Article Text

Abstract
MUCs are glycoproteins with various roles in homeostasis and carcinogenesis. Among other actions, MUC1 may inhibit cell–cell and cell–stroma interactions and function as a signal transducer, participating in cancer progression. In contrast, MUC2 is normally found only in goblet cells, where it contributes to the protective barrier function of these cells. Recently, a tumour suppressor role has been demonstrated for MUC2, and both MUC1 and MUC2 appear to have important roles in pancreatic neoplasia. MUC1 appears to be a marker of aggressive phenotype and may facilitate the vascular spread of carcinoma cells. In contrast, MUC2 is rarely detectable in aggressive pancreatic tumours, but is commonly expressed in intraductal papillary mucinous neoplasms (IPMNs), which are rare, indolent tumours, in intestinal IPMNs, and in indolent colloid carcinomas. MUC2 appears to be not only a marker of this indolent pathway, but also partly responsible for its less aggressive nature. Thus, in pancreatic neoplasia, MUC1 and MUC2 have potential diagnostic and prognostic value as markers of aggressive and indolent phenotypes, respectively, and have potential as therapeutic targets.
- EGFR, epidermal growth factor receptor
- IPMN, intraductal papillary mucinous neoplasia
- MAPK, mitogen activated protein kinase
- PanIN, pancreatic intraepithelial neoplasia
- TCF, T cell factor
- MUC1
- MUC2
- pancreatic cancer
- intraductal papillary mucinous neoplasm
- colloid carcinoma
Statistics from Altmetric.com
- EGFR, epidermal growth factor receptor
- IPMN, intraductal papillary mucinous neoplasia
- MAPK, mitogen activated protein kinase
- PanIN, pancreatic intraepithelial neoplasia
- TCF, T cell factor
MUCs are a heterogeneous group of glycoproteins with various roles both in homeostasis and carcinogenesis. MUC1, also referred to as mammary-type mucin, has a role in the maintenance of the lumina of ductal epithelial cells, and is thought to have an inhibitory role in cell–cell and cell–stroma interactions and in cytotoxic immunity. It also appears to function as a signal transducer, closely interacting with the epidermal growth factor receptor (EGFR) family, and participating in the progression of carcinogenesis.
“Both MUC1 and MUC2 seem to have important roles in pancreatic neoplasia”
In contrast, MUC2 is referred to as intestinal-type mucin because its expression is normally limited to goblet cells, where it contributes to the protective barrier function of these cells. Recently, MUC2 has been shown to have tumour suppressor activity, as demonstrated by the neoplastic transformation seen in the gastrointestinal system of MUC2 knockout mice. Both MUC1 and MUC2 seem to have important roles in pancreatic neoplasia. MUC1 appears to be a marker of aggressive phenotype. It is commonly expressed in high grade but not low grade pancreatic intraepithelial neoplasia (PanIN; microscopic/incidental precursors of invasive carcinoma). Furthermore, it is abundant in almost all examples of conventional ductal adenocarcinoma. In fact, dense cytoplasmic immunostaining for MUC1 can be used as a diagnostic tool, because such staining is not usually seen in normal or preinvasive neoplasia or other carcinoma types in this region. This may also be helpful in the subclassification of ampullary neoplasia. It is also possible that MUC1 facilitates the vascular spread of carcinoma cells by helping them to remain detached from the endothelial cells.
In sharp contrast to MUC1, MUC2 is almost never detectable in PanINs or conventional adenocarcinomas, but instead, it is commonly expressed in a rare but distinctive set of tumours that appear to form a distinct and indolent pathway of carcinogenesis. These are intraductal papillary mucinous neoplasms (IPMNs), characterised by clinically detectable papillary tumours that grow within and lead to pronounced cystic dilatation of the ducts (mass forming preinvasive neoplasia). MUC2 is expressed consistently in the intestinal subset of IPMNs, which is morphologically similar to villous adenoma. MUC2 is also uniformly present in colloid carcinoma, an indolent form of invasive carcinoma, which often arises in association with IPMN. MUC2 may not only be a marker of this indolent pathway, but may also partly be responsible for its less aggressive nature. It is speculated that MUC2, also known as gel forming mucin, may be a key factor in the slow growth of colloid carcinoma cells by forming a protective gel around the neoplastic cells, and therefore leading to the characteristic “cells floating in abundant mucin” morphology, and also limiting the spread of the cells.
Thus, in pancreatic neoplasia, MUC1 and MUC2 may have diagnostic and prognostic value as markers (and possible instigators) of the aggressive and indolent phenotypes, respectively, and may have potential as therapeutic targets.
MUC1 AND MUC2: BIOCHEMICAL AND PHYSIOLOGICAL PROPERTIES
Mucins are the major components of mucous, the visco-elastic substance that protects and lubricates epithelial mucosa, including that of the gastrointestinal tract. They are highly glycosylated molecules; up to 80% of their mass consists of O-linked glycosyl residues.1,2 Mucins constitute an expanding family of proteins that can be grouped into “transmembrane mucins” and “secretory mucins”.3 So far, 19 different mucin apoproteins have been identified.3–6 The transmembrane mucins are emerging as signal transducer proteins that regulate the growth, adhesion, and motility of cells.2,5,7
The best studied transmembrane mucin is MUC1, also known as epithelial membrane antigen, which was first identified in human milk.2 MUC1 is synthesised as a single polypeptide that undergoes proteolytic cleavage, creating a heterodimer that remains associated during its post-translational processing in the Golgi. The larger component contains most of the extracellular domain—the tandem repeat domain—which comprises 30–90 repeat sequences of 20 amino acids. Approximately 50–90% of the mass of MUC1 results from the O-glycosylation that occurs on the amino acid repeat units. The smaller component of the heterodimer consists of an extracellular stem that joins the larger component to the transmembrane domain and a 72 amino acid cytoplasmic tail, which has signal transduction properties as a result of the presence of docking sites for SH2 domain containing proteins, in addition to the presence of tyrosine phosphorylation sites.8–10
MUC1 is expressed by almost all human glandular epithelial tissues and throughout all regions of the gastrointestinal tract.2,7,11,12 MUC1 is also expressed in normal pancreatic intralobular ducts, together with MUC5AC, MUC5B, and MUC6.7,13–17 One major role of the MUC1 protein is to act as an anti-adhesive protein to maintain the luminal integrity of the lining epithelium.5,8 Therefore, in normal epithelia its expression is largely limited to the apical membrane of the cells.
In contrast, MUC2 is a secreted form of mucin, which is exclusively expressed in the goblet cells lining the gastrointestinal mucosa. MUC2 is characterised by tandem and irregular repeat sequences rich in threonine and serine, which are sites of attachment of the oligosaccharide chains. The MUC2 gene product is more than 5100 amino acids long in its most common allelic form, which accounts for one fifth of the mucin glycoprotein molecule by weight. The MUC2 protein is polymerised end to end through disulfide bridges to form large secreted polymeric gel forming mucins. It acts as a protective barrier at mucosal surfaces.18–20 It is also expressed in areas of intestinal metaplasia, such as those seen in Barrett’s oesophagus and long standing Helicobacter pylori gastritis.21–23 MUC2 is not expressed in the normal pancreas.24
MUC1 AND MUC2: THEIR POSSIBLE ROLES IN MOLECULAR CARCINOGENESIS
MUC1 is a signal transducer molecule, which can sense environmental changes and transduce messages into the cell. It is normally expressed on the apical borders of secretory epithelial cells. However, in tumour cells, MUC1 expression loses its polarity, being expressed throughout the entire cell surface.2,5,25 The presence of extracellular, transmembrane, and cytoplasmic domains makes it an ideal candidate as a signal transduction unit.2,5,8,10,25–27
MUC1 has been shown to be associated with the epidermal growth factor receptor (EGFR) members EGFR, ErbB2 (HER2/neu), ErbB3, and ErbB4 receptor tyrosine kinases through its cytoplasmic tail.9,10,27–29 In addition, binding of Grb2/sos and c-src to the cytoplasmic tail of MUC1 has been demonstrated.27 These findings suggest that the Ras–Raf–mitogen activated protein kinase (MAPK) signalling system can be triggered by MUC1. The importance and the context of these interactions are not completely clear. It is tempting to speculate that the extracellular domain of the MUC1 protein can sense some distinct changes in the extracellular environment, such as adhesion status or chemical composition of the milieu (for example, the presence of oxygen radicals).8
In addition to binding to EGFR family members, MUC1 can physically interact with β catenin, a key molecule of the Wnt signalling pathway, and also a key molecule in colorectal tumorigenesis.9,10,26,29,30 β Catenin is normally bound to cadherins, which regulate cell to cell adhesion. Upon activation of the Wnt pathway, β catenin translocates to the nucleus, binding the lymphoid enhancer 1/T cell factor (TCF) complex, thereby initiating the transcription of growth promoting genes.10,18,28–30 MUC1 is associated with increased nuclear localisation of β catenin. In fact, Wen et al recently demonstrated the translocation of the cytoplasmic tail of MUC1 to the nucleus in conjunction with β catenin.31 These findings suggest that, overall, MUC1 is associated with the detachment of β catenin from the cadherins and its translocation to the nucleus. This translates into loss of adhesion, and perhaps contact inhibition, and increased proliferation.
“In addition to binding to epidermal growth factor receptor family members, MUC1 can physically interact with β catenin, a key molecule of the Wnt signalling pathway, and also a key molecule in colorectal tumorigenesis”
The association of MUC1 with the cadherin–catenin–TCF and EGFR–Raf–Ras–MAPK, signalling pathways, two important transduction modules that regulate cell proliferation and diverse functions, strongly suggests that MUC1 has an active and functional role in carcinogenesis in a variety of tissues. MUC1 is overexpressed and differentially glycosylated by many tumours. There are several studies demonstrating the adverse prognostic effect of MUC1 expression on survival in various tumours, including those of the stomach, breast, kidney, colon, endometrium, lung, bile duct, and even lymphomas.32–44 In a recent study, MUC1 tandem repeats of the extracellular portion and the cytoplasmic tail were shown to be responsible for the invasive properties of a pancreatic carcinoma cell line.45
In contrast to MUC1, MUC2 has no transmembrane domain or signal transduction properties. Recently, there has been increased interest in the MUC2 protein as the result of the demonstration that MUC2 knockout mice develop colorectal tumours, including tubular and villous adenomas and invasive carcinomas.46 This finding indicates that MUC2 has tumour suppressor properties.
The expression of MUC2 is regulated by homeobox genes CDX1 and CDX2.47–49 These transcription factors are key in understanding normal intestinal development and the intestinal metaplasia that is often seen in H pylori gastritis, Barrett’s oesophagus, and cholecystitis.50–53 In fact, it has been shown that intestinal metaplasia of the stomach is always preceded by activation of the transcription factor CDX2.48 CDX2 expression also precedes the expression of MUC2 in Barrett’s epithelium.53 In a recent study by Seno et al, CDX2 expression in gastric cancer was associated with intestinal-type gastric cancer, a lower proliferation rate, and better survival compared with non-expressors.50 By binding to enhancer sequences in the promoter regions of target genes, CDX2 triggers the transcription of genes that encode intestine specific proteins, such as MUC2, sucrase/isomaltase, lactase, villin, KLF4, and carbonic anhydrase I. CDX2 also upregulates its own expression. Another way that CDX2 promotes intestinal differentiation is by upregulating the expression of WAF1/p21, causing cell cycle arrest.54 Overall, CDX2 seems to promote the differentiation and maintenance of intestinal epithelial cells.54
MUC2 expression is also regulated by p53.55 The MUC2 gene has been shown to have p53 binding sites.55 In cellular stress conditions, p53 is activated to control cell proliferation and allow DNA repair.56 It also triggers apoptosis when the repair efforts have been futile.56 The fact that p53 triggers MUC2 expression suggests that MUC2 is part of a stress response programme.55 Because MUC2 is part of the intestinal metaplasia programme, which itself is a response to stress conditions in gastric, oesophageal, and biliary mucosa, MUC2 expression may not be an oncogenic event per se, but a protective mechanism, which is activated to prevent further exposure to carcinogens.54 However, overall, the development of intestinal metaplasia in the stomach and oesophagus is associated with an increased risk of cancer.54,57,58
Whereas mucin secretion and MUC2 expression are part of the many stress responses in airway epithelia, stomach, and biliary tract, conversely, loss of MUC2 expression is a frequent feature of colorectal cancer.46,59–61 In fact, during colorectal cancer progression, loss of mucin and MUC2 expression are seen frequently, and are followed by overexpression of MUC1.60,62,63
In many tissues, loss of MUC2 gene activation has been attributed to receptor methylation.24,59,64,65 Siedow et al have studied the mechanism of MUC2 expression in pancreatic carcinoma cell lines. They have shown that in non-expressor cell lines the MUC2 gene is methylated, whereas in the expressors it is demethylated. The investigators also treated non-expressor cell lines with demethylating agents, such as 5-aza-2-deoxycytidine, which caused expression of MUC2 in non-expressors.24 Demethylating agents may be useful as potential therapeutic agents in treating aggressive adenocarcinomas.
MUC1 AND MUC2 EXPRESSION IN NORMAL ADULT PANCREAS
In the normal adult pancreas, MUC1 expression is confined to the apical membrane of intralobular ductules, possibly a manifestation of the “lumen maintenance” role of MUC1. MUC1 expression is not detected in larger ducts or other pancreatic elements (islets or acini).66,67 It should be noted here that, in our opinion, it is these intralobular ductules that pancreatic ductal adenocarcinoma resembles most closely, both in its histochemical properties and its immunophenotype.
MUC1 AND MUC2 IN PREINVASIVE NEOPLASIA OF THE PANCREAS
Pancreatic intraepithelial neoplasia
-
MUC1: expressed in some PanIN-3 tumours only
-
MUC2: virtually absent
PanIN is the term adopted recently for the microscopic/incidental form of intraductal proliferations that have been long suspected to be the precursors of invasive ductal adenocarcinoma.68 These proliferations have been previously classified under various names ranging from metaplasia (for the early forms) to hyperplasia (with or without atypia) to dysplasia.69–71 According to the scheme proposed recently, these lesions are unified under the term PanIN (to conform with the terminology used in other organs, such as the prostate), and classified into three grades: PanIN-1 includes but is not limited to changes previously regarded as mucinous metaplasia (but which were recently found to harbour several molecular alterations associated with neoplasia), and at the other end of the spectrum, PanIN-3, which includes carcinoma in situ.68
MUC1 is expressed in a substantial number of PanIN-3 tumours but is almost absent in PanIN-1 or PanIN-2 (fig 1C). In contrast, MUC2 is not detected in PanINs.66
{kind=link}
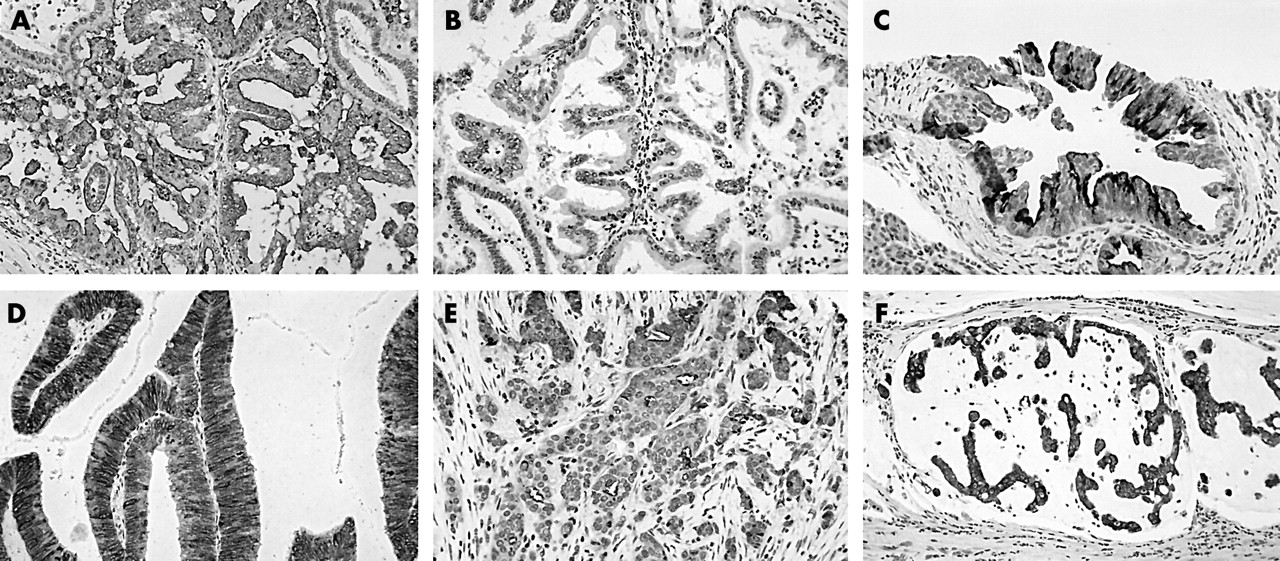
MUC1 and MUC2 staining of different entities. (A) MUC1 staining of an intraductal papillary mucinous neoplasm (IPMN), pancreatobiliary type; original magnification, ×100). (B) Lack of MUC2 staining of the same lesion; original magnification, ×100. (C) MUC1 staining of a grade 3 pancreatic intraepithelial neoplasia lesion; original magnification, ×100. (D) MUC2 staining of a villous intestinal-type IPMN; original magnification, ×200. (E) MUC1 staining of a ductal-type pancreatic adenocarcinoma; original magnification, ×100. (F) MUC2 staining of a colloid carcinoma of the pancreas; original magnification, ×100.
Intraductal papillary mucinous neoplasia
-
MUC1: rarely expressed
-
MUC2: very frequently expressed
IPMN is now a well recognised category in the pancreas, unifying tumours that are characterised by intraductal proliferation of neoplastic mucinous cells, which often form papillae, and lead to cystic dilatation of the pancreatic ducts, forming clinically and macroscopically detectable masses.72–79 These tumours have previously been reported under a variety of names, such as villous adenoma, intraductal papillary tumour, mucin producing tumour, mucinous duct ectasia, etc.80–83 IPMN should be distinguished from the more widely recognised mucinous cystic neoplasms (see below).84–86
Similar to PanINs, IPMNs are regarded as a form of preinvasive neoplasia, acting as a precursor and maybe as even a marker of invasive carcinoma.87–89 Both PanINs and IPMNs are intraductal lesions with papilla forming mucinous cells; however, in the case of IPMNs, the proliferation progresses to form large (clinically and grossly detectable) cystic or papillary masses, whereas PanINs are noted only as incidental findings.66,90 We think that this dichotomy represents two relatively distinct pathways of carcinogenesis, although there are some overlaps, as would be expected. This dichotomy is similar to that seen in other organs, such as: (1) in the urothelium, as flat versus papillary transitional cell carcinomas; or (2) in the breast, as intracystic papillary carcinoma versus ordinary intraductal proliferations; these are distinct pathways not only clinically and morphologically, but also biologically and at the molecular level.91–94
“MUC expression patterns not only support the dichotomy between pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasia (IPMN) but also confirm the existence of morphological subtypes in IPMN”
MUC1 and MUC2 expression patterns in IPMNs versus PanINs support this dichotomy. Whereas MUC2 expression is almost absent in PanINs, it is present in a substantial number of IPMNs.66 In particular, MUC2 expression is uniformly diffuse and strong in the most common subtype of IPMN (fig 1C), which is described as villous/intestinal type or compact cell type, and is characterised by finger-like papillary projections that are lined by columnar cells with cigar shaped nuclei, and is morphologically very similar to colonic villous adenomas. In contrast, MUC1, which is often present in PanIN-3, is much less frequently expressed in IPMNs.33,66 More interestingly, those IPMNs that express MUC1 are invariably of the rare subtype that we have been independently referring to as pancreatobiliary, and which is characterised by more complex (arborising) papillae and cuboidal cells, similar to those seen in biliary papillomatosis (fig 1A, B). This differential expression of MUC1 and MUC2 in the subtypes of IPMN has been noted by various investigators, including Luttges et al,95,96 Kloppel et al,97 and Yonezawa et al,33 who refer to these subtypes as dark cell, clear cell, and compact cell types. Because MUC2 is also referred to as intestinal type mucin and regarded as a marker of goblet cells, its consistent expression in the intestinal subtype of IPMN can be taken as further evidence of intestinal differentiation. In other words, MUC expression patterns not only support the dichotomy between PanINs and IPMNs but also confirm the existence of morphological subtypes in IPMNs.
Intraductal oncocytic papillary neoplasia (IOPN)
-
MUC1: expressed (data limited)
-
MUC2: expressed (data limited)
Oncocytic papillary tumours are characterised by mucin filled cysts containing nodular papillary projections. Dilated ducts communicating with the main tumour can also be seen. Microscopically, the cystic structures correspond to dilated ducts containing intraductal tumour. The tumours are characterised by variably complex, arborising papillary structures. The papillae have thin, delicate fibrovascular cores with focal myxoid changes, and are lined by stratified oncocytic cells. Goblet cells and intraepithelial mucin containing lumina are also present, with these last structures resulting in a characteristic cribriform pattern. The extent of epithelial proliferation varies from case to case and between different regions within individual tumours; solid sheets of cells can often be identified.73 Intraductal oncocytic papillary neoplasms have been studied for their mucin expression patterns and they were found to express both MUC1 and MUC2 by Luttges et al.95 However, Terris et al reported that oncocytic papillary neoplasms lacked MUC2 expression.16 Because they are rarely encountered, there is still a need for further work on these tumours.
Mucinous cystic neoplasms
-
MUC1: rarely expressed
-
MUC2: present only in goblet cells; no diffuse labelling
Mucinous cystic neoplasms are seen typically in perimenapausal women (> 95% women; mean age, 50 years) and present as multilocular, thick walled cysts in the tail of the pancreas. Ovarian-like stroma is invariably present.85,97 Luttges et al have studied the mucin expression profiles of mucinous cystic neoplasms comprising adenomas, borderline lesions, and carcinomas. They found that MUC1 is not expressed in non-invasive lesions of mucinous cystic neoplasms, but is a marker of invasion.67 MUC2 expression was seen in the interspersed goblet cells. There was no diffuse staining of the lining epithelium. They found that mucinous cystic neoplasms invariably expressed MUC5AC, which is also commonly expressed in ordinary ductal carcinoma.
MUC1 AND MUC2 IN INVASIVE CARCINOMAS OF THE PANCREAS
Conventional ductal adenocarcinomas
-
MUC1: uniform and strong expression; apical membraneous in tubule forming areas; intracytoplasmic in the poorly differentiated areas
-
MUC2: virtually absent
MUC1 is expressed in almost all examples of ordinary ductal (pancreatobiliary) adenocarcinomas of the pancreas, which are characterised by infiltrating small tubular units embedded in desmoplastic stroma. Expression is predominantly confined to the luminal membrane in the duct forming areas, whereas it is also intracytoplasmic in the poorly differentiated areas (fig 1E).12,13,45,66,98 MUC2 expression has been very rarely reported in ordinary ductal carcinomas of the pancreas.66
Colloid carcinomas
-
MUC1: rarely expressed
-
MUC2: very frequently expressed
Colloid carcinoma of the pancreas was recently described as a distinct entity and was distinguished from signet ring cell carcinomas, ordinary ductal carcinomas, and mucinous cystadenocarcinomas.99,100 Like their counterparts in the breast, colloid carcinomas of the pancreas have a much better prognosis than regular adenocarcinomas, with a five year survival of 55% compared with 10% for ordinary ductal carcinomas.99 MUC2 expression is a hallmark of colloid carcinomas of the pancreas (fig 1F). We recently examined the ultrastructural properties of colloid carcinomas and showed that mucin secretion was towards the stroma facing surface of the cells and that extracellular mucin pools formed a barrier between the tumour cells and the stroma. This altered polarity of mucin secretion may be a contributing factor to the indolent behaviour of colloid carcinomas.100
Take home messages
-
MUC1 versus MUC2 staining correlates with the morphological subtypes of intraductal papillary mucinous neoplasia (IPMN) and can predict prognosis because MUC1 expression is more often associated with pancreatobiliary-type IPMN and ductal adenocarcinoma
-
If a papillary lesion has diffuse MUC2 positivity (not limited to goblet cells) it is probably an intestinal subtype of IPMN, whereas if an invasive carcinoma is positive for MUC2 staining, it is very likely to have at least a colloid carcinoma component
-
MUC1 is a marker of an aggressive phenotype in pancreatic intraepithelial neoplasia (PanIN): it is expressed only in PanIN grade 3 lesions and is a harbinger of invasive carcinoma
-
In ampullary carcinomas, MUC1 versus MUC2 staining can help to determine the origin of the lesion: diffuse intracytoplasmic staining for MUC1 is indicative of pancreatobiliary-type carcinoma, whereas MUC2 staining favours the intestinal type
MUC1 AND MUC2 IN AMPULLARY NEOPLASIA
-
MUC1: frequently expressed in pancreatobiliary type, rarely expressed in intestinal type
-
MUC2: commonly expressed in intestinal type (low sensitivity), rarely expressed in pancreatobiliary type
Ampullary carcinomas can arise from the intestinal or the pancreatobiliary epithelium. Determining the origin of adenocarcinomas arising in the papillary region is important because intestinal-type carcinomas behave like colonic adenocarcinomas, whereas pancreatobiliary types behave more like pancreatic adenocarcinomas. MUC1 and MUC2 immunostaining can be helpful in determining the origin of the carcinoma, particularly when tumour histomorphology is not discriminatory, because cases with mixed patterns are frequently encountered.101,102 In an unpublished study, we have shown that MUC1 is frequently expressed in the pancreatobiliary type, whereas MUC2 is absent. In contrast, the intestinal type lacks MUC1 expression, whereas almost half of these tumours express MUC2. In other words, our preliminary unpublished data suggest that MUC1 and MUC2 are very specific in differentiating intestinal from pancreatobiliary types, whereas the sensitivity of MUC2 expression is low. In our experience, patients with ampullary carcinomas that are MUC1+/MUC2− have a shorter survival than patients whose tumours are MUC1−/MUC2+.101,102
REFERENCES
Linked Articles
- Corrections