Article Text

Abstract
Backgrounds—Hepatic fibrosis is one of the main consequences of liver disease. Both fibrosis and steatosis may be seen in some patients with chronic hepatitis C and alcoholic liver disease (ALD).
Aims—To quantitate fibrosis and steatosis by stereological and morphometric techniques in patients with chronic hepatitis C and compare the results with a control group of patients with ALD. In addition, to correlate the quantitative features of fibrosis with the Ishak modified histological score.
Materials and methods—Needle liver biopsies from 86 patients with chronic hepatitis C and from 32 patients with alcoholic liver disease (disease controls) were analysed by stereological and morphometric analyses using the Prodit 5.2 system. Haematoxylin and eosin and Picro-Mallory stained sections were used. The area fractions (AA) of fibrosis, steatosis, parenchyma, and other structures (bile duct and central vein areas) were assessed by stereological method. The mean diameters of fat globules were determined by morphometric analysis.
Results—Significant differences were found in the AA of fibrosis, including fibrosis within portal tract areas, between chronic hepatitis C patients and those with ALD (mean (SD): 19.14 (10.59) v 15.97 (12.51)). Portal and periportal (zone 1) fibrosis was significantly higher (p = 0.00004) in patients with chronic hepatitis C compared with the control group (mean (SD): 9.04 (6.37) v 3.59 (3.16)). Pericentral fibrosis (zone 3) occurred in both groups but was significantly more pronounced in patients with ALD. These results correlate well with the modified Ishak scoring system. However, in patients with cirrhosis (stage 6) with chronic hepatitis C the AA of fibrosis varied between 20% and 74%. The diameter of fat globules was significantly lower in patients with hepatitis C (p = 0.00002) than the ALD group (mean (SD): 14.44 (3.45) v 18.4 (3.32)). Microglobules were more frequent in patients with chronic hepatitis C than in patients with ALD. In patients with chronic hepatitis C, the fat globules had a zonal distribution in comparison with pan steatosis in ALD.
Conclusion—Quantitative, stereological techniques are simple and reliable for evaluating hepatic fibrosis and steatosis in chronic hepatitis C. They are most useful for assessing the origin, location, and the stage of fibrosis. Stereology and morphometry are recommended for the quantitation of fibrosis and steatosis, particularly for the evaluation of new treatment strategies in patients with chronic hepatitis C.
- alcoholic liver disease
- hepatic fibrosis
- hepatitis C
- morphometry
- steatosis
- stereology
Statistics from Altmetric.com
Acute hepatitis C develops into chronic hepatitis in more than 50% of patients.1, 2 A proportion of patients with chronic hepatitis C progress to cirrhosis and hepatocellular carcinoma.3 Hepatic fibrosis is one of the most important features of chronic hepatitis C. The accurate assessment of hepatic fibrosis is important to study the natural history and the prognosis of patients with chronic hepatitis C. Fibrosis is also seen in patients with alcoholic liver disease (ALD)4–6 and other forms of non-alcoholic fatty liver disease (NAFLD).7–9 Steatosis is another morphological feature that can be seen in patients with chronic hepatitis C,10–13 ALD,5, 6 and NAFLD.7, 8, 14 There are several methods for assessing hepatic fibrosis and the progression of fibrogenesis in clinical practice. Chemical methods are used to measure the concentration of collagen in liver tissue.15–17 This is a good method but requires a large sample of liver tissue. Conventional routine histological examination is the most common method, although it is subjective and not quantitative. A histological semiquantitative scoring system for the evaluation of hepatic fibrosis has been described.18–20 Morphometric assessment of hepatic fibrosis has been considered the gold standard technique,21 and has been used to assess hepatic fibrosis in experimental animals22, 23 and in clinical practice.2, 18, 24 Fat in liver disease has been assessed by semiquantitative methods,14 by automated computerised procedures,25, 26 and biochemically in liver biopsy specimens.27
Therefore, the accurate assessment of the quantity of fibrosis and steatosis is important for the pathological, clinical, and prognostic evaluation of patients with chronic hepatitis C.
In our present study, we have chosen to focus our attention on patients with chronic hepatitis C versus ALD as a disease control group and have concentrated on the quantification of hepatic fibrosis and steatosis by stereological and morphometric techniques. We also compared the quantitative values of fibrosis with the Ishak modified scoring system.19
Materials and methods
One hundred and eighteen liver biopsy specimens were evaluated from patients with chronic hepatitis C (64 UAE, 22 UK) and ALD (32 patients, UK) as disease controls. The mean age of the patients with chronic hepatitis C was 39.5 years (range, 18–65) and 60 were men. The mean age of patients with ALD was 49.8 years (range, 30–69) and 22 were men. In addition to clinical manifestations, all patients with hepatitis C had positive serological and immunological tests for hepatitis C (second generation tests). None of these patients had a history of alcohol intake. All patients with alcoholic liver disease had a long history of alcohol intake with clinical and biochemical evidence of chronic liver disease. None of the patients with chronic hepatitis C had received antiviral treatment before the biopsy procedure. Liver biopsy specimens were fixed in 4% buffered formal saline and embedded in paraffin wax. Sections were cut at 5 μm thickness and were stained with haematoxylin and eosin (H&E), reticulin, the Picro-Mallory stain, and other special stains. The H&E stain was used at two levels. All liver biopsies from patients with chronic hepatitis C were also assessed in relation to the Ishak modified score.19 The score of fibrosis was recorded as follows: 0, no fibrosis; 1, fibrous expansion of some portal tract areas; 2, fibrous expansion of most portal tract areas; 3, fibrous expansion of portal tract areas with occasional portal–portal bridging; 4, fibrosis with portal–portal and portal–central bridging; 5, pronounced bridging with occasional nodules; and 6, probable or definite cirrhosis.
Steatosis was assessed in H&E stained sections by morphometric analysis.
STEREOLOGY
Stereology (area fraction; AA) is used to obtain quantitative information about the volume, area, length, and numerical density in three dimensional structures using a simple point counting technique or a computer program. In chronic hepatitis C and ALD, the changes are usually uniform throughout the liver; therefore, biopsy sampling can be considered unbiased for assessing the area fraction. The AA of steatosis, unchanged parenchyma, portal tract, central veins, and fibrosis in all zones were assessed by stereological analysis using an objective magnification of ×10 (Nikon microscope). Stereological assessment was carried out using a computerised image analysis system (Prodit 5.2; BMA, Amsterdam, the Netherlands). A monitor screen with parallel Weibel overlay grid with 72 points at a distance of 31.83 μm was used to count fat globules, unchanged parenchyma, portal tract areas, central veins, and fibrosis (Picro-Mallory stain). At least 1000 points covering the above features were counted in each liver biopsy specimen and the whole biopsy area was covered at one level of sectioning. At least 13 fields were selected for measurement to include all zones, portal tracts, and vein areas.
MORPHOMETRY
Morphometry is the measurement of forms and it is used in histopathology to describe measurements made from two dimensional sections. We used morphometry to assess the area and diameter of fat globules in biopsies with steatosis in H&E stained sections.
Steatosis was assessed in two areas: the pericentral area (zone III) and the periportal area (zone I). A special computer program was used to assess the area of parenchyma that contained steatosis. This computer program allowed the measurement to be done in two phases. At least 10 fields were chosen for morphometric analysis around portal tract areas, central vein areas, or nodules in cirrhotic livers. The mean diameter of fat globules was obtained (all measurements are in micrometers).
DEFINITIONS
Fat globules were graded quantitatively as follows.
-
Microvesicular steatosis (microglobules): the mean diameter of fat globules plus one standard deviation is less than 15 μm (M + SD < 15 μm).
-
Macrovesicular steatosis (macroglobules): the mean diameter of fat globules minus one SD is equal to or larger than 15 μm (M − SD ≥ 15 μm).
-
Mixed macrovesicular and microvesicular steatosis: the mean diameter of fat globules plus or minus one SD is more or less than 15 μm (M + SD > 15 μm or M − SD < 15 μm).
Parenchyma is defined by the area occupied by hepatocytes, Kupffer cells, and sinusoids without fatty changes.
Pleomorphism of fat globules is the degree of variation in the size of fat globules. This was obtained from the SD of the mean values of fat globules.
The distribution of fat globules was defined as periportal or pericentral when globules are confined to zone 3 or zone 1, respectively. Pan steatosis was defined as steatosis involving all zones or all nodules. Other forms of distribution of steatosis were defined by the presence of steatosis in part of the cirrhotic nodules or both pericentral and periportal liver cell parenchyma.
STATISTICAL ANALYSIS
Data were analysed using a software program EP1 INFO Version 6. The ANOVA test was used to derive the p value for normally distributed data. When Bartlett's test showed the variances in the samples to differ, the non-parametric Kruskal-Wallis H (equivalent to χ2) was used to obtain the p value. Significance was set at p < 0.05 (two tailed).
The intraobserver reproducibility for assessing fibrosis and steatosis by stereological and morphometric techniques was tested. The coefficient of variation (CV) of fibrosis was 1.6% and the CV of steatosis was 3.8%. Reproducibility is equal to 100 − CV. The stereological and morphometric analyses were undertaken by a single observer (AMZ).
Results
MORPHOLOGICAL CHANGES
Figure 1 shows the patterns of distribution of fat globules in patients with chronic hepatitis C and ALD. Pan steatosis was higher in ALD than in chronic hepatitis C. Periportal and other forms of distribution of fat were seen more frequently in patients with chronic hepatitis C than in those with ALD.
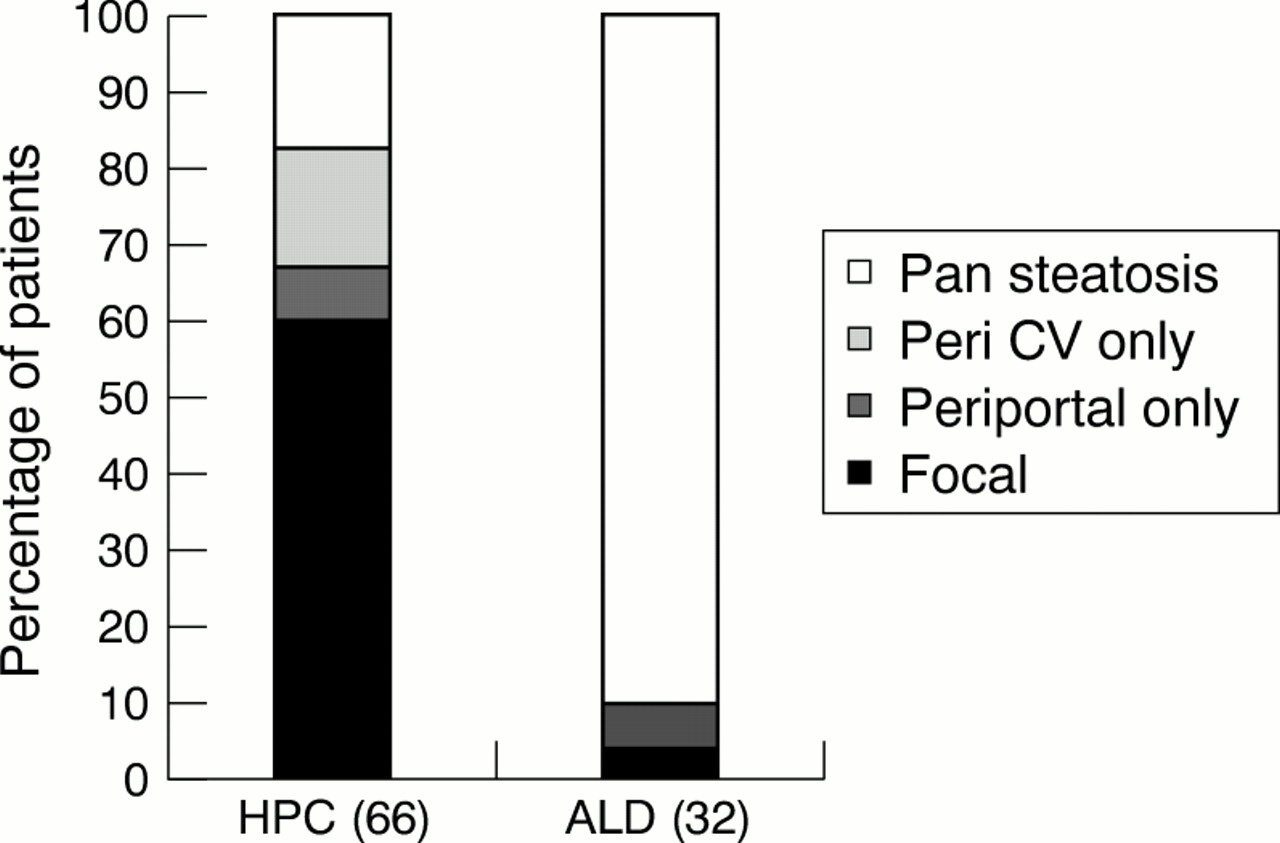
The patterns of distribution of fat globules in patients with chronic hepatitis C (HPC) and alcoholic liver disease (ALD). CV, central vein.
STEREOLOGICAL CHANGES
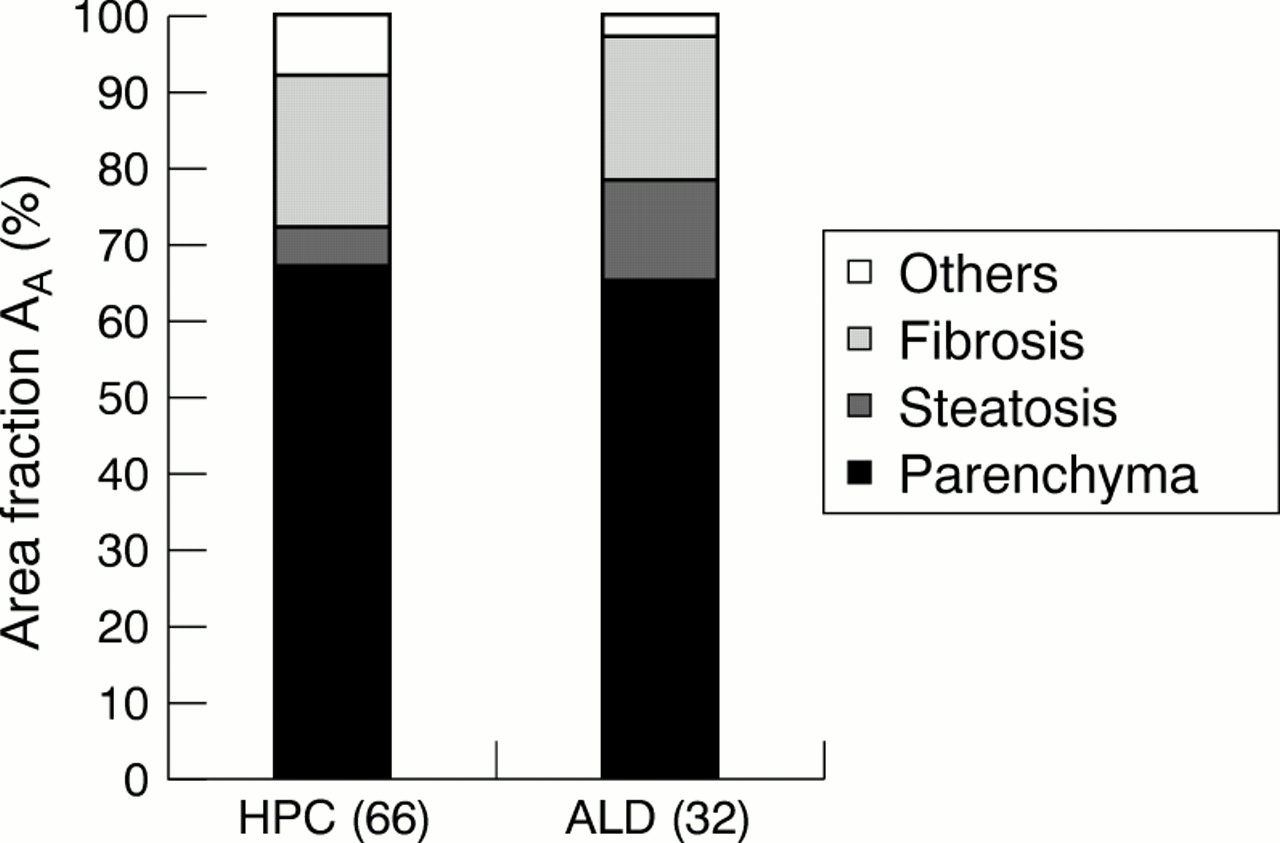
Figure 2 shows the AA values of fibrosis, steatosis, parenchyma, and other structures (portal tract areas, central vein areas combined) in patients with chronic hepatitis C and ALD. There was a significant difference (p = 0.008) in the AA of fibrosis between the two groups. The AA of steatosis was significantly higher in patients with ALD than in those with hepatitis C (p = 0.0002). There was no significant difference in the AA of parenchyma between the two groups. Figure 3 shows the stereological findings of fibrosis in patients with chronic hepatitis C in relation to the Ishak modified score of fibrosis. The area fraction of fibrosis increased exponentially from score 1 (portal fibrosis) to precirrhosis (score 5) to complete cirrhosis (score 6). In patients with cirrhosis the total percentage of fibrosis varied between 20% and 74% (approximately fourfold). Table 1 shows the percentage value of fibrosis in all topographical locations in chronic hepatitis C and ALD. In chronic hepatitis C, periportal fibrosis was significantly higher than in the ALD group (p = 0.00004). In ALD, pericentral fibrosis was significantly higher than in patients with chronic hepatitis C (p = 0.0045).
The area fraction of fibrosis in relation to topography in liver biopsies from patients with chronic hepatitis C (HPC) and chronic liver disease (ALD)

The area fraction values of fibrosis, steatosis, and other normal structures in patients with chronic hepatitis C (HPC) and alcoholic liver disease (ALD).

The area fraction of total fibrosis, including fibrosis in the portal tract area, in 86 patients with chronic hepatitis C in relation to the Ishak modified score.
MORPHOMETRIC CHANGES
Table 2 shows the mean diameter of fat globules in patients with chronic hepatitis C and ALD. The diameter of fat globules was significantly higher in patients with ALD than in those with chronic hepatitis C (p = 0.00002). Pleomorphism of fat globules was significantly higher in patients with ALD than in those with chronic hepatitis C (p = 0.009).
Morphometric features of fat globules in patients with hepatitis C (HPC) and alcoholic liver disease (ALD)
Figure 4 shows the grades of fat globules in chronic hepatitis C and ALD. The proportion of macroglobules was higher in patients with ALD than in those with chronic hepatitis C (p = 0.0003). The proportion of microglobules was higher in chronic hepatitis C than in ALD (p = 0. 0003).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The grades of fat globules in chronic hepatitis C (HPC) and alcoholic liver disease (ALD).
Discussion
The primary aim of our study was to assess fibrosis and steatosis by quantitative methods in liver biopsy specimens from patients with chronic hepatitis C. Quantification of fibrosis by image analysis has been considered to be the gold standard of morphological measurement because its CV is very low,4, 18 and values have been shown to correlate well with chemical α2 macroglobulin determination.16 Some authors have used morphometric techniques to assess fibrosis in patients with chronic hepatitis C.28, 29 We have shown in a previous study24 that stereology is superior to morphometry for quantifying fibrosis in ALD and NAFLD. In our current study, we have used stereology to assess fibrosis in patients with chronic hepatitis C. Stereological analysis has shown a significant increase in the area fraction with the increase in severity of chronic liver disease.
The modified Ishak scoring system19 has been used by pathologists as a semiquantitative estimation of fibrosis. Other systems have also been introduced to assess fibrosis.18, 30 However, these systems remain subjective. In addition, it may be difficult to compare the results between different studies using different scoring systems. The potential interobserver and intraobserver variation of grading and staging of fibrosis is very high. Our stereological technique for assessing fibrosis has shown a linear increase in the mean value of fibrosis in comparison with the modified Ishak score. However, there was an approximately fourfold variation (20–74%) in the proportion of fibrosis within the same group of patients with established cirrhosis (score 6). A recent study has shown a similar fivefold difference within the same group of Knodell's score.30 This throws doubt on the validity of semiquantitative staging19 in the evaluation of new treatment strategies in hepatic fibrosis. Paradis et al have shown that necro inflammatory lesions and collagen content are important features for predicting the progression of liver disease in patients with chronic hepatitis C.31 Other authors have shown that serum collagen and fibrosis may lead to resistance to treatment with interferon in patients with chronic hepatitis C.32–34
The second goal of our work was to compare the degree of fibrosis at different locations in the patients with chronic hepatitis C and those with ALD. We found significant differences in the amount of fibrosis in relation to topography (in all locations) in patients with chronic hepatitis C and ALD. Periportal fibrosis was significantly higher in patients with chronic hepatitis C, whereas fibrosis was significantly higher in pericellular and pericentral vein areas in ALD. Several studies4, 14, 15 have shown that pericentral fibrosis lesions in ALD are the first apparent lesions in the sequence of events leading to alcoholic cirrhosis. The assessment of fibrosis in individual locations and the total areas yield a useful clue to the origin of fibrosis in both chronic hepatitis C and alcoholic disease. The significant difference in the location of fibrosis indicates that the origin of fibrosis differs between chronic hepatitis and ALD. It seems that the origin of fibrosis is predominantly pericentral and pericellular in ALD and predominantly periportal in chronic hepatitis C. Some authors have shown that pericentral fibrosis is a precursor lesion of cirrhosis.35, 36 The natural history of liver fibrosis progression in patients with chronic hepatitis C has been studied.37 It has been estimated that, without treatment, 33% of patients have an expected median time to cirrhosis of less than 20 years.37
Steatosis of the liver is not a disease entity but a histological feature that may have clinical associations. It is the most common morphological feature seen in patients with ALD and some patients with chronic hepatitis C. We described a quantitative method to assess steatosis in all histopathological stages of liver disease in both groups of patients. Semigrading of steatosis has been described by many authors.7, 14, 38 Semiquantitative and fully automated methods have also been described,38 but require special staining for fat. In semiautomated interactive methods, H&E stained sections prepared for routine diagnosis can be used. In a previous study26 we assessed steatosis by two quantitative methods. Other authors have also used quantitative techniques to assess steatosis in liver biopsies.39 In our present study, both stereology and morphometry were used for assessing steatosis. Stereology has shown significant variation in AA of steatosis between patients with chronic hepatitis C and those with ALD. The diameter of fat globules differed significantly between the two groups. The highest degree of variation in the diameter of fat globules was seen in patients with ALD. In humans, fat globules initially formed in zone 3 coalesce to form large droplets. This may explain the variation in the diameter of fat globules in patients with ALD. Our results confirm the morphological findings that steatosis is focally distributed and is seen more frequently in zone 1 in patients with chronic hepatitis C than in those with ALD.
In a previous study,26 we found a good correlation between the morphological grading of fat globules and morphometric grades. Our present study has shown another application of the quantitative grades in patients with chronic hepatitis C. This system can be used easily to study the changes in steatosis when evaluating a new treatment strategy and also for follow up of patients with chronic hepatitis C.
In conclusion, stereology and morphometry are simple and reliable quantitative techniques for the measurement of fibrosis and steatosis in patients with chronic hepatitis C. Stereology offers a means of assessing fibrosis and steatosis in the entire biopsy specimen, whereas morphometry is very useful in assessing steatosis in relation to the size and diameter of fat globules. In view of the high reproducibility in intrafield assessment and low intraobserver variability, we recommend this method as one of the most important tools in the evaluation of new treatment strategies in hepatic fibrosis and for follow up of patients with chronic hepatitis C and ALD.