Article Text

Abstract
Aim (1) A pilot study to determine the accuracy of interpretation of whole slide digital images in a broad range of general histopathology cases of graded complexity. (2) To survey the participating histopathologists with regard to acceptability of digital pathology.
Materials and methods Glass slides of 100 biopsies and minor resections were digitally scanned in their entirety, producing digital slides. These cases had been diagnosed by light microscopy at least 1 year previously and were subsequently reassessed by the original reporting pathologist (who was blinded to their original diagnosis) using digital pathology. The digital pathology-based diagnosis was compared with the original glass slide diagnosis and classified as concordant, slightly discordant (without clinical consequence) or discordant. The participants were surveyed at the end of the study.
Results There was concordance between the original light microscopy diagnosis and digital pathology-based diagnosis in 95 of the 100 cases while the remaining 5 cases showed only slight discordance (with no clinical consequence). None of the cases were categorised as discordant. Participants had mixed experiences using digital pathology technology.
Conclusions In the broad range of cases we examined, digital pathology is a safe and viable method of making a primary histopathological diagnosis.
- DIGITAL PATHOLOGY
- DIAGNOSTICS
- SAFETY
Statistics from Altmetric.com
Introduction
Whole slide imaging (WSI) converts a physical glass slide to a digital image allowing pathologists to view histological sections digitally rather than with a conventional microscope. Over the last decade, the technical quality has improved such that its use is increasingly contemplated for educational, research and archival purposes1 and for primary diagnosis.2 Several studies show very favourable comparisons between digital pathology and conventional glass microscopy as a diagnostic tool.3–8 A number of factors have limited the roll-out and acceptance of WSI in primary diagnosis. These include scan time, WSI exploration time, storage, cost and lack of robust validation. The latter has recently been addressed by the College of American Pathologists9 who make a total of 12 guideline statements. The aim of this pilot study was to evaluate the clinical suitability of digital pathology in routine practice in a broad range of cases of graded complexity and also to survey the participants’ experiences using this technology.
Materials and methods
Cases were selected to represent increasing levels of complexity based on the competency based framework for graded responsibility for Specialist Registrars in Histopathology and Cytopathology published by the Joint Committee on Pathology Training of the Royal College of Pathologists (UK).10 This categorises surgical pathology cases into four levels of complexity (1–4 where 4 is the highest level of complexity on the scale). In addition, we included 5 cases within each subspecialty considered higher level than level 4. A SNOMED code search was performed of potentially suitable cases which had been reported at least 12 months previously (therefore giving a washout period of at least 12 months). Slides were retrieved and reviewed by JPH and SLK and cases which were technically impaired such as faded or artefacted were excluded. Twenty-five cases were finally identified from four different anatomical sites—gastrointestinal tract, head and neck, female reproductive system and skin (table 1). The mean age of the patients was 48 years (range 5–86 years).
Illustrates the range of cases selected for this study
The glass slides were digitally scanned as whole slide images at 40× using a Hamamatsu Nanozoomer (Hamamatsu UK). Any marks that had been placed on the slides previously by the reporting pathologist were removed prior to scanning. Digital images were uploaded to the PathXL cloud platform (PathXL, UK) allowing the images to be managed and rapidly viewed remotely via the PathXL web viewer. Authorised users were able to login to the PathXL digital pathology platform using a secure username and password, and review each slide in the digital slide series via a standard web browser interface (e.g., Internet Explorer, Firefox, Safari, etc). The entire high resolution slide could be navigated and viewed at any magnification up to 40× objective magnification using the PathXL web viewer. This provides a range of tools to select and move the slide, change magnification, annotate the slide and record diagnoses, on screen and from any location on a computer with an internet connection. All images were reviewed on a range of standard monitors located inside and outside of the hospital.
The digital slides were made available to the original reporting pathologist along with the original demographic details, clinical information and macroscopic description, but the consultants were blinded to their original diagnosis.
The reporting pathologist was then asked to record a digital pathology diagnosis which was compared with the original glass diagnosis by an independent pathologist and classified as concordant (digital pathology and original diagnosis the same), slightly discordant (no clinical or prognostic implications) or discordant (difference with clinical and/or prognostic implications for the patient). In discrepant cases, the glass slides and digital images were reviewed and the preferred diagnosis was recorded.
The participants were surveyed with regard to their experiences using digital pathology (table 3).
Results
There was concordance between the original light microscopy diagnosis and digital pathology diagnosis in 95 of the 100 cases while the remaining 5 cases showed slight discordance. None of the cases were categorised as discordant. In the 5 cases where there was a slight discordance, reassessment of the glass slides and WSI by the reporting pathologist was performed. In each case, the original light microscopic diagnosis was preferred. Table 2 summarises the 5 slightly discordant cases and the reasons for the discordance.
List of cases where there was a discrepancy between glass and digital diagnoses
Case 1 (figure 1) was a vocal cord biopsy in a middle-aged male smoker with hoarseness and vocal cord thickening. The original diagnosis was of mild dysplasia whereas the diagnosis using WSI was Reinke's oedema with no dysplasia. After reassessment it emerged that there had been a previous biopsy showing dysplasia and it was in the context of minimal morphological atypia in addition to review of the previous slides that the diagnosis of mild dysplasia had been made originally. The digital image was felt to be of similar quality to the glass slides. This illustrates the importance of a complete patient history and also the difficulty in assessing dysplasia in this region which is known to be subjective and subject to intraobserver and interobserver reproducibility due to the insufficiency of validated morphological criteria and the biological nature of dysplasia.11

Case 1, vocal cord biopsy (×20), H&E.
Case 2 (figure 2) was a gastric biopsy in a patient with a history of biopsy-proven high grade dysplasia. The original diagnosis was of reactive gastritis with a small focus of intestinal metaplasia. The WSI diagnosis was reactive gastritis only. Review of the digital images in this case confirmed the presence of a small focus of intestinal metaplasia which had been overlooked during the initial assessment of the WSI. The pathologist felt that the focal abnormality was missed due to lack of experience scanning digital images rather than an issue with image quality. While gastric intestinal metaplasia is considered a preneoplastic condition, the relative risk is low and unless extensive or of incomplete phenotype, is not an indication for further investigations.12
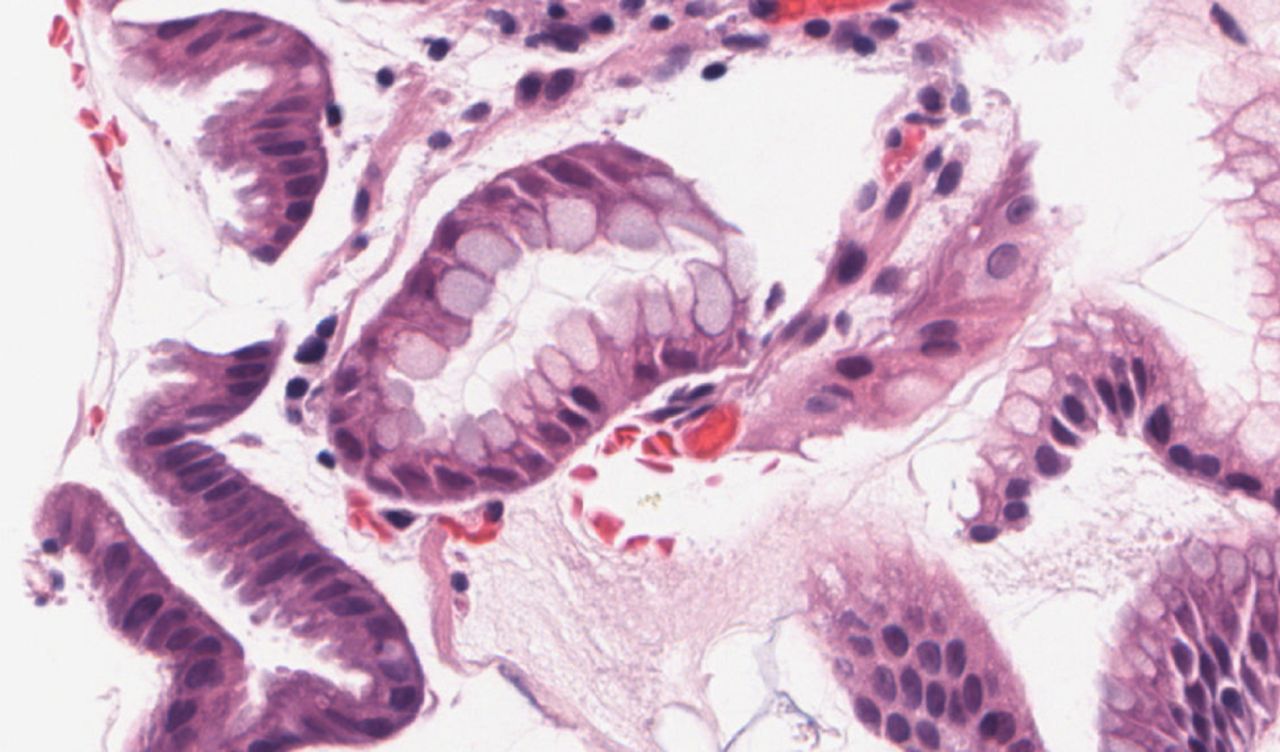
Case 2, gastric biopsy (×40), H&E.
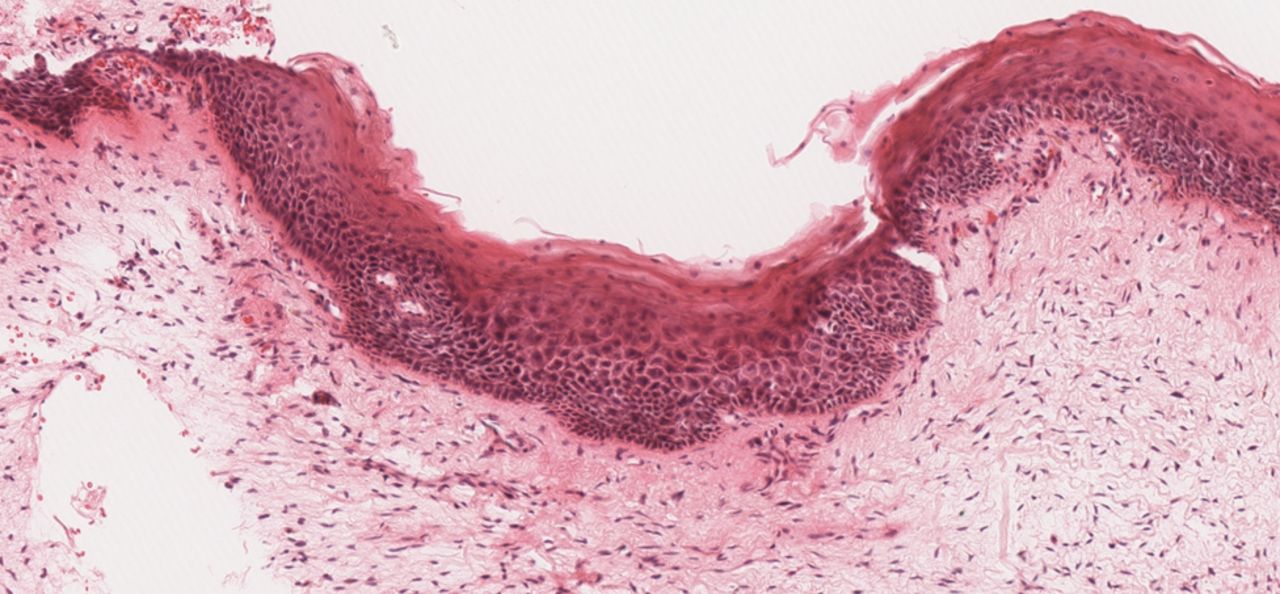
Case 3 (figure 3) was a colposcopic punch biopsy originally reported as cervical intraepithelial neoplasia I (CIN I) and the WSI diagnosis was koilocytosis. Upon review the original diagnosis was preferred. Distinguishing between koilocytosis and CIN I is an area with significant intraobserver and interobserver variability, even on glass.13 In fact, there is an increasing tendency to categorise koilocytosis and CIN I together as a low grade squamous intraepithelial lesion rather than diagnose these separately; management and follow-up of koilocytosis and CIN I is identical.

Case 3, cervical biopsy (×40), H&E.
Case 4 (figure 4) and case 5 had similar histological appearances. Both were originally diagnosed as neurofibromas via light microscopy and subsequently as neurotised intradermal naevi using digital WSI assessment. In both cases the diagnosis was discrepant but benign. Differentiating between a neurofibroma and a neurotised intradermal naevus is normally achievable with light microscopy alone, but the distinction can sometimes be difficult without the use of immunohistochemistry. Immunohistochemistry was not used for the original diagnosis in these cases but was performed during this study to confirm the diagnosis (Melan-A was negative in both cases). In both cases, after review of the glass slide and WSI images and the use of additional immunohistochemistry (Melan-A) the original diagnosis was preferred. Despite the benignity of these 2 entities, it is important to differentiate these lesions in some situations because multiple neurofibromas may be a sign of neurofibromatosis (von Recklinghausen disease) and a superficially sampled desmoplastic melanoma can resemble a neurofibroma.14

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 4, skin biopsy (×5), H&E.
In none of the 5 cases was image quality considered to be responsible for the minor discrepancies. The mean washout period for concordant cases (1.8 years) and discordant cases (1.7 years) was similar and would not account for differences in interpretation.
Survey of pathologists’ experiences using digital pathology
Discussion
Digital pathology is used for routine primary diagnosis in a number of settings.15 However, within the USA, the Food and Drug Administration regards WSI as a class III (highest risk) medical device16–18 and has approved WSI in restricted circumstances only such as in the quantification of breast cancer markers.19
We set out to establish whether digital pathology was a viable and safe alternative to conventional light microscopy in the diagnosis of a broad range of routine surgical pathology cases. We have shown an acceptable concordance rate of 95% between conventional light microscopic assessment and digital pathology assessment. This rate of concordance is in line with other pilot studies of similar design, which have shown concordance rates ranging from 90% to 95%.4 ,7 ,20–24
In our series, 5 cases had slight discordances judged not to be of clinical relevance. In 4 of the 5 cases where there was a slight discordance between the glass slide diagnosis and the WSI assessment; this was due to different interpretation of subtle or borderline pathology. In one case a slight discordance occurred because the diagnostically relevant area of the slide had been overlooked, which may be attributed to a lack of experience with the use of digital pathology.
Our secondary objective was to assess the participants’ experiences with digital pathology. This was certainly mixed. Most participants felt digital pathology was slower to use than light microscopy and were not enthusiastic about using it for routine diagnosis.
A strength of our study was that rather than comparing the WSI diagnosis with a consensus diagnosis, a method used in other studies,7 we employed an approach similar to that advocated by the College of American Pathologists, among others9 ,20 where we asked the same pathologist who made the original diagnosis to review the digitally scanned image in order to avoid interobserver variability. A limitation of our study was that all specimens were biopsy or small resection specimens. This is not entirely reflective of the full spectrum of reporting which can include larger cases requiring review of multiple slides and larger areas of tissue.
In conclusion, in the range of cases we examined, digital pathology is a safe, viable method of making a primary histopathological diagnosis.
Take home messages
-
Digital pathology is a safe alternative to light microscopy in the broad range of general pathology cases we examined.
-
Minor discrepancies that occurred mostly involved the interpretation of subtle or borderline pathology.
-
Participating pathologists had mixed experiences using digital pathology and would prefer light microscopy for routine practice.
References
Footnotes
-
Contributors The concept of this study was created by JPH and PWH. All authors contributed to the script and agreed to the final version.
-
Competing interests PWH is Vice Principal for Research and Development and Director in PathXL.
-
Provenance and peer review Not commissioned; externally peer reviewed.