Article Text

Abstract
Aim: To investigate necropsy request practices at the University Hospital of the West Indies, Jamaica, to determine the extent to which these might influence the declining necropsy rates. This is the first such study from a developing country.
Methods: The necropsy service was audited prospectively over a six month period, and data relating to non-coroner’s (hospital) necropsy requests, including the clinical service and post of the clinician involved, were documented. The reasons for non-request were recorded for deaths in which a necropsy was not requested, in addition to the reasons given by pathologists for not performing necropsies in cases that were requested but not done. The overall, non-coroner’s, and coroner’s necropsy rates in addition to the non-coroner’s necropsy request and success rates were calculated.
Results: There were 364 deaths comprising 323 non-coroner’s and 41 coroner’s cases. The overall, non-coroner’s, and coroner’s necropsy rates were 29.2%, 20.2%, and 38.7%, respectively. The non-coroner’s necropsy request rate was 35.3% with a success rate of 65%. Seventy five per cent of the requests were made by non-consultant clinicians and on the internal medicine service, which accounted for most of the non-coroner’s deaths; necropsy requests were biased towards younger patients (p < 0.0001). Confident clinical diagnosis was the main reason for not requesting a necropsy, and the primary reason for refusing to perform a necropsy was that the request had been made too long after death.
Conclusions: These findings show a relatively high necropsy success rate in the face of a comparatively low necropsy request rate, and indicate that necropsy rates can be increased if clinicians make more necropsy requests in a timely manner in patients of all ages.
- autopsy request practices
- necropsy request rates
- necropsy rates
- Jamaica
- UHWI, University Hospital of the West Indies
- UWI, University of the West Indies
Statistics from Altmetric.com
Despite consistent confirmation of the importance of the necropsy in the practice of modern medicine, necropsy rates have shown a worldwide decline over the past several decades.1–6 Recently, we examined our necropsy rates at the University Hospital of the West Indies (UHWI) in Jamaica over the 30 year period 1968 to 1997 and documented a significant fall in the overall rate from 65.3% in the first decade to 39.3% in the third, and a concomitant fall in the non-coroner’s (hospital) necropsy rate from 57.5% to 31.5%.7 The latter is now below the figure of 35% recommended by the Royal College of Pathologists.8 The factors contributing to declining necropsy rates have been examined and discussed in several reports from developed countries, and may be broadly grouped to include administrative policies, the attitudes of the medical profession, manpower, and the attitudes of the public.9–12 Where the medical profession is concerned, it is well recognised that the number of hospital necropsies performed at any institution depends heavily on requests being made by the relevant clinicians, and that inappropriate delegation of clinical necropsy requests to the most junior clinicians has contributed to falling necropsy rates.13
Therefore, we decided to conduct a prospective audit of our necropsy service in an attempt to establish a possible link between our declining necropsy rates and the necropsy request practices of our clinicians. We also sought to document the necropsy success rate and examine the reasons why pathologists did not perform necropsies in cases where a necropsy was requested but not done. To the best of our knowledge, this study represents the first such report from a developing nation.
“Inappropriate delegation of clinical necropsy requests to the most junior clinicians has contributed to falling necropsy rates”
MATERIALS AND METHODS
Our study took the form of an audit of the necropsy service of the department of pathology, University of the West Indies (UWI), which prospectively examined data related to deaths and autopsies at the UHWI—the 500 bed, multidisciplinary teaching hospital attached to the faculty of medical sciences at the UWI in Jamaica—over the six month period July to December 1999. We designed a simple questionnaire that elicited the following information: the age and sex of the deceased, the clinical service under which the patient was managed, the relevant clinical diagnoses, and whether or not a necropsy was requested. If requested, the post of the relevant clinician was recorded and, if not, we documented the reason given for not requesting the necropsy. We also recorded the reasons that necropsies were not performed in those instances where a necropsy was not performed despite being requested. The information regarding necropsy requests was extracted for non-coroner’s necropsies only (coroner’s (medico-legal) necropsies are mandatory in our institution), and was obtained by a combination of abstraction from the patients’ notes and by administering the questionnaire by telephone to the clinicians concerned. The clinical staff were not forewarned of our study and anonymity was proffered to those doctors who participated.
These data were used to calculate the following:
-
The overall necropsy rate for the study period—the number of necropsies performed as a percentage of the total number of deaths.
-
The non-coroner’s necropsy rate—the number of non-coroner’s necropsies performed as a percentage of the number of non-coroner’s deaths.
-
The coroner’s necropsy rate—the number of coroner’s necropsies performed as a percentage of the total number of necropsies performed.
-
The necropsy request rate—the number of non-coroner’s necropsies requested as a percentage of the total number of non-coroner’s deaths.
-
The necropsy success rate—the number of non-coroner’s necropsies performed as a percentage of the number of non-coroner’s necropsies requested.
Statistical analysis
The data were expressed as counts or per cents and κ2 statistics was used to determine associations between variables. The data were analysed using Stata version 7 statistical software for Windows (Stata Corporation, College Station, Texas, USA).
RESULTS
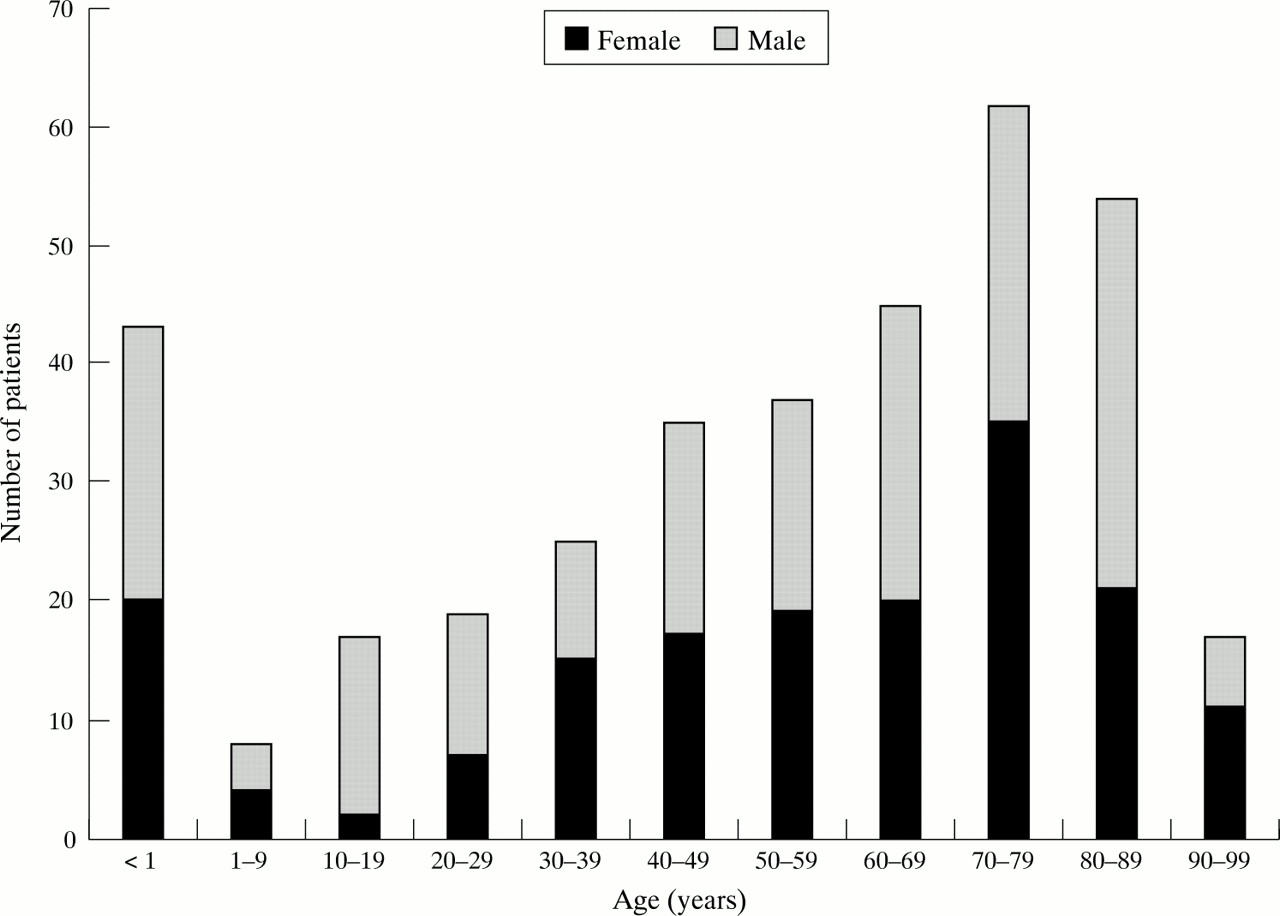
The total number of deaths for the six month study period was 364; namely, 323 non-coroner’s cases and 41 coroner’s cases. There were 191 male and 173 female patients (male : female ratio, 1.1 : 1), ranging in age from 1 day to 97 years (fig 1). The ages of two female patients were unknown.
{kind=link}
Breakdown of patients by age and sex (n = 362). Age unknown for two female patients.
Table 1 presents the overall figures for deaths and necropsies by service. The total number of necropsies performed during this period was 106, giving an overall necropsy rate of 29.2%. The non-coroner’s necropsy rate was 20.2%, and the coroner’s necropsy rate was 38.7%. The largest number of deaths occurred under the internal medicine service, which had the lowest necropsy rates by service, excluding oncology, in which no necropsies were performed. The highest non-coroner’s necropsy rates were seen for deaths occurring in the obstetrics and gynaecology, accident and emergency, and child health services. All deaths in the obstetrics and gynaecology service were neonatal; there were no maternal deaths.
Number of deaths, number of necropsies, overall necropsy rates, and non-coroner’s necropsy rates by clinical service
A total of 338 patient records (92.9% of deaths in the study period) were available for further analysis: 297 non-coroner’s cases and 41 coroner’s. The 26 missing records were distributed as follows: obstetrics and gynaecology, seven (six were stillbirths); accident and emergency, five; internal medicine, three; oncology, zero; child health, six; surgery, two; intensive care unit, two; and service unknown, one. Table 2 shows the request and success rates for the 297 non-coroner’s cases by service. The necropsy request rate was 35.3% and all services, with the exception of surgery, showed necropsy success rates in excess of 60%. The overall necropsy success rate was 65%.
Necropsy request and success rates for 297 non-coroner’s deaths
Table 3 details the request and success rates for non-coroner’s cases in the internal medicine service. There was a significant association between necropsy requests and patient age, with a higher proportion of necropsy requests coming from the younger age groups (p < 0.0001), although most deaths (63.0%) occurred in patients 65 years and older. However, there was no significant association between the age of the patients and the necropsy request being granted.
Necropsy request and success rates for non-coroner’s deaths occurring in the internal medicine service
Overall, most necropsy requests were made by non-consultant clinicians (interns and residents) and there was no significant association between clinician grade and the granting of necropsy (table 4). Thirty five of the 100 necropsy requests were not granted and the reasons are outlined in table 5. Table 6 details the reasons given in 68 of the 197 non-coroner’s cases in which a request for necropsy was not made; a reason was not stated for the remaining 129 cases.
Non-coroner’s necropsy requests by grade of clinician
Reasons for refusal of non-coroner’s necropsy requests
Reasons why necropsies were not requested by clinicians
DISCUSSION
Necropsy rates at the UHWI have shown a consistent decline over the past three decades,7 and the data from our study demonstrate a continuation of this trend, with an overall necropsy rate of 29.2% and an overall non-coroner’s necropsy rate of 20.2%. This is similar to the trend that has been reported worldwide and various reasons have been proffered to explain this, including poor necropsy request practices.1,2,14 Our study is the first to document necropsy request practices in our institution and we could find no similar reports from developing countries such as ours.
Despite the fact that this was a prospective study, we encountered problems in retrieving some of the patients’ files because they were misplaced in transit through various administrative subdepartments. In addition, we were unable to obtain reasons for the non-request of necropsies in some of the non-coroner’s deaths because there is no provision on our death card/necropsy request form for the documentation of such a reason, and it was not always possible to contact the clinicians involved while they could recall the exact details of the cases.
The highest non-coroner’s necropsy rates were seen for the obstetrics and gynaecology, accident and emergency, and child health services, and these services also had the highest request rates. In contrast, internal medicine, in which most deaths occurred, had the second lowest non-coroner’s necropsy rate and the lowest request rate (excluding oncology). These data support the direct link between non-coroner’s necropsy rates and request rates in our institution, a finding that has been previously documented elsewhere.14 In addition, analysis of necropsy requests in relation to patient age in the internal medicine service showed a significantly greater likelihood for necropsies to be requested in younger versus older patients, although most of the deaths occurred in patients 65 years and older. Other studies have shown a similar trend3,15,16 and, as suggested by Ahronheim et al,16 the deaths of elderly patients are more likely to be attributed to “natural causes”, despite there being significant discordance between clinical and postmortem diagnoses when necropsies are performed in this age group.
Residents made most of the necropsy requests (68%), which is not surprising because they are responsible for the day to day management of wards. These results are similar to those of Start et al,13 who reported that house officers, senior house officers, and registrars (the equivalent of our residents) made most of the requests, whereas consultants requested the smallest proportion. Data from this study do not measure the degree of consultant supervision of this process, but it is accepted that it is the responsibility of consultants to obtain permission for the performance of necropsies.8 Even if this responsibility is allocated to junior staff, they should be trained to approach relatives in a sensitive and informed manner, which would maximise the likelihood of obtaining consent.
“If our necropsy rates are to attain recommended international standards our data suggest that clinicians should be educated as to the value of the necropsy in patients of all ages, with a view to improving their necropsy request rates”
The overall necropsy request rate was low but, once requested, necropsies stood a good chance of being done, with an overall success rate of 65%. This success rate showed much less variation with patient age and clinical service than did the request rate. Most cases were refused either because the request was made too long after death (beyond the four day limit set by our department), or arrived in the department without the requisite signed consent form. Both of these factors fall under the ambit of the relevant clinicians and are beyond the control of the pathologists. In our institution there are suboptimal facilities for the performance of human immunodeficiency virus/AIDS necropsies according to international safety regulations, and therefore these necropsies are not done.
Analysis of the reasons obtained for the non-request of necropsies point to a strong reliance on clinical acumen, in addition to confidence in imaging and other diagnostic procedures. This is despite the fact that it has been well documented that advances in imaging and other diagnostic technology have not significantly altered the rates of clinical and necropsy discordance over the past several decades.17–20 Terminal illness was the third most common reason for non-request of necropsy, with most of these patients being under the oncology service. Although we found a relatively low percentage of refusal of consent for necropsy by relatives in cases for which a reason for non-request was given, other studies have documented an unwillingness of relatives to provide consent in up to 69% of cases.21,22
In conclusion, the necropsy remains an important form of medical audit, while providing avenues for medical education and research. Despite this, we have documented a continuing decline in our overall and non-coroner’s necropsy rates, which varied across clinical services. The necropsy request rate was relatively low and varied with patient age and clinical service in contrast to the success rate, which was uniformly high. Most of the necropsy requests were made by non-consultant clinicians (residents and interns). Where reasons were obtained for the non-request of necropsies, most related to confidence in clinical impressions and diagnostic technologies. In most of the cases in which a necropsy, having been requested, was not performed, the reason was related to failure on the part of the relevant clinician to accede to the guidelines established by our department.
The results of our study are similar to those previously reported from developed countries. If our necropsy rates are to attain recommended international standards our data suggest that clinicians should be educated as to the value of the necropsy in patients of all ages, with a view to improving their necropsy request rates. This might entail implementing some of the recommendations made by Sinard and Blood,23 such as orientation conferences and written guidelines for new residents and interns to make them more aware of the importance of the necropsy and how best to approach grieving relatives to obtain consent for non-coroner’s cases. In our setting, the importance of timely requests in keeping with our departmental guidelines must also be emphasised. Failure to deal with these issues will probably result in the continuing decline of the necropsy, with the concomitant loss of all of its potential benefits.
Take home messages
-
Although the necropsy is an important form of medical audit, there has been a continuing decline in overall and non-coroner’s necropsy rates
-
The necropsy request rate was low and varied with patient age and clinical service in contrast to the success rate, which was uniformly high
-
Most of the necropsy requests were made by non-consultant clinicians so that educating new residents and interns about the importance of the postmortem examination might help increase the rate of necropsy
Acknowledgments
The authors thank Dr M Reid for assistance with the statistical analyses.