Article Text

Abstract
Aims Mycophenolate-associated colitis has been previously reported to show patterns of colonic mucosal injury mimicking a host of conditions, including graft-versus-host disease, ischaemia and inflammatory bowel disease (IBD). The aim of this study is to characterise, semiquantitatively, pathological changes of mycophenolate mofetil (MMF) mucosal injury.
Methods Seven transplant patients receiving MMF who underwent colonoscopic examination and biopsy were identified retrospectively over a 2-year period. Multiple histologic parameters, including architectural distortion, cryptitis, stromal active inflammation, individual damaged crypts (IDC) and crypt apoptotic figures were evaluated in the biopsies semiquantitatively. Where biopsy site was identified, the parameters were assessed separately in biopsies from right and left colon.
Results All cases showed mixed patterns of mucosal injury. All seven cases showed focal architectural distortion (in 58% of fragments per case), focal cryptitis (mean 3.0 foci per case), increased crypt apoptosis (mean 26.5/100 crypts) and IDC (mean 3.0 foci). Focal changes resembling acute self-limited colitis were noted in three cases. Possible proximal accentuation of some changes was noted with right side biopsies tending to show greater crypt apoptotic activity and more foci of architectural distortion. Three cases showed dual pathology (two with cytomegalovirus (CMV) infection and one with IBD).
Conclusions Although a wide spectrum of changes may be seen in MMF-associated colitis, important microscopic clues include a mixed pattern of injury (typically a combination of crypt apoptosis, isolated crypt damage and architectural distortion), and possible proximal accentuation of pathologic changes. The need for clinical correlation and follow-up is emphasised by the occurrence of dual pathology in patients treated with MMF.
- Colitis
- Transplantation
- Infectious Intestinal Disease
- Inflammatory Bowel Disease
Statistics from Altmetric.com
Introduction
Mycophenolate mofetil (MMF) is a newer-generation immunosuppressive agent routinely used as part of the prophylactic and treatment regimen of allograft rejection in organ transplant recipients. A significant minority of patients (up to 52.5%) experience gastrointestinal symptoms with diarrhoea as the most frequently reported adverse effect.1 The histologic features of mycophenolate-associated colitis (MAC) have recently been characterised. Previous studies have been descriptive, reporting patterns of mucosal injury mimicking a host of conditions, including graft-versus-host disease, ischaemia and inflammatory bowel disease (IBD).2 ,3 The aim of this study is to further characterise and quantify the pathological changes of mycophenolate mucosal injury, and to highlight the need to consider or exclude dual pathologies.
Methods
Colonic biopsies from all transplant patients with clinical diagnosis of MMF-associated colitis who underwent colonoscopic examination and biopsy at Sir Charles Gairdner Hospital over a 24 month period between January 2009 and December 2010, inclusive, were identified and reviewed. Multiple histologic features were evaluated in the biopsies semiquantitatively. Crypt architectural distortion (IBD-like changes) was assessed and related to the number of fragments involved. Foci of cryptitis and focal acute self-limiting colitis-like changes (characterised by lamina propria neutrophilic infiltration) were counted. Individual damaged crypts (IDC, or ‘dilated damaged crypts’, as previously described by Parfitt et al3) were quantified according to number of crypts and also percentage of fragments bearing these crypts. Apoptotic figures were counted per 100 crypts (with >5/100 crypts considered to be abnormal4). Where biopsy site was identified, the parameters were assessed separately in biopsies from right and left colon.
Results
The clinicopathologic features are described in table 1. Seven transplant patients on MMF who underwent colonoscopy and biopsy (five renal transplant recipients, one liver transplant and one bone marrow transplant) were identified. The mean age was 46.1 years (range 24–63), with male:female ratio of 3 : 4.
Clinicopathologic features of MMF-associated colitis
The clinical indication in all cases was watery diarrhoea. The mean number of biopsy fragments per case was 11 (range 4–22). Six of the seven cases had separately submitted right and left colonic biopsies (mean number of fragments per biopsy site, 5).
All seven cases exhibited a variety of microscopic changes, including focal architectural distortion, focal cryptitis, increased crypt apoptosis and IDC.
IBD-like changes
In all cases, there was architectural distortion characteristic of IBD, with crypt shortening, branching and dropout (figure 1). Crypt disarray was discontinuous, and involved a mean of 58% fragments per case.

Crypt shortening and branching resembling inflammatory bowel disease. This figure is only reproduced in colour in the online version.
Focal cryptitis
Active crypt inflammation in the form of cryptitis, or crypt abscess, was observed in all seven cases, and was not restricted to fragments with distorted architecture, and was very focal (mean 3.0 foci, range from 1 to 7 foci).
Acute self-limited colitis
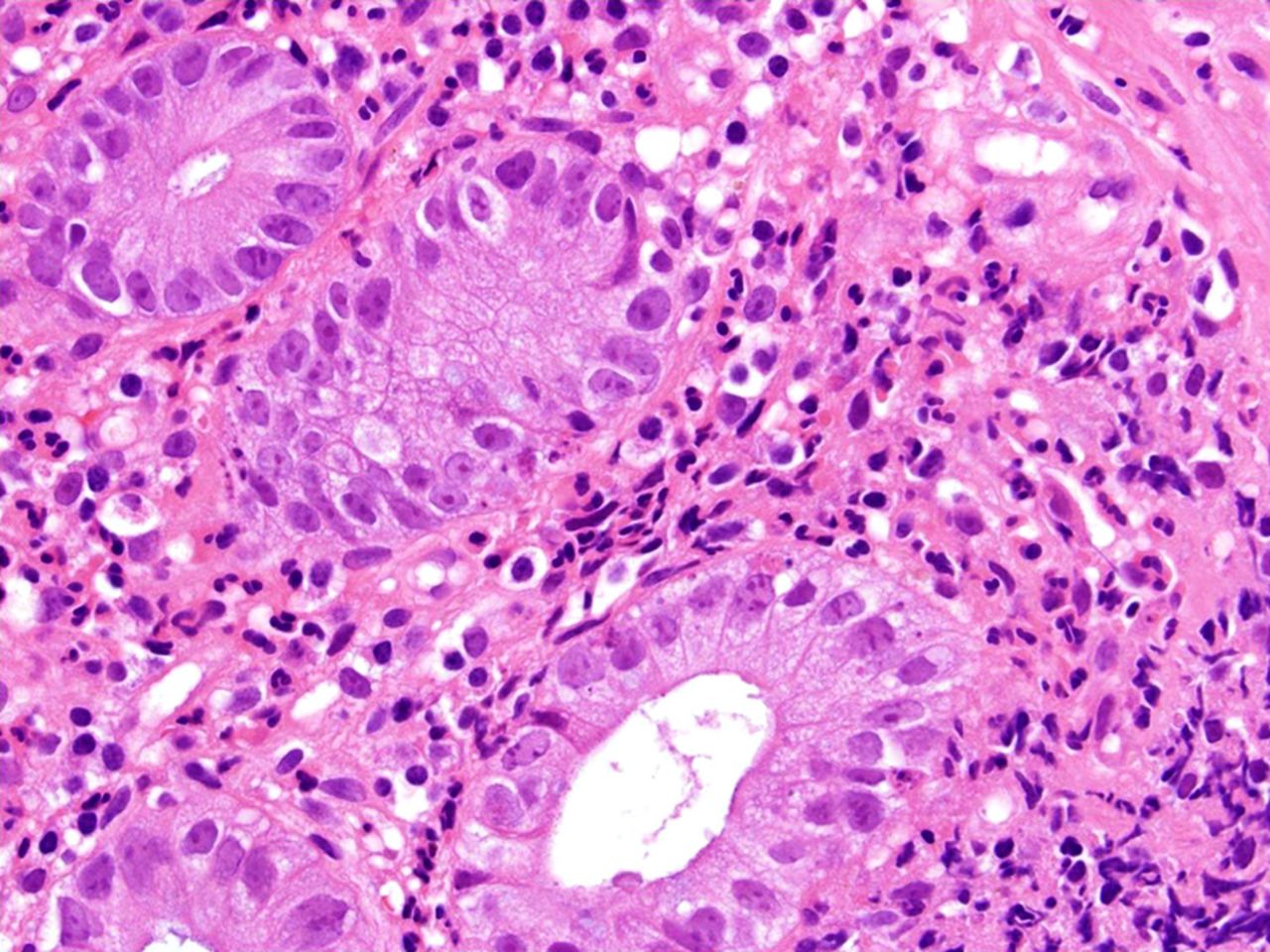
Changes resembling acute self-limited colitis were noted in three cases (figure 2), with two showing involvement of both right and left side biopsies (cases 3 and 4).

Active inflammation in the stroma resembling focal active colitis. Note, numerous apoptotic figures within the crypts. This figure is only reproduced in colour in the online version.
Individual damaged crypts
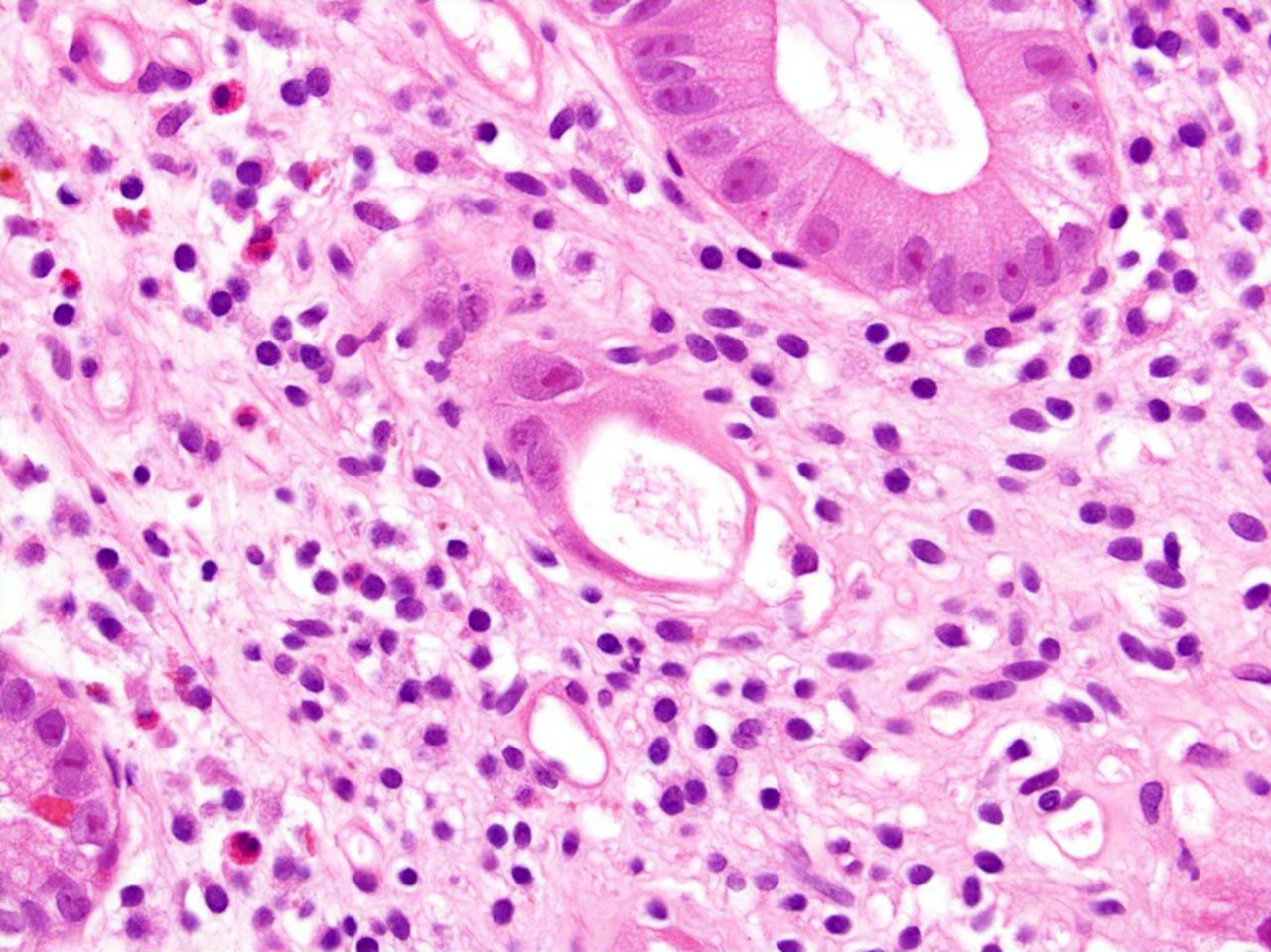
A prominent feature was the presence of IDC lined by either atrophic-flattened epithelium (ischaemic-look or ‘withering crypts’, figure 3), or cells with abundant eosinophilic cytoplasm (regenerative-look). The majority were of normal calibre and possessed luminal secretions, apoptotic debris or small numbers of neutrophils, with occasional glands showing microcystic dilatation. These damaged crypts characteristically occurred singly and in a background of normal crypts. No vasculitis or microthrombi were identified. A mean of 3.0 foci of IDC per biopsy were identified.

Individual damaged crypt characterised by normal calibre gland lined by atrophic-appearing epithelium. This figure is only reproduced in colour in the online version.
Apoptosis
In all cases, there was greatly increased apoptosis in the deep crypts (mean 26.5/100 crypts, range 12–40/100 crypts, figure 2).
Location
There appeared to be greater involvement of right colonic biopsies by IBD-like changes with relative sparing of the left colon and rectum (mean 87.8% vs 7.4% of fragments). Similarly, more crypt epithelial apoptotic figures were noted in biopsies from the right than the left side (13.8 vs 6.8). These are observed trends only, and statistical analysis was not performed due to the small numbers in this series. There did not appear to be a significant difference in the mean number of IDC (p=1.0) or foci of cryptitis between the left and right colonic biopsies (table 2).
Comparison of pathologic changes in right and left side colon biopsies (cases 1–6)
Cases with dual pathology
There were three of seven cases in this current series with dual pathology. In cases 5 and 6, characteristic cytopathogenic changes of CMV infection (figure 4) were noted and confirmed by immunohistochemistry, although only one of these was clinically suspected. The remaining case (case 7) involved a 41-year-old female renal transplant patient on MMF with persistent lower gastrointestinal (GI) symptoms including per rectal (PR) bleeding over 3 years. Repeated colonoscopies over 3 years showed persistent ileal ulceration with varying degrees of left-sided colitis and ulceration. The first two sets of corresponding biopsies revealed non-specific ileitis and active colitis with preserved architecture. Architectural disarray was noted in the two subsequent biopsies which also showed more established active chronic colitis in addition to IDC, and increased apoptosis. MMF was discontinued with a short-lived improvement in symptomatology. Repeat colonoscopy and biopsy demonstrated progressive ileocaecal and colonic ulceration including rectal involvement and active chronic colitis. The persistence of endoscopic and microscopic changes raised the possibility of denovo IBD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CMV-related cytopathogenic changes are seen in the endothelial lining of the small vessel. This figure is only reproduced in colour in the online version.
Discussion
Mycophenolate mefotil has become part of the standard immunosuppressant regime used in organ transplant patients. MMF requires hepatic metabolism for conversion to its active isomer mycophenolic acid (MPA). MPA inhibits inosine monophosphate dehydrogenase, an enzyme necessary for de novo purine synthesis. As this is the main pathway for purine synthesis (and hence, DNA synthesis and replication) in T and B lymphocytes, MPA mediates immunosuppression by inhibiting lymphocytic proliferation.1 ,2 Enterocytes are also highly dependent on de novo purine synthesis, and hence, susceptible to MPA inhibition. The dose-related gastrointestinal toxicity of MMF is related to the damage of enterocytes. Diarrhoea is the most commonly reported adverse effect, reported in up to 36.1% of patients.1 Diarrhoea is not an entirely inconsequential side effect, and may necessitate physician-directed reduced dosing or drug cessation, lead to non-compliance, and in severe cases result in a wasting illness.5 Dose adjustments are required in approximately 60% of patients treated with MMF due to side effects, such as leucopenia and diarrhoea.6 Enteric-coated preparations may also be used.
The histologic features of MMF-associated colitis have been well characterised. Case reports and series describe changes mimicking graft vs host disease (GVHD), IBD, ischaemia or acute colitis. Parfitt et al3 reported a spectrum of changes, including crypt distortion, stromal oedema and inflammation, dilated damaged crypts and increased crypt apoptosis. Dalle et al7 similarly described patchy crypt disarray, mild active inflammation, focal dilated and inflamed crypts, and increased mucin secretion, although increased crypt apoptosis was not a feature. Selbst et al2 were able to categorise their cases as normal/near-normal (31%), IBD-like (28%), GVHD-like (19%), ischaemia-like (3%) and self-limited colitis-like (16%).
We found a similar spectrum of morphological features, although we report two additional diagnostic features not previously documented. A characteristic feature of MMF-related colitis in our study was a ‘mixed pattern of injury’ not easily placed in any ‘pure’ or classic disease pattern. All cases demonstrated a minimum of chronic architectural disarray, increased crypt apoptosis, cryptitis and isolated damaged crypts in variable degrees, with acute inflammation of the lamina propria (active self-limited colitis-like) being more inconsistent findings. Microscopic changes were often patchy within and between fragments.
Focal active colitis (FAC) has been associated with medication-induced injury and early manifestations of IBD, in particular, Crohn's disease. However, the definition appears rather vague in the literature ranging from a single crypt abscess, single focus of cryptitis, to multiple discrete foci. Depending on the definition, one might choose the degree of cryptitis seen in our cases that may fit into the spectrum of FAC.
The other potentially useful finding in our study was the gradient of some changes from proximal to distal colon. Previous studies have not documented site-specific changes. The current study has shown some differences between biopsies from the right colon and left colon. In particular, architectural damage was more severe and diffuse, and there was a greater degree of crypt apoptosis in the proximal colon. These, however, are observed trends, and the cohort was too small for meaningful statistical analysis. Nevertheless, this would be an interesting feature to investigate in future larger studies. The reasons for the proximal accentuation are unclear, although one possibility is the enterohepatic recycling of MMF which may deliver greater concentrations to proximal large-bowel segments.
IDC or ‘dilated damaged crypts’, have previously been described by Parfitt et al3 and Dalle et al7 as a relatively specific finding in antimetabolite drug-induced colitis. We note in our study that many damaged crypts were of normal calibre, although otherwise showing the same morphology as dilated damaged crypts. The aetiology of such damaged crypts is uncertain, although the very focal nature of damage (single crypts) and ischaemic appearance of some glands raises the possibility of microvascular injury. However, no capillaritis or microthrombi were seen in any of our cases.
The diagnosis of MAC is difficult to render based entirely on pathologic grounds. The usual clinical setting is of a transplant patient who develops severe or non-transient diarrhoea meriting a colonoscopy and biopsy. The clinicopathologic differential diagnosis in these cases is broad, and includes infections (particularly CMV), mycophenolate toxicity, graft-versus-host disease (particularly in bone marrow allografts) and IBD. The difficulty in pathologic diagnosis is compounded by the overlapping morphologic features of mycophenolate colitis and the other diagnostic considerations.
Three cases in our series highlight the issue of dual pathology, and caution against dogmatism in diagnosing MAC. Two cases (cases 5 and 6) showed concomitant CMV infection with characteristic viral inclusions seen on H&E, and confirmed with immunohistochemistry. However, it was difficult to ascertain the relative contribution of this to the morphologic change and symptomatology. While CMV may be associated with increased crypt apoptosis and active stromal and crypt inflammation, architectural distortion and isolated crypt damage are usually not prominent features. Nevertheless, despite uncertain clinical significance, the incidence of CMV (25%) in our study suggests a possible role for routine CMV immunohistochemistry. The final case (case 7) with dual pathology involved a 32-year-old patient with persistent changes and symptoms 1 year after cessation of MMF, raising the possibility of de novo IBD. The development of IBD, post-organ transplant, is uncommon and may be masked, clinically, by immunosuppressive treatment.8 ,9 In the case of patients receiving MMF, the diagnostic difficulty is further compounded by the IBD-like changes seen on biopsies, and the requirement for continuing immunosuppression. As in our case, diagnosis of IBD in these patients may necessitate drug withdrawal to allow for possible MMF-related symptoms and biopsy changes to resolve.
In conclusion, MMF-associated colitis should be considered in every patient receiving MMF presenting with diarrhoea. Although a wide spectrum of changes may be seen, important microscopic clues to MAC include a mixed pattern of injury (typically a combination of crypt apoptosis, cryptitis, isolated crypt damage and architectural distortion), and the suggestion of proximal accentuation of pathologic changes. The observations in this small series merit further investigation with studies in larger cohorts. The need for clinical correlation and follow-up is emphasised by the possibility of dual pathology in patients treated with MMF.
What this study adds
-
This is, to our knowledge, the first paper which describes mucosal changes seen in mycophenolate mofetil (MMF)-associated colitis semiquantitatively. We describe two previously unreported diagnostically helpful findings, that is, MMF-associated colitis shows a mixed rather than pure injury pattern, and some microscopic changes are seen more in the proximal colon. In addition, three cases in our series illustrate the possibility of missing potentially treatable causes of colitis, and emphasise the importance of clinicopathologic correlation.
Take-home messages
-
Mycophenolate-associated colitis (MAC) should be considered in all patients receiving mycophenolate mofetil therapy presenting with diarrhoea, although diagnosis requires close clinicopathologic correlation.
-
Although no specific diagnostic biopsy changes are seen with MAC, the mixed pattern of injury characterised by features resembling inflammatory bowel disease (IBD), focal ‘ischaemic-type’ damage and focal cryptitis, and proximal accentuation of changes should raise the possibility.
-
Alternative aetiology of colitis (such as, CMV and IBD, as seen in the current study) need to be excluded before rendering a diagnosis of MAC, and considered if symptoms persist despite drug withdrawal.
Footnotes
-
Contributors SL: principal author, preparation of manuscript, review of slides; WBB: preparation of manuscript; MPK: senior author, conceived study, preparation of manuscript, review of slides; KS: provided cases, reviewed clinical details.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.