Article Text

Abstract
Aims: A review of the literature indicated that only one case of serrated adenoma of the appendix has been recorded. The aim was to explore the possible occurrence of serrated adenomas of the appendix at the department of pathology, Karolinska Institute and University Hospital, Stockholm, Sweden.
Methods: Between January 1993 and December 2003, 38 non-carcinoid, non-neoplastic, or neoplastic polyps or tumours of the appendix were surgically removed at this hospital. All filed histological sections (haematoxylin and eosin stained) were reviewed.
Results: Of the 38 lesions, four were hyperplastic polyps, 10 serrated adenomas, six villous adenomas, and the remaining eight mucinous adenocarcinomas without a remnant adenoma. Serrated adenomas accounted for six of the 11 adenomas without invasion, and four of the 15 adenomas with invasive carcinoma. At the time of surgical resection, four of the 10 serrated adenomas had evolved into invasive carcinomas, in addition to 11 of the 16 villous adenomas.
Conclusions: Serrated and villous adenomas of the appendix appear to be highly aggressive lesions, more aggressive than similar adenomas in the colon and rectum. Of the seven cases with a hyperplastic polyp, one concurred with a serrated adenoma, two with a serrated adenoma having an invasive carcinoma, and one with invasive carcinoma without a remnant adenomatous structure. At present, there is an increased awareness that some hyperplastic polyps of the colon and rectum may evolve into serrated adenomas. Whether this pathway is also valid for the appendix vermiformis should be investigated in a larger number of cases.
- serrated
- adenomas
- appendix
Statistics from Altmetric.com
It is generally accepted that adenocarcinomas of the appendix are preceded by an adenomatous growth. Fenoglio-Preiser1 classified adenomas of the appendix into mucinous cystoadenomas, mixed hyperplastic villous adenomas, and serrated adenomas. According to that author,1 serrated adenomas are found more often in the right colon and the appendix. Williams divided benign tumours of the appendix into adenomas, hyperplasias, and mixed adenoma/hyperplasia (serrated adenomas).2 More recently Carr et al postulated that the precursor lesion in tumours of the appendix is probably a villous or a serrated adenoma.3 It should be stressed that all these descriptions emanated from textbooks and that the number of serrated adenomas of the appendix found was not given.
“The aim of our present investigation was to explore the possible occurrence of serrated adenomas of the appendix at this department”
For the purpose of this work, we searched the medical literature for published reports on cases of serrated adenoma of the appendix. Longacre and Fenoglio-Preiser4 reported 110 cases of mixed hyperplastic adenomatous polyp of the colon and rectum. The localisation of 12 of those 110 cases was the “caecum/appendix”.4 Unfortunately, the number of lesions localised exclusively to the appendix was not specified. Williams and Whitehead5 reported 33 non-carcinoid epithelial tumours of the appendix and found two lesions containing mixed adenoma/hyperplasia. The illustrations accompanying those cases showed that the configuration of the dysplastic component was tubular and not serrated.5 In a subsequent publication by Williams et al,6 reviewing 42 benign epithelial neoplasms of the appendix, no cases of serrated adenoma were reported. Carr et al classified benign tumours of the appendix into simple mucocele, hyperplastic polyp, and adenoma.7 Adenomas were subclassified into tubular, mucinous, or cystoadenomas, and lesions with both hyperplastic and adenomatous features. These authors found that of the 42 adenomas, one was a tubular adenoma, 16 were villous, and the remaining 25 had an undulating pattern of growth.7 The undulating pattern was not defined and the accompanying illustration shows absence of a serrated pattern.7 Thus, the adenomas with an undulating pattern reported by Carr et al were not serrated adenomas.7 Interestingly, Riddell et al wrote in a recent monography that “some appendiceal cystoadenomas demonstrate a more undulating architecture or mucosa typical of serrated adenoma (mixed adenoma/hyperplastic polyp)”.8 However, those authors8 were, in fact, referring to the work of Carr et al.7 Consequently, no case of serrated adenoma of the appendix was presented in that monography.8
The review of the literature revealed that only one case of serrated adenoma of the appendix has been recorded.9
The aim of our present investigation was to explore the possible occurrence of serrated adenomas of the appendix at this department. For that purpose, all non-carcinoid benign and neoplastic growths of the appendix registered during a period of 11 years were retrieved and reviewed.
MATERIAL AND METHODS
Between January 1993 and December 2003, a total of 38 non-carcinoid non-neoplastic or neoplastic polyps or tumours of the appendix were surgically removed at this hospital. All filed histological sections (haematoxylin and eosin stained) were reviewed.
Definitions10
Hyperplastic (metaplastic) polyps
A focus of mucosal hyperplasia in which the crypts of Lieberkühn show a sawtooth configuration as a result of crenate epithelium. The cells are columnar with or without apical mucous vacuoles alternating with large goblet cells. The bases of the crypts are lined by regular cells with small, round nuclei.
Villous adenoma
An adenoma having ⩾ 80% of dysplastic epithelium arranged as straight villous fronds.
Serrated adenoma
An adenoma that has crenate, sawtooth-like structural changes in the dysplastic epithelium covering the basal aspect of the crypts of Lieberkühn, as a result of epithelial infolding. When serrated fronds are present in more than 50% of the dysplastic structures, the adenoma is classified as serrated adenoma. The remaining adenomatous tissue usually shows metaplastic or villous structures. Recently Bariol et al reported that the diagnosis of serrated adenomas of the colon and rectum should include lesions having serrated structures in ⩾ 20% of the dysplastic crypts.11 We have used a limit of more than 50%.10
RESULTS
The patients
Sex
Of the 38 patients, 21 were men and 17 were women.
Age
The mean age of the 38 patients was 55.7 years (range, 20–89).
Preoperative diagnosis
The preoperative diagnoses in the 38 patients were: acute appendicitis (n = 25), mucocele of the appendix (n = 2), caecal carcinoma (n = 2), endometriosis (n = 1), suspected metastasis in the caecum–appendix from a uterine carcinoma (n = 1), appendiceal and ovarial myxoma (n = 2), peritoneal carcinosis (n = 1), and myxoma peritonei (n = 4).
Histological examination
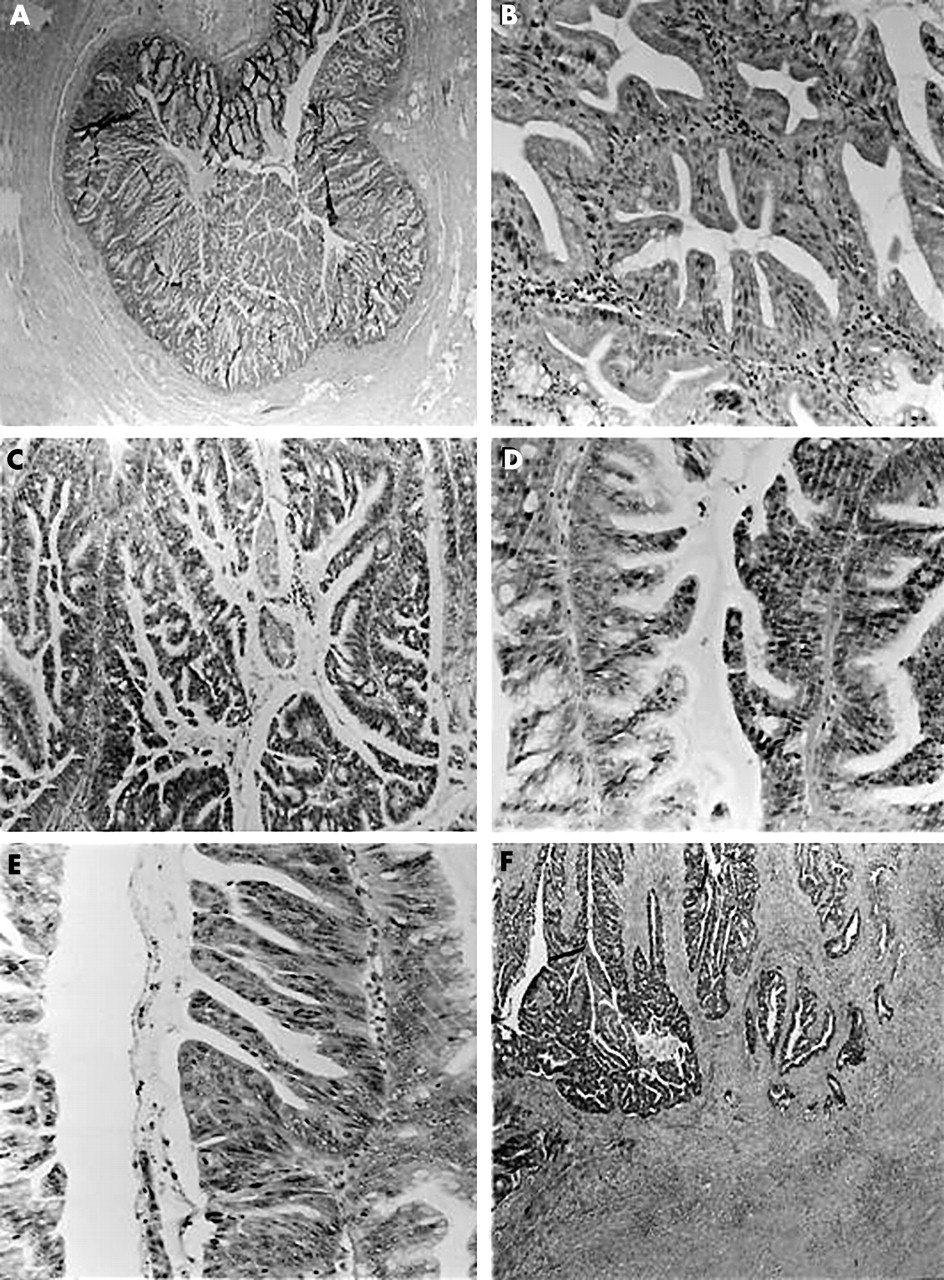
Table 1 shows that of the 38 lesions, four were hyperplastic polyps (fig 1A), 10 were serrated adenomas (fig 1B–F), 16 were villous adenomas, and the remaining eight were mucinous adenocarcinomas without a remnant adenoma.
Histological findings in 38 hyperplastic and neoplastic lesions of the appendix found in 4934 appendicectomy specimens received at the department of pathology, Karolinska University Hospital between 1993 and 2003

{kind=link}
(A) Low power view of a mixed hyperplastic polyp–serrated adenoma of the appendix (haematoxylin and eosin (H&E) stain; original magnification, ×5). (B) Detail from panel (A) showing an area with serrated indentations with low grade dysplasia (appendix; H&E stain; original magnification, ×50). (C) Serrated adenoma of the appendix showing serrated epithelial indentations with high grade dysplasia (H&E stain; original magnification, ×10). (D) High power view of panel (C) showing an area with serrated epithelial indentations with high grade dysplasia (right part of the picture). On the left half of the picture note the remnants of hyperplastic polyp with serrated configurations evolving into serrated adenoma with low grade dysplasia (H&E stain; original magnification, ×50). (E) Detail from a serrated adenoma of the appendix with high grade dysplasia (H&E stain; original magnification, ×50). (F) Invasive carcinoma of the appendix originating in a serrated adenoma (H&E stain; original magnification, ×10).
One of the six serrated adenomas without invasion had a hyperplastic polyp adjacent to the adenoma. Of the 10 serrated adenomas, four had an invasive carcinoma. Two of the four serrated adenomas with invasion also had a hyperplastic polyp adjacent to the adenoma, and in two an area of villous adenoma was found.
Of the 16 villous adenomas, 11 had an invasive carcinoma. None of the cases with a villous adenoma concurrently had a hyperplastic polyp. However, in one villous adenoma an area of serrated adenoma comprising 5% of the neoplasia was seen.
Table 1 shows that 15 of the 23 cases with invasive adenocarcinoma had a remnant adenoma. In one of those 15 cases, the remnant lesion was a hyperplastic polyp, in four a serrated adenoma, and in the remaining 11 a villous adenoma.
Age and histological subtypes
The mean age of the four patients with hyperplastic polyps of the appendix was 62 years. The mean age of the six patients with serrated adenomas without invasion was 46.8 years, and in the four with invasion it was 71.7 years. The mean age of the five patients who had villous adenomas without invasion was 47.4 years, and the mean age of the 11 patients with invasion was 59.7 years. Finally, the mean age of the eight patients who had invasive carcinoma of the appendix without remnant adenoma was 50.8 years.
DISCUSSION
A review of the 38 tumours of the appendix received at our department over a period of 11 years (1993–2002) showed that 10 were serrated adenomas with or without invasion. Five of these 10 cases were reported over a nine year period (between January 1993 and December 2001), whereas the other five occurred during just two years (2002 and 2003). Consequently, whereas only 0.6 cases/year of serrated adenoma of the appendix were recorded during the first period of nine years, as many as 2.5 cases/year were found during the years 2002 and 2003. In contrast, of the 16 patients with villous adenoma, 13 tumours were found during a nine year period (between January 1993 and December 2001) and the remaining three during two years (2002 and 2003). Accordingly, 1.4 cases/year of villous adenoma of the appendix were found during the first period of nine years, and 1.5 cases/year were found during 2002 and 2003. Because the number of apendicectomies varied between 1993–2001 and 2002–2003 and the numbers of observations were few in some of the groups, a statistical assessment was difficult. However, when comparing the first period of nine years to the last two years in this survey, the number of serrated adenomas/year had obviously increased, but not the number of villous adenomas/year.
Several possibilities were considered as explanations for the discrepancy in the frequency of serrated adenomas of the appendix between those two periods. One was that the technique of sectioning the appendix for histological evaluation had changed through the years, with more sections being available for histological evaluation during the years 2002 and 2003. However, this was not the case because the sectioning technique had remained unchanged during the entire period of this investigation. Another possibility was the increased awareness of serrated adenomas in later years. However, the present work was not based on archival reports but on the review of filed sections following strict histological criteria. A third possibility was that during 2002 and 2003 the number of appendices received had increased compared with 1993 to 2001. To investigate this possibility a search was carried out on our database. The retrieved data showed that between 1993 and 2001 a total of 3475 (or 346.1/year) appendices were received at this department, whereas during 2002 and 2003 a total of 1459 appendices (or 729.5/year) were booked in. Accordingly, the possibility that the increased number of serrated adenomas found during the years 2002 and 2003 was partly the result of a higher number of specimens available for histological evaluation could not be totally rejected. However, if this were the case, why were serrated adenomas of the appendix not being reported from other hospitals? There must be another rational explanation (at present elusive) for this chronological difference in frequency of serrated adenomas in our survey. The possibility that serrated adenomas of the appendix are becoming more frequent because of epigenetic factors modulated by changing local microenvironmental conditions conveyed by the diet appears unlikely.
Take home messages
-
A review of the 38 tumours of the appendix resected at the department of pathology, Karolinska Institute and University Hospital, Stockholm, Sweden over a period of 11 years (1993–2002) showed that serrated and villous adenomas of the appendix seem to be more aggressive lesions than their counterparts in the colon and the rectum
-
Of the seven cases with a hyperplastic polyp, one concurred with serrated adenoma, two concurred with serrated adenomas with an invasive carcinoma, and one concurred with invasive carcinoma without a remnant adenomatous structure
-
There is an increased awareness that some hyperplastic polyps of the colon and rectum may evolve into serrated adenomas and larger numbers of cases are needed to investigate whether this pathway is also valid for the appendix vermiformis
The results showed that serrated adenomas accounted for six of the 11 adenomas without invasion, and for four of the 15 adenomas with invasive carcinoma. At the time of surgical resection, four of the 10 serrated adenomas had evolved into invasive carcinomas, as had 11 of the 16 villous adenomas. Thus, villous and serrated adenomas of the appendix appear to be highly aggressive lesions, more aggressive than those found in the colon and the rectum. In this regard, Muto et al postulated that most colorectal adenomas do not become cancerous during a normal adult life span,12 and Williams and Bedenne13 calculated that fewer than 10% of colorectal adenomas evolve into invasive carcinoma. However, it should be born in mind that there are histofunctional differences between the mucosa of the colon and rectum and that of the appendix. In the appendix, most of the lumen is lined by specialised follicle associated epithelium. That specialised epithelium has—in contrast to the epithelium of the colorectal mucosa—few goblet cells and many of the columnar cells are of the M cell type (that is, membranous cells able to attract luminal antigens). In addition, the mucosa of the appendix contains neuroendocrine complexes (a collection of neuroendocrine ganglia interconnected with neural fibres) just beneath the crypts.14 Another important difference is that in the colon and rectum the most common adenoma phenotype is the tubular type,11,12 but this type of adenoma seems to be rare in the appendix; in our survey no case of tubular adenoma was recorded. Whether those histofunctional and obvious anatomical differences play a crucial role in the aggressive behaviour of villous and serrated adenomas of the appendix remains unclear.
Although the number of cases presented here is small, it is worth mentioning that there was a difference of 24.9 years (mean) between patients with serrated adenomas of the appendix without invasion and those with invasion. In contrast, the difference between patients with villous adenomas of the appendix without invasion and those with invasion was only 12.3 years (mean). These results suggest that in the appendix the invasive process has a more accelerated pace in villous adenomas than in serrated adenomas.
“There are histofunctional differences between the mucosa of the colon and rectum and that of the appendix”
Of the seven patients with hyperplastic polyps, one concurred with a serrated adenoma, two with a serrated adenoma having an invasive carcinoma, and one with invasive carcinoma without a remnant adenomatous structure. At present, there is an increased awareness that some hyperplastic polyps of the colon and rectum may evolve into serrated adenomas.4,11,15 Whether this pathway is also valid for the appendix vermiformis should be investigated in a larger number of cases.