Article Text

Abstract
Modern molecular methods for precancer diagnosis have expanded the range of detectable disease to a preclinical level and provided material for histopathological correlation. The precancer scenario begins with sporadic acquisition of rare PTEN mutation bearing glands, which are morphologically unremarkable, and progresses to discrete foci of cytologically altered glands, readily visible on routinely stained sections. Clinical outcome studies of women with endometrial lesions have established threshold diagnostic features that confer increased cancer risk. This class of high risk lesions has been designated endometrial intraepithelial neoplasia (EIN). EIN is diagnosed by presence of cytological demarcation, crowded gland architecture, minimum size of 1mm, and careful exclusion of mimics. Most EIN lesions have been diagnosed as atypical endometrial hyperplasias in the World Health Organisation system. Specialised molecular and morphometric analyses have been extremely useful in redefining clinically relevant premalignant endometrial disease, but translation to improved patient care requires the informed participation of pathologists.
- endometrium
- hyperplasia
- diagnosis
- endometrial intraepithelial neoplasia
- precancer
- terminology
- EIN, endometrial intraepithelial neoplasia
- VPS, volume percentage stroma
Statistics from Altmetric.com
Endometrial carcinoma is the most common malignancy of the female genital tract1 and its most frequent subtype, endometrioid carcinoma (“type I” cancers2,3), is often preceded by a histologically evident precursor lesion.1,4 Accurate and sensitive recognition of these precursors, which generally have fallen under the diagnostic umbrella of “hyperplasias”,5,6 has great clinical value as an early warning of heightened cancer risk and a potential target for preventative treatment. Public awareness of the need for early diagnosis is also on the rise, in part because of widespread media coverage of the endometrial tumorigenic effects of hormonally active medications, such as tamoxifen,7,8 and the recognition that everyday dietary or environmental exposures to compounds with oestrogenic activity9–11 are much more common than previously appreciated.
Histopathological plasticity of normal and pathological endometrial tissues alike presents formidable barriers for classification of biologically homogenous groups into reproducible morphological diagnostic categories. Premalignant lesions of the endometrium can demonstrate non-endometrioid differentiation (squamous, mucinous, and tubal changes are common)12 and, similar to normal tissues, may transiently change their architecture and cytology in response to fluctuating oestrogens and progestins. The effects of progestins on endometrial glandular cytology are a particular diagnostic problem. In a progestin rich environment, nuclei of premalignant glands tend to diminish in size and acquire a rather bland chromatin pattern, which makes them appear less “atypical”. Paradoxically, the nuclei of normal glands become enlarged and rounded—features associated with atypia.
“Histopathological plasticity of normal and pathological endometrial tissues alike presents formidable barriers for classification of biologically homogenous groups into reproducible morphological diagnostic categories”
Pathologists have applied different strategies to harness a workable diagnostic scheme from this elusive group of endometrial precancers, resulting in a variety of classification schemes,13–16 confused by overlapping terminology. A reductionist approach attempts to uncover those minimal shared features that correspond to a relevant clinical outcome. This had led to the strong association of cytological atypia with cancer risk,17–19 thereby suggesting that atypical endometrial hyperplasias are the subset of hyperplastic endometrial lesions most likely to progress to carcinoma. Interobserver reproducibility in the assessment of the presence or absence of cytological atypia is poor,15,20,21 an alarming state of affairs in light of the dominance afforded this feature in patient management. In contrast, a divisionist approach attempts to improve the homogeneity of diagnostic groups by classifying a broad spectrum of disease into a large number of discrete categories. An example is when endometrial hyperplasia cytology and architecture are separately graded on a three part scale, yielding nine permutations of endometrial hyperplasia. An unfortunate side effect is the degradation of reproducibility proportionate to the number of categories used.15 Furthermore, there is diminishing clinical benefit in having more diagnostic categories than therapeutic responses.
WHAT HAS HAPPENED LATELY?
Molecular diagnostic methods compatible with paraffin wax embedded archival human tissues have permitted histopathological correlation with genetically defined premalignant endometrial disease.22 This was first done using markers capable of distinguishing monoclonal from polyclonal tissues, in search of predicted monoclonal premalignant lesions. Non-random X chromosome inactivation23–25 and clonal propagation of altered microsatellites12 confirmed that many atypical endometrial hyperplasias are indeed monoclonal, and these clones have an altered genotype that is conserved in the subsequent carcinomas they produce.21,26 Establishing lineage continuity between monoclonal putative precancers and cancer is crucial in the molecular discrimination of precancers from other “dead end” benign processes, such as the monoclonal stroma of endometrial polyps.27,28
The histopathology of monoclonal putative endometrial precancers is identical to that seen by computerised morphometric analysis to increase the risk of endometrial adenocarcinoma.21,29 Morphometric analysis of an index series of endometrial lesions of known clonal composition showed that most monoclonal putative precancers had a high risk D score, a weighted index of computer measured cytological and architectural features that are highly predictive of concurrent30 or future31,32 endometrial adenocarcinoma. Of the three variables used to calculate the D score, the architectural feature of volume percentage stroma (VPS) has by far the greatest predictive value.21,31 As glands become more crowded in monoclonal precancers, the VPS drops below a threshold of 55%.21 This establishes formal architectural features as useful cancer predictive criteria in addition to cytology. One caution is that some completely benign conditions such as normal basalis, endometrial polyps, and secretory endometrium can have VPS < 55% and must be excluded.
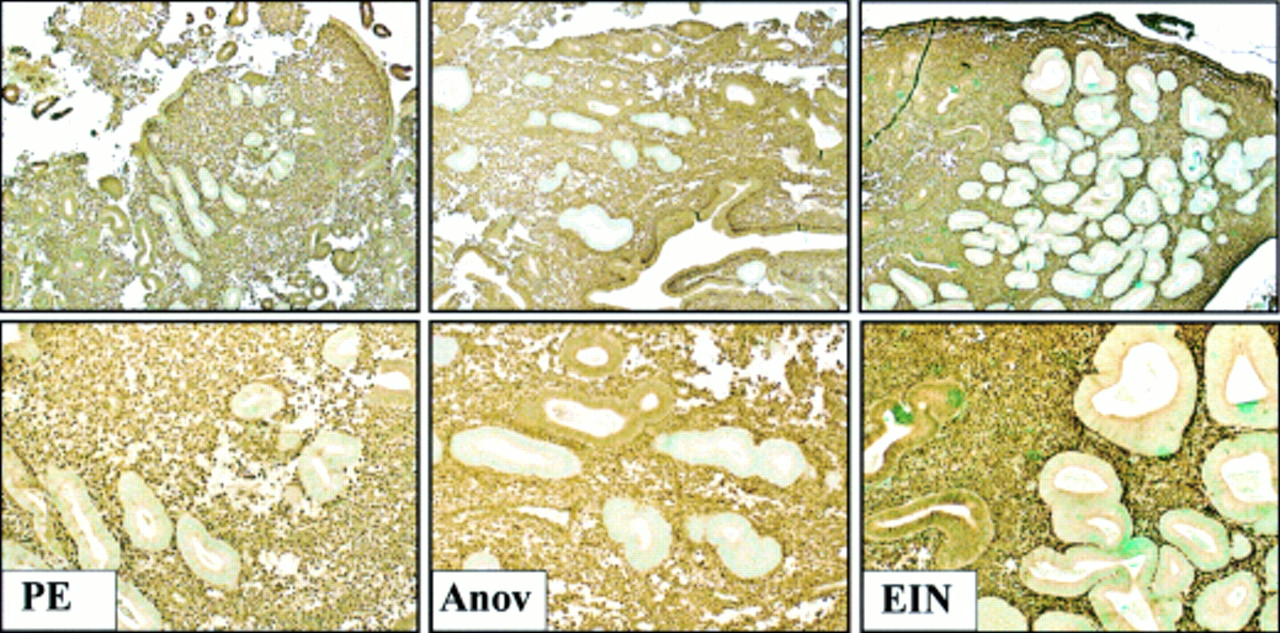
Immunohistochemical biomarkers have further pushed the detection limit of premalignant endometrial disease to a truly preclinical stage, disclosing a much higher prevalence of early stage disease than previously suspected. DNA based clonal analysis typically requires DNA isolated from a 1–2 mm diameter area of a tissue section, limiting the physical resolution of small lesions. The PTEN tumour suppressor gene33,34 is inactivated in up to 83% of endometrial adenocarcinomas.35–37 Because loss of the PTEN protein occurs at or near the time of the initiation of carcinogenesis,37–40 premalignant and malignant endometrial glands can be distinguished by the loss of this marker. Thus, PTEN immunohistochemistry shows lesion specific loss of the PTEN protein in 63% of endometrial intraepithelial neoplasia (EIN) lesions,41 confirming that these tightly aggregated glands are clonal outgrowths of genetically abnormal cells. However, immunohistochemistry has the potential to uncover individual or rare PTEN null glands that may represent a stage of disease not yet evident on routine haematoxylin and eosin histology (fig 1). Tiny clusters of architecturally and cytologically unremarkable PTEN null glands are seen in 43% and 56%, respectively, of normal proliferative and anovulatory endometria.41 These PTEN null glands of normal cycling proliferative endometria contain somatically acquired deletions and/or mutations of the PTEN gene itself, and persist between menstrual cycles.41 Persistence between menstrual cycles probably results from the inclusion of mutant cells in the regenerative population that repopulates the functionalis after each menses.

Broad spectrum of premalignant endometrial disease demarcated by PTEN immunohistochemistry. PTEN immunohistochemistry with monoclonal antibody 6H2.137,41,42 delimits the distribution of PTEN null pale glands (pale counterstain) in proliferative (left, “PE”), anovulatory (middle, “Anov”), and endometrial intraepithelial neoplasia (right, “EIN”) endometria. Loss of PTEN protein expression is abnormal, caused by mutations and/or deletion of the PTEN gene itself.41 A comparison of PTEN null and expressing glands shows no distinguishing features in proliferative and anovulatory endometria: these mutant clones unrecognised by haematoxylin and eosin staining represent preclinical disease. In contrast, PTEN null glands in EIN lesions have an altered cytology and are more tightly packed (low VPS; volume percentage stroma), which permits the identification of these localising lesions by routine histology. Although PTEN immunohistochemistry is informative for educational purposes, its low sensitivity (about half of EIN lesions express the PTEN protein) and specificity (most PTEN null glands are seen in histologically normal endometrium) in the detection of clinically relevant EIN lesions makes it impractical for routine patient care. Images reprinted, with permission, fromwww.endometrium.org.
“The histopathology of monoclonal putative endometrial precancers is identical to that seen by computerised morphometric analysis to increase the risk of endometrial adenocarcinoma”
The endometrium has the highest prevalence (43%) of non-familial premalignant disease yet shown experimentally in any intact normal human tissue.41 Most of this is “latent” in that additional changes are required before it becomes clinically evident, and these occur at a low efficiency. It is not necessary to invoke any special mechanisms of mutation to explain this high rate of initiation of endometrial carcinogenesis. The rate of sporadic mutagenesis in human cells has been estimated at 10−7 mutations/gene/cell division,43 consistent with the prediction of hundreds of cells for each gram of proliferative tissue (109 cells/g) that generate “first hits” of a multistep carcinogenesis44 pathway. The PTEN gene acts as a gatekeeper for endometrial carcinogenesis, being one of the initial genetic changes seen in this process.40 As comparable biomarkers for neoplastic initiation become available in other tissue sites, it is anticipated that similarly high rates of initiation will be seen in other tissues.
DEFINING PREMALIGNANT DISEASE
A comprehensive genetic and histopathological model of endometrial carcinogenesis can now be constructed. Initiating sporadic mutations, such as loss of PTEN function, occur quite frequently within the endometrial regenerative pool, at such a high rate that they can be considered part of background “normal” genetic events. These mutant clones remain indistinguishable from non-mutant glands in normal cycling and anovulatory endometrium. Involution or expansion of mutant clones in response to non-genetic factors is one possible mechanism whereby the ambient hormonal state may modify the risk of endometrial cancer. Interestingly, the PTEN gene appears to be hormonally regulated, with greatest physiological endometrial gland expression in an oestrogen rich environment.45 Thus, the effects of diminished PTEN tumour suppressor function are probably accentuated under the very circumstances known to increase cancer risk: protracted oestrogen exposure unopposed by progestins.46,47 Mutant glands subsequently acquire additional genetic damage and then become recognisable as focal lesions by their altered cytology and crowded architecture. It is these lesions that pathologists can diagnose (table 1).
The term endometrial intraepithelial neoplasia (EIN) has been proposed50 as a descriptive term for monoclonal endometrial precancers whose distinctive histopathology is characterised by those morphometric features21 that have been documented to increase the risk of cancer.30–32 This category of lesions has now fulfilled most of those postulates predicted for clinically relevant precancerous disease (table 2). Their natural history dictates that EIN lesions should be ablated by hormonal (progesterone) or surgical (hysterectomy) means.
Features of endometrial precancers
DIAGNOSING PREMALIGNANT DISEASE
EIN is diagnosed by a pathologist using haematoxylin and eosin stained sections prepared from a representative endometrial sample. Although computerised morphometry has been a useful tool in identifying features characteristic of EIN,18,21,30–32,61 such equipment is not required for routine diagnosis. Subjective interpretation of stated criteria by a pathologist at a standard microscope is often adequate, or a simple ocular grid may be used as a counting device for area measurements (VPS). Diagnostic accuracy may be severely compromised by exogenous progestin containing hormonal treatments. For this reason, primary diagnosis or follow up surveillance of a suspected EIN lesion should be based whenever possible on a sample obtained while the patient is not on therapeutic hormones. For those patients on progestins, diagnostic tissue can be obtained after two to four weeks of discontinuing exogenous hormone treatment, after completion of a withdrawal bleed.
A simple process for diagnosing EIN lesions can be broken down into component steps as follows. Additional images and an interactive tutorial are available online (www.endometrium.org ).
Glandular crowding: VPS < 55%
A tissue sample can be divided into stromal and glandular compartments, and their relative proportions used to assess glandular crowding (fig 2). Focusing on the stroma ensures that fragmented areas are not misinterpreted and provides a homogenous field amenable to visual assessment. EIN lesions have a stromal volume less than that of the glands.

{kind=link}
{kind=link}
Architectural features of endometrial intraepithelial neoplasia (EIN). A visual impression of the appearance of endometria with differing volume percentage stroma (VPS) is shown diagrammatically (below) and in photomicrographs. Large, or dominant cysts, such as those shown in the middle panel, top, should be avoided in calculating VPS. VPS measurements are indicated for three benign (top) and EIN (middle) endometria which divide at a threshold VPS of 55%. The EIN lesions are further characterised by cytological changes in the areas of low VPS compared with the background (not shown). Haematoxylin and eosin photomicrographs. Images reprinted, with permission, from www.endometrium.org.
Cytological demarcation
EIN lesions have an abnormal cytology within areas where glands are more tightly packed than is seen in the background endometrium. The manner of cytological change in EIN varies considerably and can include, but is not limited to, increased variation in nuclear size and contour, a clumped or granular chromatin texture, a change in nucleoli, a change in the nuclear/cytoplasmic ratio, and altered cytoplasmic differentiation. The absolute cytological appearance is also influenced by tissue processing methods, the extent of reactive/degenerative change, and the hormonal environment. Beware diagnosing an EIN lesion if the cytology is identical between areas with crowded compared to uncrowded glands! Many of these are artifactual disruptions where the stroma is sheared and glands pushed together.
Size >1 mm
The diagnosis of EIN requires a contiguous field of glands sufficiently large to permit estimation of the VPS: lesions with a largest diameter exceeding 1–2 mm. This was the minimum size required for accurate morphometric correlation of lesion histology with clinical outcome.30–32 Lesion size is measured across the perimeter enclosing cytologically altered glands that are closely arranged (VPS < 55%).
Exclude confounding benign processes
Accurate diagnosis requires the exclusion of overlapping entities. EIN criteria are meant to be applied to endometrial functionalis. The lower uterine segment and basalis must be excluded. Furthermore, degenerative (stromal breakdown) or pure hormonal effects (anovulation) must be diagnosed as such, with the realisation that they may contain some features of altered glandular architecture or cytology that overlap with those of bona fide EIN. It is the distinction between these benign endometrial lesions and EIN that produces the greatest challenge in diagnosis. Some specific presentations that might be falsely interpreted as premalignant must be excluded, including very small atypical areas, polyps, normal secretory endometrium, and inflamed endometrium. Glands pushed together after the breakdown of the intervening stroma are commonly overinterpreted as premalignant, especially when having degenerative epithelial changes that mimic atypia. In those cases where an EIN lesion is suspected within one of these backgrounds, the diagnosis relies heavily upon contrasting the localising features of the EIN lesion to the regional context.
Exclude carcinoma
Carcinoma should be distinguished from EIN because it must be surgically, not hormonally, ablated. It should be borne in mind that the absence of carcinoma in a tissue biopsy does not exclude the possibility that the patient has a cancer that was not sampled during the biopsy procedure. An opinion should always be rendered based upon available material, and clearly stated.
“Beware diagnosing an endometrial intraepithelial neoplasia lesion if the cytology is identical between areas with crowded compared to uncrowded glands!”
Cancers in most cases may be identified as separate from EIN by the presence of solid areas of neoplastic epithelium or a maze-like rambling of uninterrupted lumens, which indicate interruption of the normal gland–stroma relations. Poorly differentiated and papillary serous carcinomas may be identified by their distinctive appearance. In some small, distorted, or poorly oriented samples, EIN may be indistinguishable from well differentiated carcinomas. This should be mentioned in the report to avoid inappropriate progesterone treatment of an incompletely sampled endometrial adenocarcinoma. A fraction of EINs will thus be upgraded to carcinoma upon more extensive sampling—either from a follow up curettage or hysterectomy.
If the neoplastic epithelium is detached from its stroma, or present only in very small tissue fragments, it may at times be impossible to resolve the differential diagnosis between EIN and carcinoma. In these instances, a clear diagnosis of “neoplastic endometrial epithelium, cannot exclude carcinoma” will alert the clinician to the problem. Lastly, always remember that surgical treatment of endometrial cancers may be modified by the distribution of the lesion. The surgical management of a cancer completely contained within an excised polyp may be different to a well differentiated cancer that extends to involve the lower uterine segment.
Take home messages
-
Recently developed molecular methods for precancer diagnosis have expanded the range of detectable disease to a preclinical level, disclosing a much higher prevalence of early disease than previously suspected
-
The precancer scenario begins with sporadic acquisition of rare PTEN mutation bearing glands, which are morphologically unremarkable, and additional genetic damage results in a progression to discrete foci of cytologically altered glands, readily visible on routinely stained sections
-
Clinical outcome studies of women with endometrial lesions have established threshold diagnostic features that confer increased cancer risk and these lesions has been designated endometrial intraepithelial neoplasia (EIN).
-
EIN is diagnosed by presence of cytological demarcation, glandular crowding (volume percentage stroma < 55%), minimum size of 1mm, and careful exclusion of mimics
-
Specialised molecular and morphometric analyses have been powerful tools in redefining clinically relevant premalignant endometrial disease, but translation to improved patient care requires the informed participation of pathologists
WHAT LIES AHEAD?
Isolated PTEN negative glands in normal endometria may well be the earliest detectable phases of endometrial tumorigenesis yet seen, but the clinical relevance of such small lesions remains to be determined.37,41 This situation is very similar to the first use of the polymerase chain reaction in the diagnosis of infectious diseases, where organisms could be detected at a burden well below that associated with clinical disease. Can one PTEN null gland in an “about to be shed” endometrium possibly increase the risk for carcinoma? Disease burden (lesion size) and the likelihood of persistence (influenced by hormonal state and location of lesion within the functionalis/basalis) are poorly understood factors that probably interact in determining the ultimate cancer risk. Sorting out the natural history of latent disease, a stage that had long been hypothesised but was undocumented, is a major challenge for the future.
The impact of molecular diagnosis and computerised morphometric analysis on the future practice of clinical pathology will be determined by pathologists. Endometrial precancer diagnosis has clearly benefited from those diagnostic insights contributed by these investigational tools. The result is revised diagnostic criteria, rather than obsolescence of standard microscopy. As long as pathologists actively participate in critical evaluation of new data, and are open minded to its constructive use, it is likely that this precedent can be followed in other organ sites.