Article Text

Abstract
Although guidance exists for the use of many laboratory tests in a wide range of clinical situations, this guidance is spread among a range of literature sources, and is often directed at laboratory specialists rather than test users. Individual general practices display large variations in standardised test requesting, yet much of their testing activity involves a relatively small range of tests. This paper describes a methodological approach to review the available evidence and guidance and to extract relevant primary research work to examine a range of testing scenarios in general practice, with the aim of formulating guidance based on the best available evidence or consensus opinions.
- appropriateness
- best practice
- evidence based pathology
- multidisciplinary
Statistics from Altmetric.com
Best practice use of pathology has again become prominent across the medical press,1–4 variously appearing under the headings of best practice, appropriateness, and demand control. There is little dispute that pathology tests are not optimally used, and that tests are often used unnecessarily, although the absolute amount of overuse is not known.5,6 Inappropriate tests may also have important adverse consequences for patients.7 Conversely, with the increasing transfer of the management of chronic disease into primary care, underuse of appropriate tests may compromise good patient management.
It is unlikely that laboratory medicine will ever have the extent of evidence base with which our more clinical colleagues are endowed. Indeed, it has recently been suggested that the discipline of evidence based pathology may not exist,8 although the same author reminds us that this must not be a reason for not addressing the difficult question of the appropriate use of laboratory tests.
“There is little dispute that pathology tests are not optimally used, and that tests are often used unnecessarily, although the absolute amount of overuse is not known”
Primary care accounts for 50% or more of laboratory activity in many district hospitals, although locally 95% of this activity concerns only 28 test types.9 Given the large differences in test submission rates between general practices, and the clinical governance structures that have been established within primary care trusts, this is an opportune time to examine the use of pathology testing in primary care.
Although the evidence base behind much laboratory testing is limited, there is a wealth of guidance, consensus documents, national policy statements, and related documents that have sought to provide guidance based on extrapolation from evidence based reviews and clinical trails. However, these are distributed throughout medical and government literature and are not readily available to the general practitioner, or indeed to many laboratory medicine specialists. Work reviewing the field of preoperative laboratory testing has recently been published by the National Institute for Clinical Excellence,10 and represents an important start in this process.
To benefit from the advances in information technology that allow information about good practice to be disseminated more easily there is a need for ready access to up to date guidance on the optimal use of laboratory tests, which can be used to inform interventions by the laboratory medicine specialist or general practitioner. These can involve prompting in electronic requesting, educational facilities, laboratory based prompts and investigation strategies, or interactive debate between laboratory medicine specialists and general practitioners. The same information can also be of potential benefit in empowering patients, offering them accurate information on tests and helping them to participate more in their own management, in addition to dispelling unrealistic expectations of testing. Although guidance alone is not an effective means of effecting change,11 knowledge of the existing knowledge base is a prerequisite for any intervention designed to improve practice.
BEST PRACTICE GROUP
It was this background that led to the formation last year of a cross discipline group containing representation from the Associations of Clinical Pathologists, PRODIGY (www.prodigy.co.uk),12 the Royal College of General Practitioners, the Royal College of Pathologists, the Association of Clinical Biochemists, the Association of Medical Microbiologists, and the British Society for Haematology, supported by a patient representative from the lay committee of the Royal College of Pathologists. The aim of the group is to examine the evidence for producing best practice guidance in the primary care use of laboratory testing.
The 14 members are from the disciplines of general practice, information science, biochemistry, haematology, microbiology, and immunology. In microbiology the group is working with the Health Protection Agency primary care unit, the head of which is a group member. A list of the group members is shown as supplementary data online (http://www.jclinpath.com/supplemental). We would be happy to hear from colleagues who would be willing to contribute to the writing of answers in their particular field of interest.
TERMS OF REFERENCE
The overall aim of the group is to improve the clinical quality of laboratory pathology requesting in primary care. The first objectives of the group will be to identify existing best practice evidence and guidance, identify areas needing research, and produce consensus guidance on best test use. To do this, the initial aims are:
-
To establish a common methodology for conducting literature searches on a range of primary care pathology questions specifically in biochemistry, haematology, and microbiology.
-
To construct a list of “common questions” that arise in primary care (fig 1).
-
To invite suitably experienced people to prepare brief reviews, ideally of no more than one page each, to answer the question.
-
To link with individual discipline professional bodies, the Royal College of General Practitioners, the Royal College of Pathologists, and other organisations with specific interests in the subject (such as Diabetes UK and the British Thyroid Foundation) for approval of answer content.
-
To liaise with the journal editors to arrange for suitable peer review of the reviews before publishing, either individually or as a series of reviews.
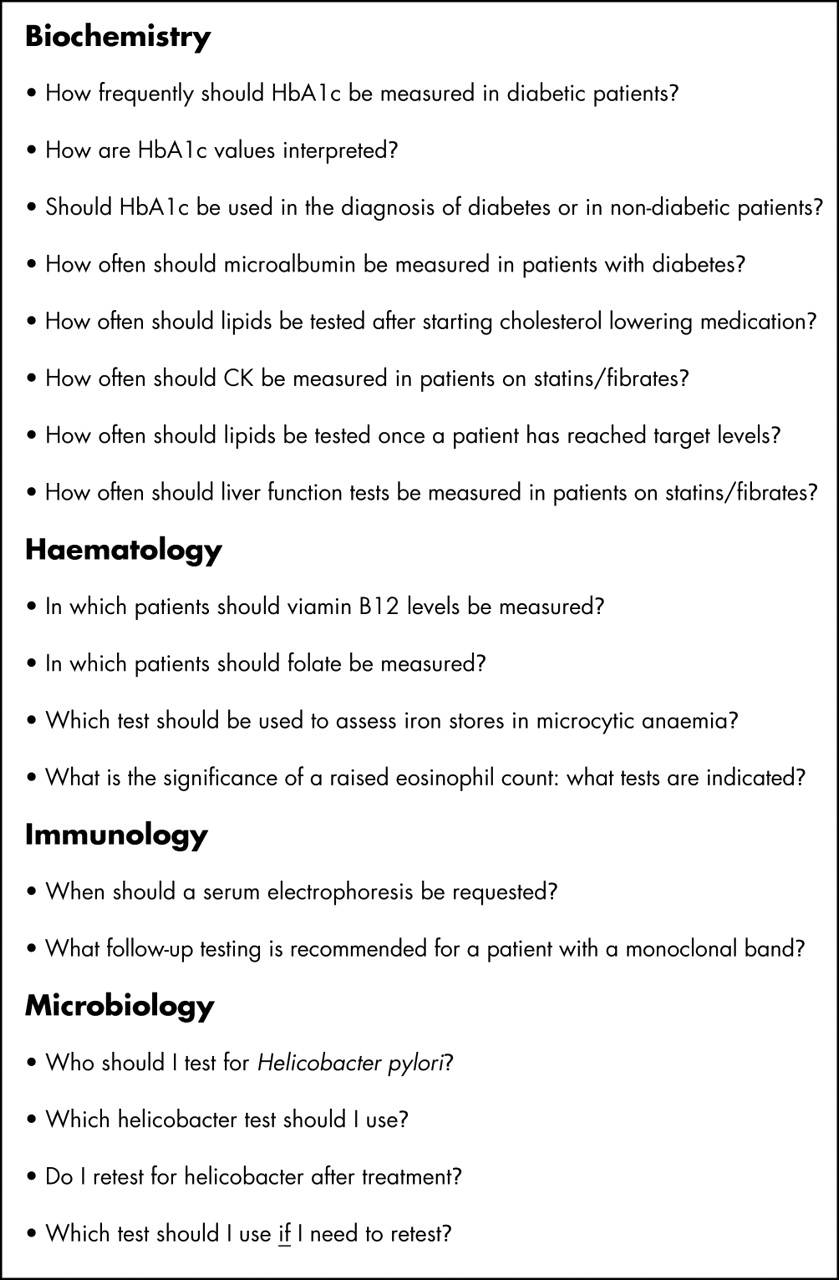
Sample questions. An initial series of 86 questions was expanded and refined after distribution to general practitioners to produce the final draft list of 103 questions to form the basis of the literature searches.
METHODS
It is envisaged that the data collection phase will last for two years, subject to funding, and we aim to publish guidance as it is produced and, in parallel, examine possible means of dissemination/implementation.
COORDINATION
A coordinator in each discipline will liaise with authors, currently two or three for each answer set (fig 2), and questions will be grouped into common themes. Each author group has taken on a two to three question set, with a remit of producing a brief answer, based on the results of the standardised literature search. Two phases of question refinement are carried out with the purpose of (1) making the clinical questions as specific as possible, and (2) making the questions as suitable as possible for the literature search (both the authors and an information scientist are involved in this refinement). There are therefore two stages of consensus agreement to be reached, one for the question content and one for the answer content. Because the number of group members involved in deriving the consensus was small in each case (author pair or trio, coordinator, and information scientist) and the aim of the authors was to interact directly to summarise existing published guidelines, rather than formulate new ones, we did not attempt to adopt the more formalised structured group processes such as “Delphi”13 or “nominal group”,14 but used an approach closer to that described by Glaser15 (“state of the art approach”), which appears better suited to our aims. Therefore, the group was formed initially around necessary support from relevant professional organisations, with several members being approached by the group chair, and additional authors were recruited either from individual group members’ knowledge of their involvement in a particular area of laboratory medicine, or were recommended on a similar basis by the professional organisations. Because questions were centred around issues specific to the “everyday” practice of primary care medicine we did not seek, necessarily, to recruit leading national experts on individual subjects, but practitioners (consultants or general practitioners) with interests in the specific subject matter of the question, or in the wider issues of the appropriate use of testing. This was in keeping with a tenant of Lundberg16 on methods of changing test requesting behaviour, whereby those involved need not be service heads, but rather those closer to the usual practice of the issue in question. Direct email, telephone, and occasional face to face contacts (where practicable) between authors, coordinator, and information scientist were used to distribute and return successive question and answer drafts until the group involved reached agreement on its final content. Email greatly facilitates the dialogue process and helps to focus the question being addressed and to avoid the digression that can occur in a face to face environment, although after the initial pilot study the group is forming a web based forum to facilitate dialogue further using the PRODIGY web site (http://www.PRODIGY.nhs.uk).

Sample question/answer set. Following the search strategy described, several guidelines and consensus documents were identified and reviewed to produce the short guidance and background information shown. ALT, alanine aminotransferase; AST, aspartate aminotransferase.
PILOT PHASE
A pilot phase lasting up to six months is currently under way with the aim of testing methodology in answering a series of 18 questions across the disciplines. A total of 86 questions were constructed initially by group members, and then put to general practitioners in the South Durham, Luton, and Dunstable areas for consultation. Additional questions and modifications to original questions were incorporated in a final draft list of 103 questions (fig 1). At this stage, histopathology questions have not been included because guidance on the management of skin malignancy is currently being prepared by the National Institute for Clinical Excellence.17 The questions relate to indications for testing, follow on and disease monitoring tests, and the interpretation of abnormal results.
PILOT SEARCH STRATEGY
To answer everyday primary care questions we need to combine consensus views with evidence based statements and qualify where necessary with pragmatic advice. Therefore, the search strategy avoids primary research, except where recent landmark works have been published but not yet incorporated into guidance documents.
This draft search strategy attempts to achieve this and provides a worked example, based on strategies used successfully by PRODIGY in constructing their existing guidance.
BACKGROUND ASSUMPTIONS FOR SEARCH STRATEGY
-
It is not feasible for the group to carry out 100 systematic reviews in a time frame compatible with producing up to date guidance on all subjects.
-
The evidence base is poor for many diagnostic and monitoring procedures.
-
There are few systematic reviews of diagnostic tests and the method for doing these is less well established.
-
Questions need to be focused and unambiguous.
-
The search strategy must be flexible (for example, diagnostic testing versus frequency of test monitoring).
-
Indexing may be imperfect in some bibliographical databases.
-
For consistency, searches should be coordinated by the same information scientist.
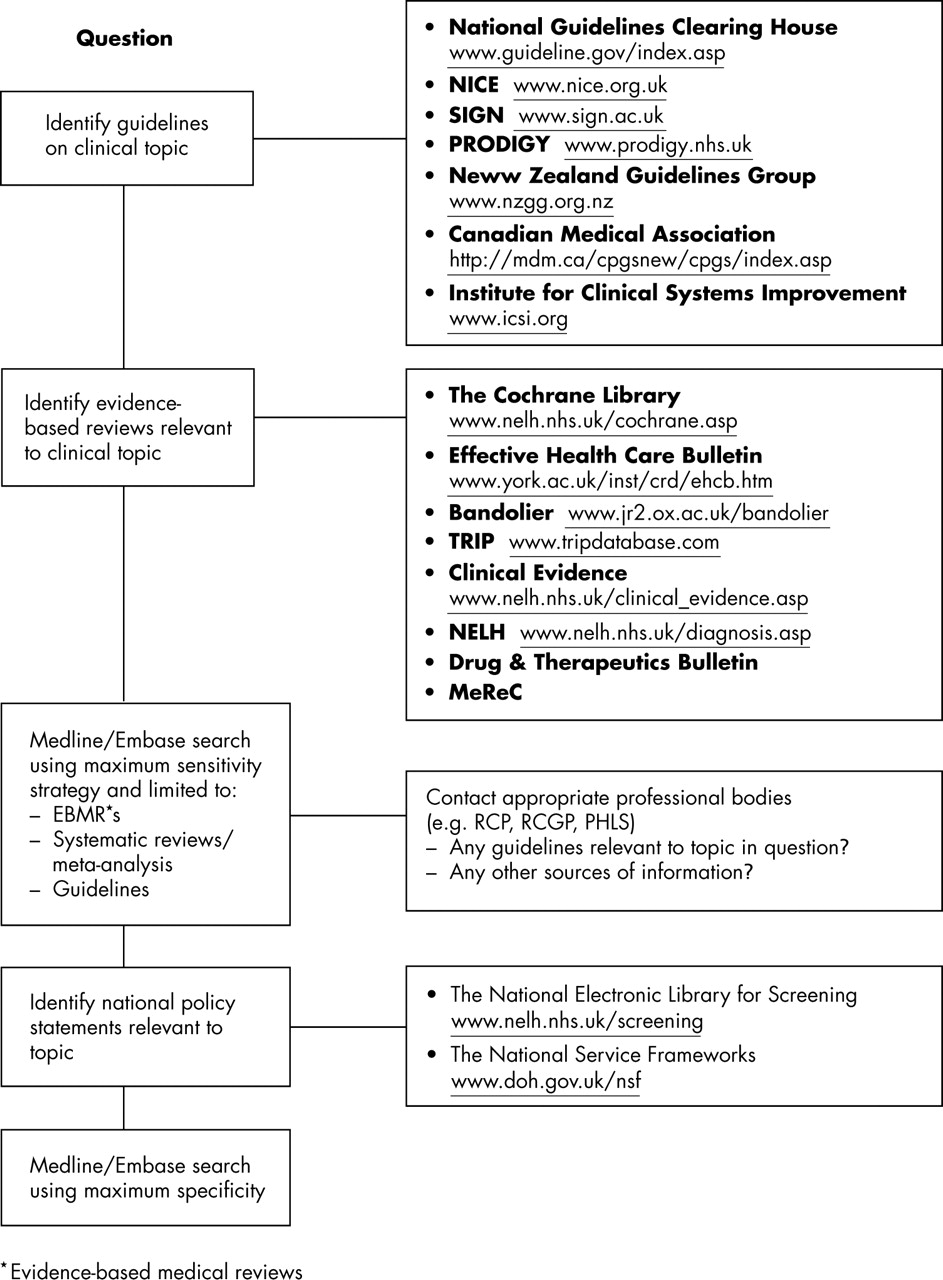
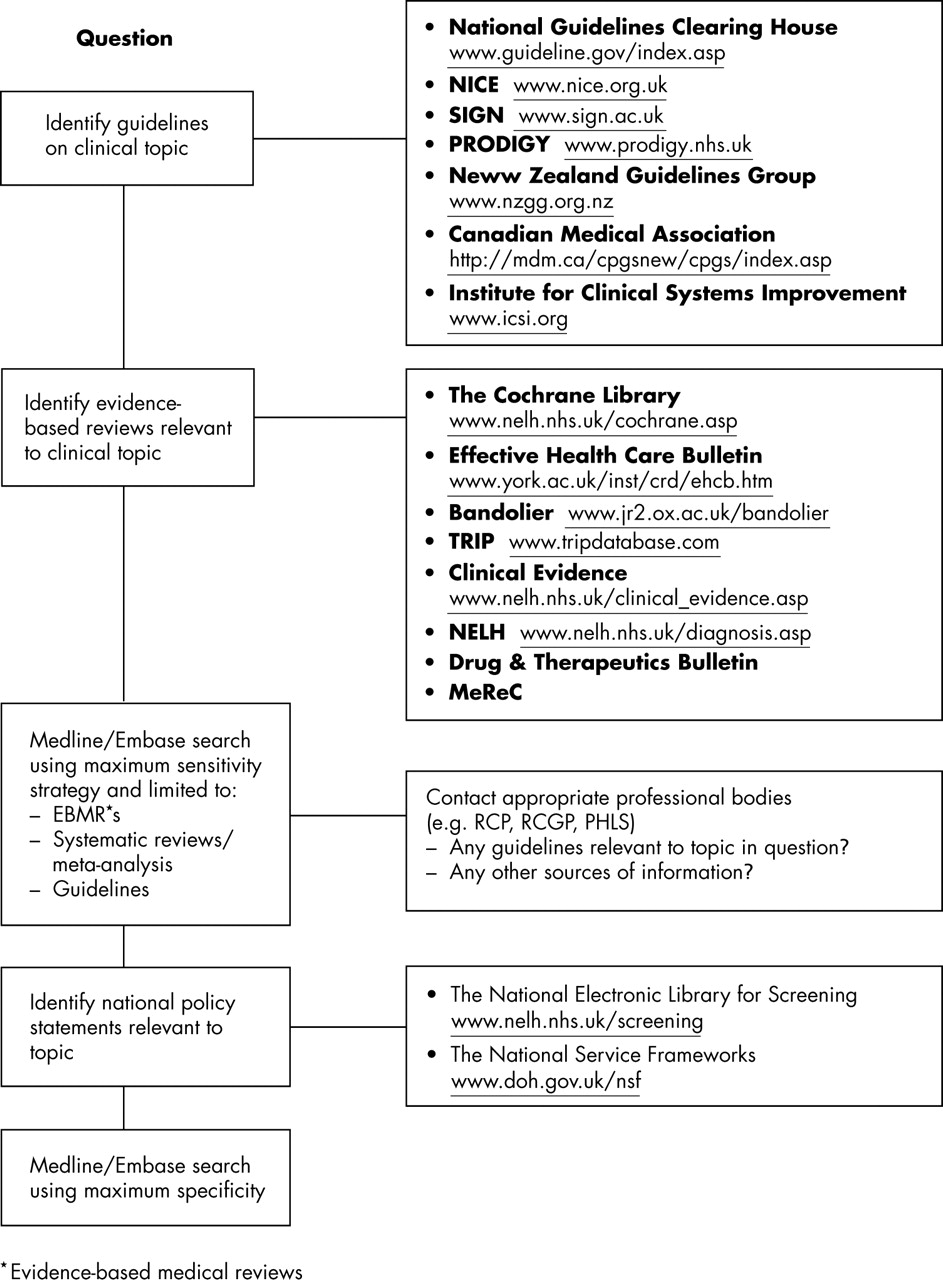
The strategy identified in the initial pilot work is based on specific searches for guidance documents combined with a high sensitivity Medline/Embase search to identify abstracts of potential contributory primary research papers (fig 3). The usefulness of the high sensitivity search is expected to vary depending on the availability of pre-existing reviews and consensus documents relating to each question. Subjects that have been extensively documented or for which a national service framework exists, such as management of cholesterol or diabetes, produce a high yield from the core search, whereas we expect several questions to have few if any related consensus documents and to make greater use of primary research. It is probable that specific topics requiring research will emerge for several questions for which the published literature may be very scarce. The search results are then sent electronically to authors.
{kind=link}
{kind=link}
{kind=link}
Outline search strategy for diagnosis based questions. Depending on the nature of the test—diagnostic or monitoring—the search is varied to include additional search options. The high sensitivity search will vary in its contribution to answers, depending on the amount of published guidance documents.
“The usefulness of the high sensitivity search is expected to vary depending on the availability of pre-existing reviews and consensus documents relating to each question”
PUBLICATION
The Journal of Clinical Pathology hopes to publish a series of reviews each designed to answer a set of five to 10 questions on related subjects. Thereafter, we hope that the resource will be made available to royal colleges and individual discipline associations for more widespread dissemination. Although laboratory medicine specialists represent only one of the target groups for this information, it is a logical starting place, because it will need laboratory medicine specialists to help drive the process forward with support from primary care.
CONCLUSION
Advances in information technology have opened up an opportunity to promote the best practice use of pathology. Web based guidance could improve patient management and contribute to medical and patient education, in addition to slowing the relentless but not always appropriate rise in laboratory tests and costs. Clinicians and laboratories need ready access to guidance that can inform initiatives to improve laboratory testing. Because of the manner in which laboratory tests are used in the scenarios identified, much of the evidence will be of level IV,18 and the guidance recommendations will be of grade D.19 In the context of the large variations in test requesting in both primary and secondary care, however, widespread availability of consensus advice can only represent a considerable improvement over the status quo.
The guidance generated should inform debate on improving practice and should not be seen as a series of standards to which doctors should be expected to work. The process does not need to be costly or difficult, but does require the judicious marriage of a sound evidence based approach with the degree of pragmatism required to distill available guidance into workable solutions for the medical practitioner. This is a subject Lundberg has been writing about for over 20 years,16 although there is probably a greater opportunity to move best practice forward now than ever before.
REFERENCES
Supplementary materials
Web-only Appendix
The appendix is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [View PDF] - Group Membership