Article Text

Abstract
Aims: To evaluate whether ki-67 labelling index (LI) has independent prognostic value for survival of patients with bladder urothelial tumours graded according to the 2004 World Health Organisation classification.
Methods: Ki-67 LI was evaluated in 164 cases using the grid counting method. Non-invasive (stage Ta) tumours were: papilloma (n = 5), papillary urothelial neoplasia of low malignant potential (PUNLMP; n = 26), and low (LG; n = 34) or high grade (HG; n = 15) papillary urothelial carcinoma. Early invasive (stage T1) tumours were: LG (n = 58) and HG (n = 26) carcinoma. Statistical analysis included Fisher and χ2 tests, and mean comparisons by ANOVA and t test. Univariate and multivariate survival analyses were performed according to the Kaplan–Meier method with log rank test and Cox’s proportional hazard method.
Results: Mean ki-67 LI increased from papilloma to PUNLMP, LG, and HG in stage Ta (p<0.0001) and from LG to HG in stage T1 (p = 0.013) tumours. High tumour proliferation (>13%) was related to greater tumour size (p = 0.036), recurrence (p = 0.036), progression (p = 0.035), survival (p = 0.054), and high p53 accumulation (p = 0.015). Ki-67 LI and tumour size were independent predictors of disease free survival (DFS), but only ki-67 LI was related to progression free survival (PFS). Cancer specific overall survival (OS) was related to ki-67 LI, tumour size, and p27kip1 downregulation. Ki-67 LI was the main independent predictor of DFS (p = 0.0005), PFS (p = 0.0162), and cancer specific OS (p = 00195).
Conclusion: Tumour proliferation measured by Ki-67 LI is related to tumour recurrence, stage progression, and is an independent predictor of DFS, PFS, and cancer specific OS in TaT1 bladder urothelial cell carcinoma.
- DFS, disease free survival
- HG, high grade
- ISUP, International Society of Urological Pathologists
- LG, low grade
- LI, labelling index
- PFS, progression free survival
- PUNLMP, papillary urothelial neoplasia of low malignant potential
- OS, overall survival
- RR, relative risk
- WHO, World Health Organisation
- bladder cancer
- survival
- prognosis
- ki-67 MIB1
- grade
Statistics from Altmetric.com
- DFS, disease free survival
- HG, high grade
- ISUP, International Society of Urological Pathologists
- LG, low grade
- LI, labelling index
- PFS, progression free survival
- PUNLMP, papillary urothelial neoplasia of low malignant potential
- OS, overall survival
- RR, relative risk
- WHO, World Health Organisation
Most bladder urothelial tumours (80%) are non-invasive (stage Ta) but 20% invade the lamina propria/submucosa (stage T1) at diagnosis.1–5 Stage Ta tumours have a high risk of recurrence (50–75%) but a low risk of progression (5%), and stage T1 tumours have a high progression rate (30–50%).4,6 Conventional prognostic factors have a limited ability to predict behaviour in TaT1 bladder carcinoma, tumours for which more reliable indicators of aggressiveness (recurrence or progression) are needed.4,7,8 Tumour stage is still considered the most important predictor of patient outcome, but the significance of pathological grade is less consistent.4,5,9,10
“Tumour proliferation is thought to be a powerful prognostic indicator of tumour recurrence”
A new grading classification of bladder tumours based on the former 1998 ISUP/WHO (International Society of Urological Pathologists/World Health Organisation) grading system has recently been introduced by the WHO, followed by controversies on its predictive value.1,4,5 Since the introduction of this grading scheme a limited number of studies have investigated the issue of immunohistochemical markers in predicting the outcome of superficial bladder tumours.3,7,9–13 Recent studies have mainly investigated the use of p53 nuclear accumulation and the ki-67 MIB1 proliferation index. Tumour proliferation is thought to be a powerful prognostic indicator of tumour recurrence, and p53 accumulation is viewed as a marker of progression, although some studies failed to demonstrate independent prognostic significance.2,6,10,11,14–20 Patients with aberrant expression of ki-67 MIB1, p53, or p27Kip1 might have a better prognosis when coexisting with fibroblast growth factor receptor 3 (FGFR3) mutations.7,13
The purpose of our study was to investigate the predictive value of the ki-67 MIB1 labelling index (LI) in the prognosis of patients with primary TaT1 bladder urothelial cell carcinoma graded according to the 2004 WHO grading scheme in comparison with the immunohistochemical expression of relevant markers, such as p21 Waf1, p27Kip1, and p53. Patient’s age, patient’s sex, tumour size, multiplicity, and pathological stage also entered the analysis as clinicopathological variables.
MATERIAL AND METHODS
Our study group was a sequential cohort series of 164 patients with primary bladder tumours treated between 1990 and 1995 by complete transurethral resection of the bladder and random mucosal biopsies. Patients with high grade carcinoma also received intravesical BCG as current protocol. Patient’s follow up, calculated as the number of months from the date of the diagnostic surgical procedure to the date of the most recent cystoscopy (or the last visit or death), was five to 12 years (mean, 75; SD, 28). Tumour recurrence was defined as reappearance of tumour after the initial treatment with at least one tumour free cystoscopy interval. Tumour stage progression was defined as a shift to a higher stage—T1–T2–T4 in Ta tumours, stage T2–T4 in T1 tumours—or the appearance of metastasis. Survival time was the period between diagnosis and death. Cancer related death was that caused by bladder carcinoma. The end point of our study was disease free, progression free, and overall cancer specific survival. Tumour size was defined as the largest tumour measured with the resection loop, which is 1 cm long, and specimens were stratified as < 3 cm, 3–5 cm, and > 5 cm.
Haematoxylin and eosin stained slides including primary tumours and their recurrences were re-evaluated by three dedicated pathologists without knowledge of the clinical status. Briefly, the slides were first reviewed by a specialised genitourinary pathologist, followed by two additional pathologists with a special interest in uropathology. Fifty urothelial cell bladder carcinomas, published available information,1,4,5,21 and web facilities (http://162.129.103.34/bladder/) served as a preliminary teaching set to facilitate agreement on grading and staging parameters. Sections were graded in the worst differentiated area. If a discrepancy occurred in grading or staging a review round was organised to obtain a consensus diagnosis. The resulting grade and stage were in accordance with the 2004 WHO (former WHO/ISUP 1998) and the TNM 2002 revision.5,22
Quantitative and qualitative assessment of immunohistochemistry
A representative paraffin wax block from each tumour was serially cut at 4 μm thickness, dewaxed in xylene, rehydrated in graded ethanol, and washed for five minutes with phosphate buffer saline. For antigen retrieval, the sections were boiled in 10mM citrate buffer (pH 6.0). Endogenous peroxidase was blocked by incubation of the slides for 30 minutes with 3% hydrogen peroxide in methanol. Sections were then incubated with the primary mouse monoclonal antibodies (table 1) at room temperature, incorporating positive and negative controls. Immunohistochemical staining was performed using the highly sensitive polymer based EnVision system (DakoCytomation, Glostrup, Denmark). The reaction was visualised with diaminobenzidine as chromogen substrate solution (0.6 mg/ml in Tris buffer saline, pH 7.6 with 12 ml 30% hydrogen peroxide) for 30 minutes at room temperature. Sections were counterstained with Mayer’s haematoxylin, dehydrated, and mounted as standard procedure. Quantitative analysis was carried out using a Nikon Labophot optical microscope (Tokyo, Japan). Three dedicated pathologists independently evaluated all immunohistochemical slides in a blinded fashion. The same area on each slide was examined. A set of 50 urothelial cell carcinomas collected from a previous study12 served as a preliminary teaching set to facilitate agreement before the main study was carried out. If a discrepancy occurred between the assessments of the observers, the slides were reassessed in a combined session without the information of the previous scores. The presence and location of the TaT1 lesion was carefully controlled (“sandwich technique”: evaluation of a haematoxylin and eosin stained slide that was taken from the paraffin wax block before and after the slides for immunohistochemistry were cut) to ensure that the section for immunohistochemistry contained the same lesion.9 All markers were measured quantitatively using random fields measuring 62 500 μm2 delineated by a 1 cm2 graded ocular grid attached to the eyepiece of the microscope. The regions were chosen inside high immunoreactive areas and were examined under high power magnification (×400), counting a mean of 1000 cells/case. An LI expressed as the percentage of positive nuclei was established for each marker, which allowed tumours to be stratified according to the low versus high expression scheme used in previous studies: < 13% v > 13% for ki-67, < 10% v > 10% for p21 Waf1, < 30% v > 30% for p27Kip1, and < 6% v > 6% for p53.
Characteristics of immunohistochemical markers used in our present study
Statistical analysis
Bivariate and multivariate analyses were undertaken by means of Fisher’s exact test and χ2 analysis. The mean ki-67 MIB1 LI was assessed for differences using ANOVA for stage Ta tumours and the t test for stage T1 tumours. Univariate survival analysis was conducted using the Kaplan–Meier method and differences among groups were tested for significance using the log rank test. Significant parameters entered a multivariate analysis of probable prognostic factors for survival using Cox’s proportional hazard regression analysis and the relative risks (RRs) with 95% confidence intervals were calculated. The statistical analysis was performed using SPSS for Windows software (SPSS Inc, Chicago, Illinois, USA). A p value ⩽ 0.05 was considered to be significant. All tests were two sided.
RESULTS
The mean age at diagnosis of the 164 patients (21 women) was 61 years (range, 29–93). Eighty (48.78%) patients had non-invasive tumours classified as papilloma (6.25%), papillary urothelial neoplasia of low malignant potential (PUNLMP; 32.50%), low grade (LG; 42.50%), or high grade (HG; 18.75%) carcinomas. Fifty eight of the 84 stage T1 tumours were LG carcinoma. Tumour size ranged from 1 to 8 cm (mean, 3.08). As shown in table 2, high tumour proliferation correlated with larger tumour size, recurrence, stage progression, survival status (borderline significance), and p53 overexpression (fig 1). No association was seen with patient’s age or sex, multiplicity, grade, stage, or p21 Waf1/p27Kip1 downregulation. The mean ki-67 MIB1 LI increased progressively in stage Ta and T1 tumours (table 3; fig 2). None of five patients with urothelial papilloma (two of which recurred) progressed or died of disease.
Ki-67 MIB1 immunohistochemical expression and clinicopathological parameters in superficial (stage Ta or T1) bladder urothelial tumours
Mean Ki-67 MIB1 labelling index values according to the 2004 WHO categories in stage Ta and T1 bladder urothelial cell tumours
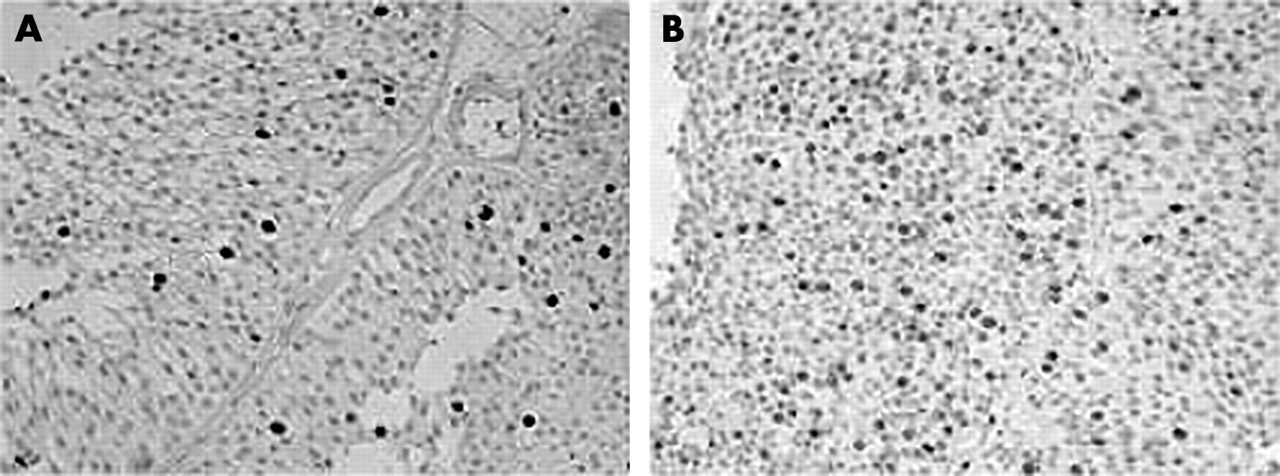
Examples of bladder urothelial carcinoma showing (A) low and (B) high ki-67 MIB1 labelling index. Streptavidin–biotin peroxidase immunohistochemistry; original magnification, ×100.

Box plots illustrating the mean ki-67 MIB1 labelling index in (A) stage Ta and (B) stage T1 bladder urothelial tumours stratified according to the 2004 World Health Organisation classification (see also table 3). HG, high grade; LG, low grade; LMP, papillary urothelial neoplasia of low malignant potential.
During follow up time, 81 (49.39%) patients remained free of disease; stage progression was seen in 28 (17.07%) patients and 23 (14.02%) patients died of disease. Univariate survival analysis showed that higher tumour grade in stage Ta tumours (log rank, 4.75; p = 0.0456), increased tumour size (log rank, 6.87; p = 0.0322), and high proliferation index (log rank, 8.85; p = 0.0029) were associated with shorter disease free survival (DFS). No association was found between tumour grade in stage T1, stage (Ta v T1), p21 Waf1, p27Kip1, or p53 expression and DFS. Tumour size (log rank, 7.34; p = 0.0254) and tumour proliferation (log rank, 5.67; p = 0.0172) were related to progression free survival (PFS), but tumour grade and stage and the expression of p21 Waf1, p27Kip1, and p53 were not related. Cancer specific overall survival (OS) was related to tumour size (log rank, 6.11; p = 0.003) and Ki-67 MIB1 LI (log rank, 5.23; p = 0.0222). p27Kip1 downregulation (log rank, 3.60; p = 0.0539) and tumour stage (log rank, 3.35; p = 0.0578) had borderline significance. Tumour grade and the expression of p21 Waf1 or p53 were not associated. Cox’s multivariate analysis selected ki-67 MIB1 LI (RR, 3.0293) and tumour size (RR, 2.5058); ki-67 MIB1 LI (RR, 3.3832); and ki-67 MIB1 LI (RR, 3.8154), tumour size (RR, 3.5138), and p27Kip1 downregulation (RR, 2.7178) as independent predictors of DFS, PFS, or OS, respectively. Ki-67 MIB1 LI was the main independent predictor of survival in the study groups (table 4; fig 3).
Cox multivariate analysis showing significant variables independently related to disease free, progression free, and cancer specific overall survival in 164 patients with stage Ta or T1 bladder urothelial tumours

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plots illustrating the association between clinical and immunohistochemical parameters with disease free, progression free, and overall survival. These markers were selected as independent predictors in the multivariate analysis.
DISCUSSION
Only a few studies have investigated the issue of immunohistochemical markers in predicting the outcome of TaT1 bladder urothelial cell carcinoma since the introduction of the WHO/ISUP grading scheme for bladder urothelial tumours (now recognised as the 2004 WHO classification).9,10,14 Recent studies have focused mainly on p53 and ki-67 MIB1 LI, and have suggested that they might be related to progression and recurrence, respectively2; however, studies including survival analysis are limited. In addition, short term follow up, low numbers of cases, and variable stage selection characterise most previous reports. Therefore, the prognostic role of these markers in TaT1 bladder tumours needs to be substantiated. Moreover, a multivariate survival analysis of tumour proliferation compared with prognostically relevant cell cycle related proteins and conventional clinicopathological parameters, as performed here, would provide superior clinically useful information.
“The ki-67 MIB1 labelling index was an independent predictor of disease free, progression free, and overall survival in TaT1 bladder urothelial cell carcinoma”
In our study, large tumour size, high grade in stage Ta tumours, and high ki-67 MIB1 LI were predictors of short DFS in univariate analysis, but only ki-67 MIB1 LI and tumour size were independent predictors in multivariate analysis (with ki-67 MIB1 as the main predictor). These results agree with those of Oosterhuis et al who, in a similar study including stage Ta/T1 cases, reported that high ki-67 MIB1 LI was an independent predictor of significantly shorter DFS.18 These authors included a similar cut off point to the one used in our study to define proliferation (< 13% v > 13%); this was also associated with DFS in the study of Dybowski et al, although these authors used a different grading system.14 They found superior predictive value of DFS when proliferation and p27Kip1 downregulation were combined. Pich et al found that the ki-67 MIB1 LI was the best predictor of recurrence in non-invasive bladder tumours (PUNLMP and LG carcinoma).6 Yan et al suggested that the ki-67 MIB1 LI could be used to identify higher risk of a first recurrence.23 Van Rhijn et al found that a high proliferation was related to poor survival, but in their cases FGFR3 mutation was a protective factor.7 In the study of Zlotta et al, p21 Waf1, p53, and ki-67 MIB1 LI did not predict response to BCG treatment.24 Our study suggests additional prognostic value for tumour size and the 2004 WHO grading scheme of non-invasive tumours; DFS was longer in patients with PUNLMP or LG bladder carcinoma whose tumours were less than 3 cm or had a low proliferation rate, a previously unreported finding in superficial bladder tumours. Other cell cycle related proteins such as p21 Waf1, p27Kip1, and p53 were not associated with DFS, unlike other reports, which found p27Kip1 or p21 Waf1 downregulation and high p53 accumulation more common in HG muscle invasive bladder carcinomas with low OS.14,16,20,23,25–32 Our study also investigated the role of ki-67 MIB1 LI, p53, p21 Waf1, p27Kip1, and clinicopathological parameters as markers of PFS and we found ki-67 MIB1 LI to be the only independent predictor—a finding previously unrecognised—which suggests that high tumour proliferation may increase the value of the WHO grading system as a predictor of stage progression. Bol et al suggested that the percentage area of ki-67 MIB1 by image analysis might be superior to ki-67 MIB1 LI alone in predicting PFS.9 Liukkonen et al and Oosterhuis et al, using different grade and stage selection, reported that the ki-67 MIB1 LI was related to PFS, but was not an independent predictor, perhaps because of the grade and stage selection of their patients.16,18 Finally, we found large tumour size, high tumour proliferation, stage, and p27Kip1 (the last two of borderline significance) to be markers of shorter OS in univariate analysis. High proliferation, tumour size greater than 5 cm, and downregulation of the cyclin dependent kinase inhibitor p27Kip1 were independent predictors of OS in our series, suggesting that alterations of p21 Waf1 and p53 are less relevant in TaT1 bladder tumours as predictors of OS.12 In our study, the fact that the pathological stage was not a significant predictor of DFS, PFS, and OS might be the result of the sampling procedure or the limited follow up. Similar results concerning staging have been reported by others in clinically and pathologically oriented studies.9,12,21,31,33–35 Although it is well known that the factors governing OS are multifactorial, it has been suggested that cyclin D3 overexpression might be superior to ki-67 MIB1 LI in predicting OS.12
Take home messages
-
Tumour proliferation measured by the ki-67 MIB1 labelling index (LI) is related to tumour recurrence and stage progression in bladder urothelial cell carcinoma
-
Ki-67 MIB1 LI is also an independent predictor of disease free, progression free, and cancer specific overall survival in TaT1 bladder urothelial cell carcinoma
-
Thus, ki-67 MIB1 LI might be useful for stratifying patients with TaT1 bladder tumours into risk categories
In conclusion, our study has shown that the ki-67 MIB1 LI is associated with recurrence and stage progression in bladder urothelial cell carcinoma but, most importantly, as shown by multivariate analysis, is an independent predictor of DFS, PFS, and OS in TaT1 bladder urothelial cell carcinoma. Thus, together with tumour size, ki-67 MIB1 LI might be useful for stratifying patients with TaT1 bladder tumours into risk categories; if confirmed by prospective studies, these results may have important clinical implications. The availability of ki-67 MIB1 antibodies in most pathology laboratories makes it an ideal marker to be used in the daily evaluation of bladder urothelial tumours.
Acknowledgments
Supported by the grants 00/898 and 03/952 (FIS (Ministry of Health), Madrid, Spain).