = 0.017). No mutation was detected in the atypical hyperplastic polyps. Three of 20 (15%) serrated adenomas contained a focus of carcinoma in situ, indicating their malignant potential and the existence of a serrated adenoma-carcinoma sequence, but no mutation was detected in the foci of carcinoma in situ.
Conclusions—K-ras mutation is uncommon in serrated adenomas, indicating a different spectrum of genetic alterations in these lesions from those in typical polypoid sporadic adenomas. This subtype of colorectal adenoma represents a new genetic pathway in the histogenesis of colorectal carcinoma.
- serrated adenoma
- colorectal adenoma
- K-ras mutation
- PCR-RFLP
Statistics from Altmetric.com
Serrated adenoma is a new morphological subtype of colorectal adenoma, as proposed by Longacre and Fenoglio-Preiser in 1990.1 The polyp combines the morphological features of hyperplastic and adenomatous epithelium. It shows a serrated glandular architecture reminiscent of hyperplastic polyps, but the cytological features (incomplete mucinous differentiation, pseudostratified and enlarged spindle shaped nuclei) and lack of surface maturation indicate its neoplastic nature. It has been separated from mixed polyps comprising a mixture or “collision” of readily identified hyperplastic and adenomatous components.1 Although the incidence of serrated adenomas has been estimated as less than 1% of all colorectal polyps, malignant potential is thought to exceed that of typical adenomas.1 Attention has also been focused on the relation between giant hyperplastic polyps and hyperplastic polyposis.2 ,3 Genetic changes in these lesions have not been investigated previously.
APC and K-ras mutations are important alterations in the morphogenesis of colorectal adenomas,4 ,5 the APC mutation initiating microadenoma5 and K-ras mutations, predominantly in codon 12,4 ,6 ,7 being associated with progression.4 In this study, we focused on analysis of K-ras codon 12 point mutations in serrated adenomas of the colon and rectum and compared them with sporadic polypoid tubular adenomas. K-ras codon 12 mutation was found to be infrequent in serrated adenomas, indicating a different genetic pathway of change in this new subtype of colorectal adenomas.
Methods
SPECIMEN
Formalin fixed, paraffin embedded blocks were obtained from endoscopically resected serrated adenomas (20), atypical hyperplastic polyps (five), and sporadic polypoid tubular adenomas (60, including ones in our previous study8). Serrated adenomas were defined as polyps composed of serrated glands reminiscent of hyperplastic polyps on low power magnification, but the serrated epithelium showed neoplastic cytological atypia: pseudostratification of enlarged and/or elongated spindle shaped nuclei, loss of mature goblet cells, a dark eosinophilic cytoplasm and lack of surface maturation, and lack of the thickened collagen table at the free surface.1 The distinction between serrated adenoma and hyperplastic polyps was not always straightforward. All uncertain cases were grouped separately as “atypical hyperplastic polyps” (AHP). Serrated adenomas were either pure (SA) or accompanied by AHP (SA+AHP) or typical hyperplastic polyps (SA+HP). Lesions that appeared as a “collision” or intermingling of typical hyperplastic and adenomatous epithelium1 were carefully excluded from the study. Serial sections 3 and 10 μm thick were prepared for each specimen. The 3 μm thick section was used for haematoxylin and eosin staining and the 10 μm thick section for DNA extraction.
DNA EXTRACTION AND ANALYSIS OF K-RAS CODON 12 MUTATION
DNA was extracted as described previously.8 ,9 When a lesion was histologically heterogeneous (composed of serrated adenoma and/or hyperplastic polyps, atypical hyperplastic polyps, carcinoma in situ), DNA was extracted separately from each individual area by microdissection. DNA samples from normal colorectal tissue were also extracted if present in the specimen. The K-ras codon 12 point mutation was analysed by the nested polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. PCR amplification was performed using the primers and conditions described by Ooshima et al,10 except that annealing was carried out for 1.5 minutes. In each PCR run, three control reactions were included: (a) negative control (containing no template DNA); (b) normal control (normal human placental DNA); (c) positive control (AsPcl pancreas cancer cell line DNA which contains a homozygously mutant K-ras codon 12: GTT to GAT11). RFLP was carried out by established methods8-10: PCR products (10 μl) were incubated with 1 μl Mval (Takara, Kyoto, Japan) at 37°C for six hours, electrophoresed in 3.5% NuSieve agarose gel (FMC Bioproducts, Rockland, ME, USA), and stained with ethidium bromide. The wild type PCR products were cleaved, resulting in a band of 86 bp fragments (fig 1). In each electrophoretic run, a normal control (normal human placental DNA) always showed a single band of 86 bp fragments, ruling out the possibility of partial digestion with the restriction enzyme. Any PCR products containing 106 bp fragments (not cleaved by Mval) were considered to contain a mutation at codon 12.

Nested polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) analysis of K-ras codon 12 mutations in serrated adenomas and sporadic traditional polypoid adenomas. The wild type and mutant fragments were detected at 86 and 106 bp respectively. M, ΦX174/HaeIII DNA size marker; lane C1, positive mutant control (AsPcl1) homozygous for mutant K-ras at codon 12 showing uncleaved mutant band (106 bp) only; lane C2, normal control (normal human placental DNA) showing cleaved wild type band (86 bp) only; lanes A1 to A4, DNA samples from polypoid adenomas showing both mutant and wild type bands (heterozygous); lanes S1 to S4, DNA samples from serrated adenoma with wild type band only; lane N1, DNA sample from normal colorectal tissue with wild type band only. No negative control is shown.
STATISTICAL ANALYSIS
Statistical analysis was by Fisher’s exact test. A p value of less than 0.05 was regarded as significant.
Results
MORPHOLOGICAL FINDINGS
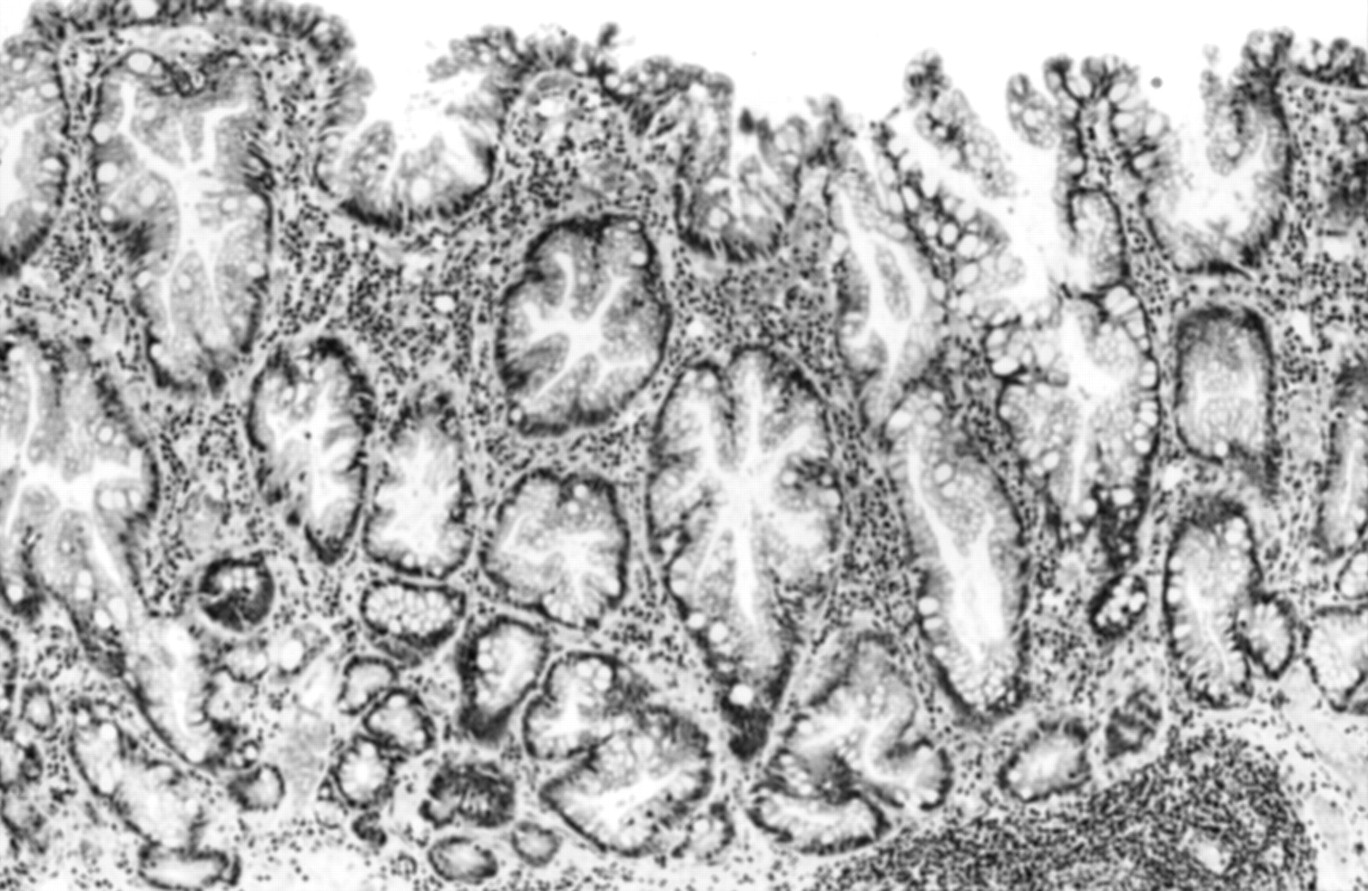
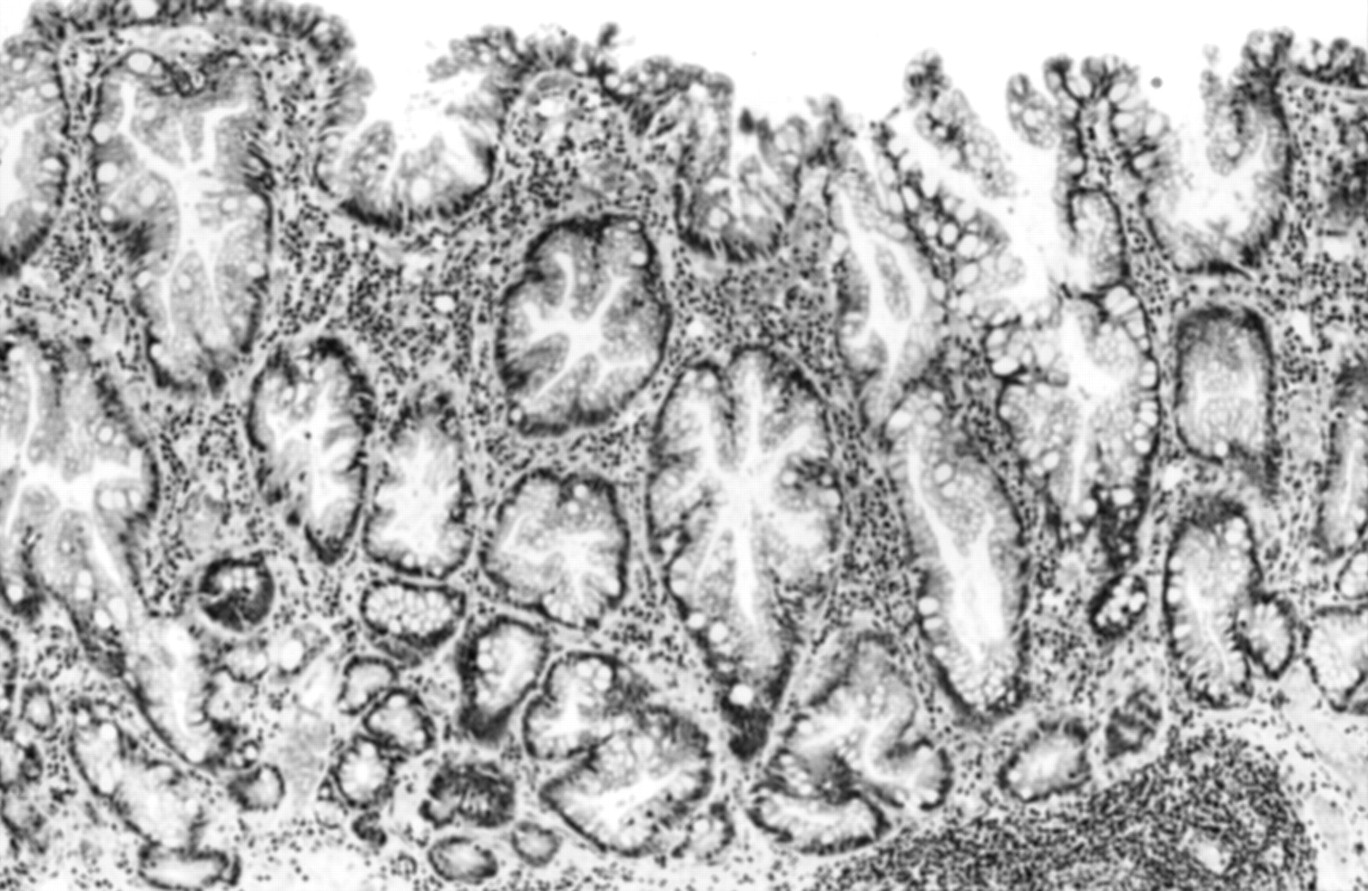
Of the 20 serrated adenomas, 11 (55%) were almost histologically pure (SA) (fig 2), six (30%) were accompanied by atypical hyperplastic polyps (SA+AHP), and three (15%) were accompanied by traditional hyperplastic polyps (SA+HP) (figs 3 and 4, table 1). The mean (SD) size of the serrated adenomas including accompanying atypical hyperplastic polyps or hyperplastic polyps was 11.4 (3.9) mm and that of the serrated adenomatous component alone was 9.6 (5.0) mm. Sixteen of 20 (80%) were protuberant macroscopically. In protuberant polyps, serration was prominent and seen throughout most if not all the lesion (figs 2 and 3), but it tended to be slight in sessile lesions (fig 4). Two lesions in SA+AHP and one in SA+HP contained a focus of severe atypia equivalent to carcinoma in situ (fig 3). This comprised closely spaced serrated glands with focal back to back or pseudocribriform appearance and round to ovoid vesicular nuclei with prominent nucleoli. Atypical hyperplastic polyps (including AHP in SA+AHP) were histologically characterised by irregularly branched serrated glands with loss of goblet cells and the presence of numerous dystrophic goblet cells, oval to spindle shaped nuclei with slight pseudostratification, and a small degree of surface maturation (fig 5). The average size of atypical hyperplastic polyps was 5.2 mm (all of them were less than 10 mm), but two of the five (40%) were protuberant.

(A) Whole mount view of serrated adenoma that was almost pure histologically, measuring 9 mm in size with subpedunculated configuration (original magnification × 2.5). (B) The serrated glandular architecture is reminiscent of a hyperplastic polyp but its cytology (pseudostratified enlarged and/or spindle shaped nuclei with loss of goblet cells) and lack of surface maturation indicate its neoplastic nature (original magnification × 50).

(A) Whole mount view of serrated adenoma accompanied by hyperplastic polyps and focus of severe atypia, equivalent to carcinoma in situ, measuring 12 mm in size with pedunculated configuration (original magnification × 2.5). (B) Serrated adenoma with enlarged nuclei with prominent nucleoli (original magnification × 40). (C) Hyperplastic polyp accompanied by serrated adenoma located at the periphery of the lesion (indicated by the small arrows in (A)) (original magnification × 25). (D) Focus of carcinoma in situ located at the centre of the lesion (indicated by the large arrows in (A)) (original magnification × 50).

Serrated adenoma adjoining hyperplastic polyp, measuring 8 mm with sessile configuration (original magnification × 13.2). Area of serrated adenoma (left half of the lesion) measuring 5 mm, showing slight but definite luminal serration. K-ras mutation was detected only in the area of serrated adenoma.
Number, size and macroscopic type of lesion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Atypical hyperplastic polyp showing irregular glandular structure, numerous dystrophic goblet cells, and a slight degree of surface maturation (original magnification × 25).
K-RAS CODON 12 POINT MUTATION
The K-ras mutation in serrated adenomas was detected in one of 20 (5%) (table 2). The serrated adenoma with a K-ras mutation was a sessile 8 mm size lesion accompanied by hyperplastic polyps (SA+HP) (fig 4). The serrated adenoma component measured 5 mm. DNA was extracted separately from the areas of serrated adenoma and hyperplastic polyp, and the mutation was detected only in the serrated adenoma. No mutation was detected in atypical hyperplastic polyps, foci of carcinoma in situ, or normal colorectal tissue. The frequency of K-ras mutation in traditional polypoid tubular adenomas was 30% (18/60). Mutation rate increased with size; 48% (12/25) of adenomas larger than 10 mm had a mutation. Statistical significance was observed between polypoid adenomas (30%) and serrated adenomas (all SA foci) (5%) (p = 0.017), and trend between polypoid adenomas and atypical hyperplastic polyp (0%) (p = 0.18).
Frequency of K-ras codon 12 mutations in serrated adenomas, atypical hyperplastic polyps and sporadic polypoid adenomas
Discussion
The frequency of K-ras codon 12 mutation in serrated adenomas was 5%, which is significantly lower than that of control sporadic polypoid adenomas (30%). K-ras mutation, predominantly in codon 12, may result in subclonal evolution of colorectal adenomas, represented morphologically as an increase in size and grade of atypia.12 About 60–70% of adenomas larger than l0 mm have been shown to have a K-rasmutation.4 ,13 However, this observation is based on sporadic polypoid colorectal adenomas,14 whereas K-ras mutation is infrequent in flat type adenomas.15 ,16 The role of K-ras point mutation in morphogenesis of colorectal adenomas has not been elucidated in detail, although it is known to up regulate mitogenic signal transduction pathways.17 The high mutation frequency in polypoid adenomas as opposed to flat adenomas suggests that K-ras mutation may be related not only to increase in size but more specifically to polypoid adenoma growth.8 ,16 The single serrated adenoma found to be positive for K-ras mutation in our study was a small and sessile lesion (the whole lesion measured 8 mm, but the area of serrated adenoma was confined to 5 mm), and no mutation was found in other larger protuberant polyps. Our data indicate that K-ras mutation is not related to morphogenesis of serrated adenomas and indicate a different spectrum of genetic alterations in these lesions.
Although the concept of serrated adenoma has been generally accepted, their diagnosis may not be straightforward.2 A histological spectrum exists within serrated adenomatous epithelial proliferations, ranging from those that are more like traditional adenoma to those that are more like hyperplastic polyp.2Further histological subclassification of serrated adenoma may be needed. All serrated adenomas in this study fulfilled the histological criteria of the original report.1 Some traditional adenomas produce a pattern superficially reminiscent of luminal serration by virtue of multiglandular budding and branching, and they were excluded from the study. Serrated adenomas with an adenoma-like appearance by virtue of definite but slight serration (fig4) were included, and accounted for the single instance of a serrated adenoma with K-ras mutation. At the other end of the spectrum, serrated polyps with indefinite adenomatous features were grouped as atypical hyperplastic polyps. They could not be judged as serrated adenoma because of incomplete but definite surface maturation. Like typical hyperplastic polyps, they were small, but two of the five were protuberant. Atypical hyperplastic polyps showed glandular irregularities and dystrophic goblet cells as described in dysplasia in ulcerative colitis.18 The presence of such foci in 30% of the serrated adenomas suggests that the atypical hyperplastic polyp may belong within the spectrum of serrated adenoma or its precursor lesion.
Intramucosal carcinoma has been reported to occur in 10% of serrated adenomas, indicating that serrated adenomas have significant malignant potential.1 In our material, 15% of the serrated adenomas included a focus of severe atypia, equivalent to carcinoma in situ. Cases of invasive carcinoma with distinct serrated configuration have been reported.2 ,19 Colorectal carcinomas are thought to arise through three main histogenic pathways: (1) classical of polypoid adenoma-carcinoma sequence20 ,21; (2) flat adenoma-carcinoma sequence22 ,23; (3) de novo cancerisation.24 ,25 Serrated adenoma-carcinoma sequence would represent a fourth pathway. With regard to the associated genetic alterations, K-ras mutation is involved in polypoid adenoma-carcinoma sequence, but not in the flat adenoma-carcinoma sequence (as above) or in intramucosal carcinomas thought to arise de novo.26 These differences allow the K-rasmutation to serve as genetic marker of histogenesis.27Since the frequency of K-ras mutation in colorectal cancers is about 50%28 (30–40% with a mutation at codon 124 ,6 ,7), at least this proportion would have originated from polypoid adenomas. The serrated adenoma-carcinoma sequence will apply to a subset of these cancers lacking a K-rasmutation.
Acknowledgments
We thank our laboratory staff for their excellent technical support. The AsPcl cell line was provided by Dr Ken Yamaguchi (National Cancer Center Research Institute, Tokyo, Japan).