Article Text

Front line tests for the investigation of suspected porphyria
Abstract
The porphyrias are uncommon disorders of haem biosynthesis and their effective management requires prompt and accurate diagnosis. This article describes methods for the determination of urinary porphobilinogen, urinary and faecal total porphyrins, and total porphyrins in erythrocytes and plasma that are suitable for use in non-specialist laboratories. The selection and interpretation of these methods, and the indications for further, more specialised, investigation are discussed.
- porphyria
- haem biosynthesis
- best practice guidelines
Statistics from Altmetric.com
Front line tests for the investigation of suspected porphyria
Although the porphyrias are uncommon disorders of haem biosynthesis, the wide range and variability of their clinical features leads to their inclusion in the differential diagnosis of many diseases. Therefore, every acute hospital laboratory needs to have simple, reliable methods for their exclusion and for the identification of those few patients who need more specialised further investigation. Here, we describe methods that are suitable for the initial investigation of patients suspected of having porphyria. Accurate identification of the type of porphyria normally requires more sophisticated methods of analysis. These further investigations, family studies, and the investigation of asymptomatic patients with a past history of porphyria are best entrusted to specialised laboratories with expertise in the porphyrias.1, 2
The clinical features and inheritance of the main types of porphyria have been reviewed3, 4 and are summarised in table 1. Each type results from partial deficiency of one of the enzymes of haem biosynthesis (fig 1). Accumulation of the substrate of the defective enzyme produces a pattern of accumulation and excess excretion of haem precursors and their derivatives that characterises each disorder (table 2).3 Symptoms that are caused by porphyria are always accompanied by detectable overproduction of haem precursors. Conversely, the absence of evidence for overproduction indicates that any concurrent symptoms are very unlikely to be the result of porphyria. Metabolite concentrations may be normal during remission and in all children and many adults who have inherited an acute porphyria but have never had symptoms (latent porphyria). In these circumstances, enzymatic or DNA analyses are required.7
The main types of porphyria
The porphyrias: patterns of overproduction of haem precursors

Haem biosynthetic pathway showing the sites of enzyme deficiencies in the porphyrias. Enzymes: 1, 5-aminolevulinate (ALA) synthase; 2, ALA dehydratase (porphobilinogen synthase); 3, hydroxymethylbilane synthase (porphobilinogen deaminase); 4, uroporphyrinogen III synthase; 5, uroporphyrinogen decarboxylase; 6, coproporphyrinogen oxidase; 7, protoporphyrinogen oxidase; 8, ferrochelatase.
Selection of front line investigations
ACUTE PORPHYRIA
Acute neurovisceral attacks of porphyria are accompanied by excessive urinary excretion of porphobilinogen (PBG) and, to a lesser extent, 5-aminolevulinate (ALA), except in the exceedingly rare condition, ALA dehydratase deficiency, where PBG excretion is normal (table 2).8, 9 Therefore, the examination of urine for excess PBG is the key investigation in patients with suspected acute porphyria (table 2). Measurement of urinary total porphyrin by itself is unhelpful and may be misleading. Concentrations are usually increased when PBG is present in excess, owing to in vitro polymerisation of PBG to uroporphyrin, but increases also occur in hepatobiliary disease, alcohol abuse, and other common disorders.2
CUTANEOUS PORPHYRIA
The skin lesions of the cutaneous porphyrias are caused by photosensitisation of the skin by porphyrins and are always accompanied by evidence of overproduction of porphyrins. Patients with erythropoietic protoporphyria (EPP) usually present in childhood with acute photosensitivity unaccompanied by fragile skin or bullae. All other cutaneous porphyrias (bullous porphyrias) present with skin fragility, bullae, and other lesions in areas of skin exposed to the sun.3
A suspected diagnosis of EPP can be confirmed or excluded by measurement of erythrocyte free protoporphyrin, as long as a method is used that distinguishes free protoporphyrin from zinc–protoporphyrin.
For suspected bullous porphyria, examination of urine and either faeces or plasma for excess porphyrins is required. Plasma porphyrin analysis is an adequate substitute for faecal porphyrin measurement as a front line test, and is particularly useful for distinguishing variegate porphyria (VP) from other bullous porphyrias, of which porphyria cutanea tarda (PCT) is by far the most common.
Specimen collection and stability
All samples must be protected from light; urinary porphyrin concentrations can decrease by up to 50% if kept in the light for 24 hours. Urinary PBG and porphyrins are best analysed in a fresh, random sample (10–20 ml) collected without preservative. Twenty four hour collections offer little advantage, delay diagnosis, and increase the risk of losses during the collection period. PBG and porphyrins are stable in urine in the dark at 4°C for up to 48 hours and for at least a month at −20°C. Very dilute urine (creatinine < 4 mmol/litre) is unsuitable for analysis. About 5–10 g wet weight of faeces is adequate for the measurement of porphyrin concentrations. Diagnostically relevant changes in concentration are unlikely to occur within 36 hours at room temperature and samples are stable for many months at −20°C. Blood, anticoagulated with EDTA, shows no loss of protoporphyrin for up to eight days at room temperature and for at least eight weeks at 4°C in the dark.
Table 3 lists the samples required for the diagnosis of clinically overt porphyria and reference ranges are shown in table 4. It is good practice to treat all samples received from patients with suspected bullous porphyria as “high risk” because there is an increased frequency of infection with hepatotropic viruses, particularly hepatitis C, in PCT.
Essential front line investigations for patients with symptoms of porphyria
Adult reference ranges
Recommended methods
PORPHOBILINOGEN IN URINE
PBG reacts with Ehrlich's aldehyde reagent, 4-dimethylaminobenzaldehyde (DAMB) in acid, to give a red condensation product with a characteristic absorption spectrum that has a peak at 553 nm and a shoulder at approximately 540 nm. Other substances in urine either react with this reagent to give red products, notably urobilinogen, or inhibit the reaction. All need to be removed. This is best achieved by anion exchange chromatography but methods for accurate quantification of PBG based on this procedure are time consuming. Qualitative screening tests in which the PBG–Ehrlich compound is separated from the urobilinogen–Ehrlich complex by solvent extraction are rapid but have been criticised for low sensitivity and poor specificity.11, 12 A commercial semiquantitave kit (Trace PBG kit; Alpha Laboratories, Eastleigh, Hampshire, UK) provides a reasonably rapid, ion exchange resin based method that appears to be more sensitive and specific for initial screening than qualitative, solvent extraction procedures.13
Measurement of PBG in urine
A commercial kit based on the procedure described by Mauzerall and Granick for quantitative determination of PBG14 is available from BioRad Laboratories (Hemel Hempstead, Hertfordshire, UK). It contains mini columns of Dowex 2 resin and a preweighed vial of DMAB. Materials that are required but are not supplied with the kit are glacial acetic acid and perchloric acid (70%). Additional DMAB (BioRad) is also required if the same kit is to be used more than once because Ehrlich's reagent must be freshly prepared. The kit should be used exactly as described by the manufacturer.
Qualitative screening test for PBG
Mix urine (1.0 ml) with qualitative Ehrlich's reagent (1.0 ml) (2.8 g DMAB/litre of 7M HCl) in a glass test tube, allow to stand for two minutes, add saturated sodium acetate (2.0 ml), mix, add amyl alcohol (1.0 ml), vortex mix, and allow phases to separate. Inspect lower aqueous phase for pink/red colour. If colour is present, remove upper organic layer and re-extract aqueous phase with 1 ml aliquots of amyl alcohol until the upper organic layer is colourless. If any pink/red colour persists in the lower aqueous phase when the upper phase is colourless, the test is positive. For all positive tests, repeat the procedure but substitute 7M HCl for Ehrlich's reagent to detect false positives caused by indicator dyes derived from foods, soft drinks, medicines, etc. A normal urine sample and a quality control sample containing excess PBG should be included in every batch.
Quality control
No commercial quality control material is available. A suitable control can be prepared by dissolving a known amount of PBG (Sigma, Poole, Dorset, UK) in normal urine. An added amount of approximately 20 mg/litre (88 μmol/litre) is suitable for the quantitative and qualitative procedures described above. Before adding PBG, urine should be centrifuged, gentamycin sulphate added (2 ml of a 40 mg/ml solution) and the pH adjusted to 7–7.5. Control material prepared in this way and stored in aliquots at −20°C is stable for up to one year.
Comments
All positive screening tests, including those obtained with semiquantitative methods that use ion exchange resins, must be confirmed by a specific, quantitative method, preferably using the same sample of urine. The BioRad column method is suitable for this purpose. Very occasionally, other compounds may coelute with PBG and react with Ehrlich's reagent to give a similar colour. Therefore, for all samples with an increased PBG concentration, the identity of the PBG–Ehrlich compound should be confirmed by comparing its absorption spectrum with that given by the quality control material.
Quantitative Ehrlich's reagent contains perchloric acid to enhance its sensitivity but is unstable and must be prepared fresh each day. DMAB in HCl is stable for up to one month if stored in a dark glass bottle at room temperature.
Interpretation
The detection limits for PBG in urine for the Trace kit method and the qualitative test described above are 25 μmol/litre and approximately 50 μmol/litre, respectively. Most patients with an acute attack of porphyria excrete much greater amounts of PBG and their urine should give a positive screening test. PBG excretion decreases as the attack resolves but usually remains increased for many weeks in acute intermittent porphyria (AIP). However, in VP and hereditary coproporphyria (HCP), excretion may return to normal or near normal within a week or so after the onset of symptoms. If screening tests are negative and clinical suspicion of acute porphyria remains, it is essential to determine urinary PBG and ALA by a quantitative method and to analyse porphyrins in plasma and, if plasma fluorescence scanning excludes VP, faeces. If all these investigations are normal, acute porphyria is excluded as the cause of the symptoms.
PBG excretion may remain high during remission in AIP and can even be increased substantially in affected adults who have never had an acute attack. In these individuals, PBG increases still further during an acute attack but, in practice, this change is often difficult to detect and attribution of symptoms to acute porphyria in such circumstances requires careful clinical assessment. However, a normal PBG concentration excludes porphyria as the cause of symptoms in an individual with AIP. Because of their lack of sensitivity, qualitative and semiquantitive PBG methods should never be used for family studies or for the reinvestigation of patients with a past diagnosis of porphyria. A normal urinary PBG concentration does not exclude latent AIP because excretion is normal in virtually all children and many adults with latent disease.
TOTAL PORPHYRIN IN URINE
Porphyrins are highly conjugated macrocycles with characteristic electronic absorption spectra that have an intense absorbance peak around 400 nm (the Soret band). Acidification of urine intensifies absorbance, facilitates conversion of porphyrinogens to porphyrins, and dissociates zinc–porphyrin chelates. Thus, total porphyrin can be detected in acidified urine by spectrophotometry and estimated semiquantitatively, as long as a correction is made for background absorbance.15
Semiquantitative determination of total porphyrin
Urine is mixed to resuspend any sedimented material and an aliquot (4.0 ml) is mixed with 1.0 ml concentrated HCl (analar grade). Undissolved material is then removed by centrifugation before transferring the clear supernatant to a 1 cm cuvette and recording the absorption spectrum between 350 nm and 450 nm against air in the reference cuvette.
If a peak is present in the 400 nm region, the total porphyrin concentration is:  where A is the peak absorbance above a baseline drawn between two suitable points (fig 2) and the factor (2500) is derived from the volume of urine, the volume of acid, and a millimolar extinction coefficient of 500, which is approximately that of a 7/1 (mol/mol) mixture of coproporphyrin and uroporphyrin in 2.3M HCl. The porphyrin composition of this mixture resembles that of normal urine.
where A is the peak absorbance above a baseline drawn between two suitable points (fig 2) and the factor (2500) is derived from the volume of urine, the volume of acid, and a millimolar extinction coefficient of 500, which is approximately that of a 7/1 (mol/mol) mixture of coproporphyrin and uroporphyrin in 2.3M HCl. The porphyrin composition of this mixture resembles that of normal urine.

Absorption spectrum of acidified urine showing the procedure for the measurement of corrected absorbance (A) of the porphyrin peak.
Quality control
Material is available commercially (for example, Lyphocheck urine control; BioRad). The semiquantitative method gives concentrations that are lower than the target value quoted by the manufacturer.
Comments
Porphyrins adsorb strongly to calcium phosphate and other precipitates that may form in urine. It is therefore essential that particulate matter is not discarded before the addition of concentrated HCl. The method is reproducible but only semiquantitative because inaccuracies are produced by the correction for background absorbance, particularly at low porphyrin concentration, and by variation in the porphyrin composition of urine in disease.
Interpretation
The detection limit depends on the amount of background absorbance but concentrations of approximately 50 nmol/litre should be detected in urine of normal colour. Ideally, concentrations should be expressed as a ratio to creatinine concentration to correct for urine concentration. Increased concentrations require further investigation to identify individual porphyrins (table 2) and to distinguish secondary coproporphyrinuria from porphyria.1, 2 The most common cause of increased porphyrin excretion is coproporphyrinuria secondary to liver dysfunction, alcoholism, drug treatment, lead poisoning, and other miscellaneous conditions.2 Secondary coproporphyrinuria is not normally associated with other abnormalities of haem precursor metabolism; an exception being lead poisoning in which urinary ALA and erythrocyte zinc–protoporphyrin concentrations are also increased.
Normal urine contains predominantly coproporphyrin with uroporphyrin as a minor component. Thus, it is possible for the concentration of uroporphyrin and other acetic acid substituted porphyrins to be abnormal although the total porphyrin concentration remains normal, particularly in patients with PCT who are entering remission. Therefore, if there is a high index of clinical suspicion of porphyria in a patient with skin lesions, further investigation is advisable even when the total porphyrin concentration is normal. Measurement of individual porphyrins in urine or fluorescence spectroscopy of plasma will distinguish PCT from pseudoporphyria caused by non-steroidal anti-inflammatory drugs and other drugs,4 a condition in which porphyrin metabolism is normal.
PORPHYRINS IN FAECES
The total porphyrin content of faeces can be measured by direct spectrophotometry of an acidic extract of faeces, provided red fluorescent pigments derived from dietary chlorophyll, which also absorb light around 400 nm, are first removed by extraction with diethyl ether.16 Qualitative screening methods that depend on solvent extraction procedures are unreliable and should no longer be used.17
Measurement of total porphyrins in faeces
Accurately weigh to the nearest 0.1 mg a small aliquot of faeces (25–100 mg) in a glass stoppered tube. Prior homogenisation of the faecal sample (5–10 g wet weight) is not necessary as long as the aliquot is removed from an area that appears reasonably uniform to the naked eye. Liquid samples are unsuitable for quantitative analysis. Add concentrated HCl (1.0 ml), vortex mix until all particles are disintegrated, add diethyl ether (3.0 ml), vortex mix to form an emulsion, add distilled water (3.0 ml), and vortex mix for 30 seconds. Separate the phases by centrifugation and transfer the lower aqueous phase to a spectrophotometer cuvette using a glass Pasteur pipette. Record the absorption spectrum between 350 and 450 nm as described above. For samples with a high porphyrin concentration or high background absorbance, dilution with 2.5M HCl might be necessary.
Determine the dry weight of the sample by placing about 200 mg wet weight of faeces on to a preweighed glass slide and weighing to the nearest 0.1 mg. Dry to a constant weight in either an oven (105°C for 16 hours), microwave oven (medium power for 15 minutes in an 850 kW oven), or rotary evaporator. Whichever method is used, careful standardisation of the technique is required. For a microwave oven, conditions depend on batch size. It is convenient to standardise conditions for one batch size which is not altered. After cooling, weigh the slide of faeces to obtain the dry weight. If a peak is present in the 400 nm region, the total porphyrin in nmol/g dry weight is given by:  where A is the peak absorbance measured as described above for the determination of porphyrins in urine, 0.33 is the average micromolar extinction coefficient for a mixture of protoporphyrin and coproporphyrin (3/1; mol/mol) in 2.5M HCl, and 4.5 is the volume of the aqueous phase in millilitres and all weights are in grams.
where A is the peak absorbance measured as described above for the determination of porphyrins in urine, 0.33 is the average micromolar extinction coefficient for a mixture of protoporphyrin and coproporphyrin (3/1; mol/mol) in 2.5M HCl, and 4.5 is the volume of the aqueous phase in millilitres and all weights are in grams.
Quality control
No commercial material is available. A homogenised normal sample and one with a high porphyrin concentration should be divided into aliquots (about 0.5 g) to prepare control samples to include with each batch of analyses. Samples stored at −20°C are stable for up to one year.
Comments
Porphyrins are rapidly destroyed by peroxides, which accumulate in diethyl ether and similar solvents. Analar grade diethyl ether contains < 0.000015% ether peroxides and is suitable for use. It should be stored in the dark and discarded after two months.
The expression of results on a dry weight basis corrects for the moisture content of faeces. The procedure may be simplified with little loss in sensitivity or specificity by omitting the drying stage and using 50 nmol/g wet weight as the upper reference limit.18 Very occasionally, faeces contain substances that produce a very high background absorbance, making identification of any peak in the 400 nm region difficult. Such samples require analysis by alternative methods and are best referred to specialised laboratories.
Interpretation
An increased total faecal porphyrin concentration requires further investigation by fractionation, identification, and quantification of individual porphyrins using a technique, such as high performance liquid chromatography (HPLC), that separates coproporphyrin I and III isomers. Older separation methods based on solvent fractionation are unreliable.19 Total porphyrin concentrations are always increased during the symptomatic phase of VP and HCP and may be increased during an acute attack of AIP,16 but fractionation into individual porphyrins readily differentiates these disorders (table 2). In PCT, total faecal porphyrin excretion is increased in about 75% of patients with skin lesions but returns to normal with remission. Fractionation reveals a specific pattern of abnormalities (table 2) that distinguish this condition and other, much rarer uroporphyrinogen decarboxylase defects from all other porphyrias. Faecal analysis20 or fractionation of plasma porphyrins by HPLC21 is required for the differentiation of PCT from clinically similar bullous dermatoses in patients with chronic renal failure. Faecal porphyrin analysis should not be used for the diagnosis of EPP. Concentrations are normal in at least 40% of patients with this condition and false positives as a result of other causes of increased faecal porphyrin concentrations may confuse.
The most common causes of increased total faecal porphyrin concentrations are constipation, particularly if results are not expressed on a dry weight basis, and bacterial degradation of increased amounts of haem in the gut to protoporphyrin and related dicarboxylic porphyrins. The latter may produce substantial increases, which can be distinguished from other causes by the absence of evidence for porphyria from erythrocyte, plasma, and urinary measurements. The source of the increased haem may be dietary or relatively trivial—for example, epistaxis or bleeding gums, or pathological. Haem based tests for occult blood may or may not be positive depending on the amount and site of origin of the haem. The combination of secondary coproporphyrinuria and an increased faecal porphyrin owing to occult bleeding is not uncommon, and may cause confusion with porphyria unless PBG and individual porphyrins are measured.
A normal faecal total porphyrin excretion does not exclude latent VP or HCP.22, 23 Concentrations are invariably normal in children before puberty and may be normal in adults with latent disease or after prolonged remission.
PORPHYRINS IN ERYTHROCYTES AND PLASMA
Qualitative and quantitative methods for the determination of porphyrins in blood that depend on solvent fractionation and spectrophotometry, or visual inspection for porphyrin fluorescence, are insensitive or technically complex and should be replaced by simpler, fluorometric methods. The detection of porphyrin in erythrocytes by fluorescence microscopy24 requires special equipment and expertise and should be restricted to specialised centres.
The methods described below all require a spectrofluorometer fitted with a red sensitive photomultiplier (for example, Hamamatsu 928). If such equipment is not available locally, samples can be referred to a specialised laboratory because erythrocyte and plasma measurements are rarely required for the urgent assessment of acutely ill patients.
Determination of erythrocyte total porphyrin
This method is based on that described by Piomelli25 as modified by Blake et al.15 Porphyrins are separated from haem by solvent partition and measured fluorometrically.
Add EDTA anticoagulated whole blood (0.05 ml) to physiological saline (0.45 ml) in a glass or polypropylene tube, vortex mix and, while mixing continues, add 5 ml of a freshly prepared diethyl ether/glacial acetic acid (4/1; vol/vol) mixture. Continue vortex mixing for at least 15 seconds, centrifuge, and decant the whole supernatant carefully into a fresh tube. Add 2.7M HCl (3.0 ml), vortex mix, and allow phases to separate, either by centrifuging or leaving for 30 minutes in the dark. Transfer the aqueous phase to a suitable cuvette using a glass Pasteur pipette. With the emission wavelength of the spectrofluorometer at 602 nm, record the excitation spectrum from 350 nm to 450 nm. Similarly scan a standard uroporphyrin solution. The standard is prepared by diluting uroporphyrin-I-fluorescence standard (602 nmol/l) (Porphyrin Products Inc, available from Pierce and Warriner (UK) Ltd, Chester, UK) 50 fold with 2.7M HCl and storing aliquots in the dark at 4°C for up to six months.
Determine the haematocrit of the blood sample. For both sample and standard, measure the vertical peak height (H) in millimetres above a line joining the points at 380 nm and 430 nm. Calculate the total porphyrin concentration (μmol/litre erythrocytes) as follows:  The factor, 0.177, allows for the 90 fold dilution of the sample, conversion from nmol/litre to μmol/litre, and the fact that protoporphyrin (the main porphyrin in blood) is about half as fluorescent as uroporphyrin at equivalent concentrations in 2.7M HCl.
The factor, 0.177, allows for the 90 fold dilution of the sample, conversion from nmol/litre to μmol/litre, and the fact that protoporphyrin (the main porphyrin in blood) is about half as fluorescent as uroporphyrin at equivalent concentrations in 2.7M HCl.
Quality control
No commercial material is available. Normal and abnormal samples divided into 0.1 ml aliquots and stored at −20°C for up to six months are suitable. Alternatively, quality control material may be prepared by adding protoporphyrin to normal blood.15
Comments
Protoporphyrin is very susceptible to oxidation by ether peroxides. Erythrocytes contain free (unchelated) protoporphyrin and zinc–protoporphyrin. A solution of 2.7M HCl dissociates the zinc chelate so both forms of protoporphyrin are measured together. Instruments that measure zinc–protoporphyrin alone are not suitable for the diagnosis of EPP because they do not accurately measure the concentration of free protoporphyrin.
Interpretation
Total erythrocyte porphyrin concentrations are increased in EPP, congenital erythropoietic porphyria (CEP), the rare homozygous variants of the autosomal dominant porphyrias, iron deficiency, haemolytic anaemia, some other forms of anaemia, and lead poisoning. It is only in EPP and, very rarely, in sideroblastic anaemia that free protoporphyrin is increased to a much greater extent than zinc–protoporphyrin. In all other conditions, and in normal individuals, zinc–protoporphyrin predominates or, in CEP and other rare porphyrias, is a prominent component of a mixture of porphyrins. Therefore, all samples with an increased total porphyrin concentration should be investigated further to differentiate free protoporphyrin from zinc–protoporphyrin.
Qualitative determination of zinc–protoporphyrin and protoporphyrin
To preserve the zinc chelate, neutral or basic extraction conditions are required. Ethanol is a neutral reagent that extracts porphyrins without dissociating haem from haemoglobin.26
Add EDTA anticoagulated whole blood (0.05 ml) to phosphate buffered saline (PBS; 0.2 ml) in a polypropylene tube and mix thoroughly. Pipette 0.05 ml of this mixture into 95% (vol/vol) aqueous ethanol (1.0 ml), mix immediately, continue vortex mixing for 15 seconds, and then centrifuge immediately to pellet the precipitated protein. Transfer the clear supernatant to a suitable cuvette and record the fluorescence emission spectrum between 550 and 650 nm at an excitation wavelength of 415 nm. Emission peaks for zinc–protoporphyrin and free protoporphyrin are at 587 nm and 630 nm, respectively.
Interpretation
If the main peak is at 587 nm, EPP is excluded, whereas a pronounced predominance of the peak at 630 nm confirms the diagnosis of EPP. With experience, this test can be used to screen for EPP without the need for prior quantitative analysis.
Fluorescence emission spectroscopy of plasma porphyrins
The method described here22 was introduced by Poh-Fitzpatrick27 and is a useful front line investigation for suspected cutaneous porphyria.
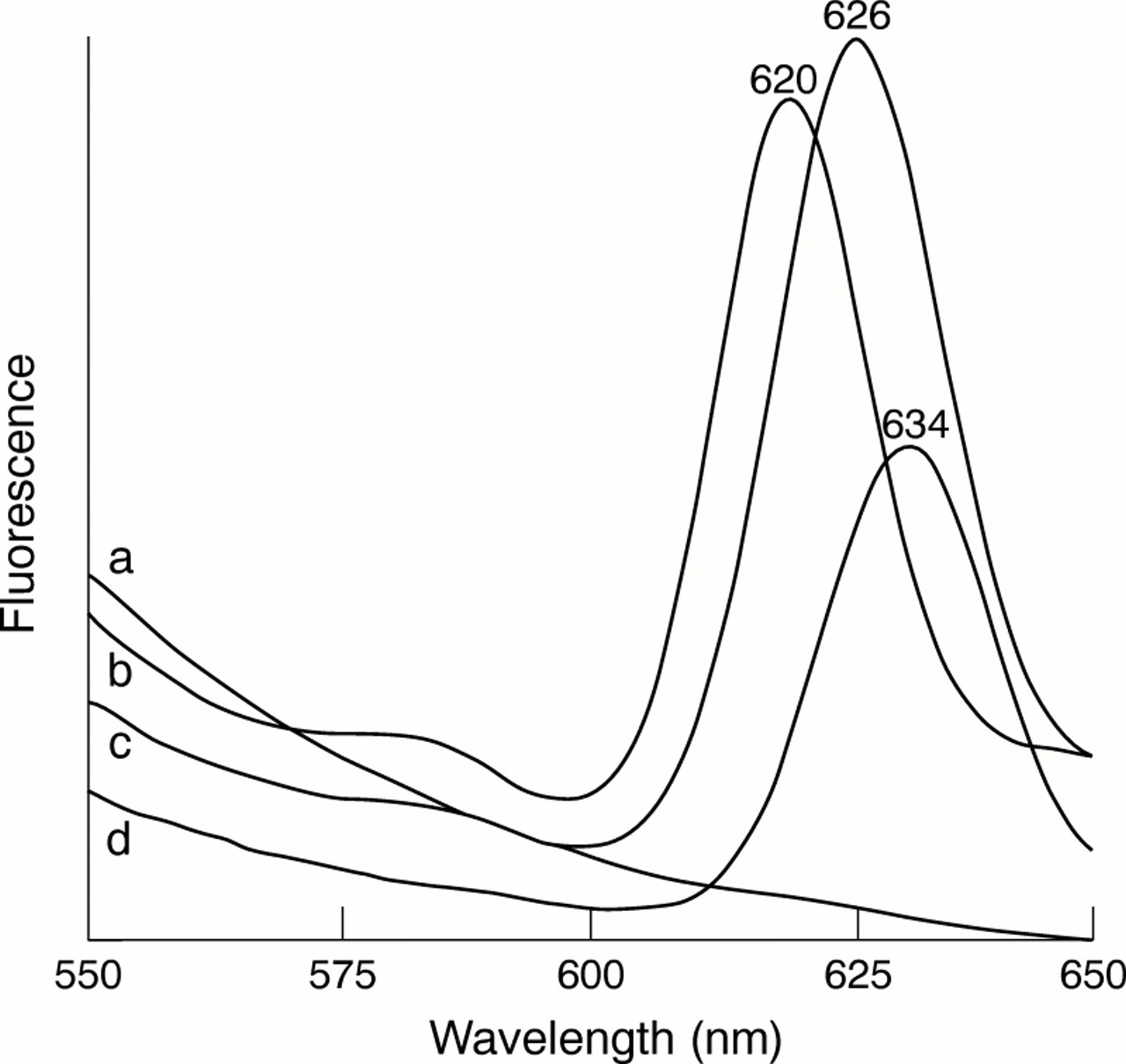
Add plasma (0.1 ml) to PBS (0.90 ml) in a spectrofluorometer cuvette and mix by inversion. Record the fluorescence emission spectrum between 550 and 650 nm with an excitation wavelength of 405 nm. Note the wavelength maximum for any peak above the background between 600 nm and 640 nm (fig 3).

{kind=link}
{kind=link}
{kind=link}
Fluorescence emission scans (excitation at 405 nm) of diluted plasma from (a) a normal subject and patients with (b) porphyria cutanea tarda, (c) variegate porphyria, or (d) erythropoietic protoporphyria.
Comments
The spectrofluorometer should be capable of detecting a small peak at a plasma porphyrin concentration of 10 nmol/litre. For the determination of the emission maximum, the spectrofluorometer should be calibrated with a solution of coproporphyrin in PBS at pH 7.4, which gives an emission maximum at 615 nm. It is important to establish a reference range by determining the maximum height above the background for normal plasma samples; most but not all will show no emission peak (fig 3).
Interpretation
Table 2 shows the emission maximum wavelengths for the cutaneous porphyrias. A normal fluorescence emission scan in plasma from a patient with clinically active skin lesions excludes all cutaneous porphyrias. The scan can become normal in PCT and HCP as skin lesions heal, and the diagnosis may be missed unless individual porphyrins are also measured in urine and faeces from such patients.
Plasma porphyrin fluorescence scanning is particularly useful for the differentiation of VP from other bullous porphyrias. The plasma in VP contains porphyrin covalently bound to protein with a fluorescence emission maximum at 624–626 nm.27 Furthermore, the plasma abnormality persists for many years after complete clinical remission, even after faecal porphyrin excretion has returned to normal, and is also present in many adults with clinically latent VP.22
The plasma porphyrin concentration may be increased in conditions in which porphyrin excretion is impaired, such as renal failure and cholestasis. Although plasma porphyrin concentrations are usually higher in chronic renal failure with PCT than in renal failure alone, unequivocal diagnosis of PCT in this situation is best achieved by faecal porphyrin analysis20 or fractionation of plasma porphyrins by HPLC.21
External quality assurance schemes
It is good laboratory practice to participate in external quality assurance schemes. Because porphyrias are rare disorders, this is the only means by which many laboratories will have the opportunity to become familiar with positive specimens. Schemes are provided by the Welsh Quality Assurance Scheme, University Hospital of Wales, Heath Park, Cardiff CF4 4XW (urinary PBG and total porphyrin, plasma porphyrin) and by RCPA-AACB Chemical Pathology QAP Group, Flinders Medical Centre, Bedford Park, South Australia 5042.