Article Text

Abstract
Aims—To analyse the cost-effectiveness of three strategies for examining temporal artery biopsies based on data from cases examined over the past 10 years.
Methods—Of a total of 172 temporal artery biopsies, five were unsuitable for further analysis, 47 had already had levels cut, and 120 had levels cut as part of the study. All the biopsies were examined blind before and after levels. A tree with eventual diagnostic outcomes for different strategies was constructed and economic and sensitivity analyses performed. Welcan units were used to assess technical workload.
Results—Only one of the 132 initially normal cases and two of 14 diagnosed with periarterial lymphocytic infiltration (PALI) revealed giant cell arteritis after examining the tissue at multiple levels. Fifteen cases (8.9%) showed PALI not previously observed. The marginal cost for each extra case of giant cell arteritis detected was 83.5 Welcan units for a strategy of routine levels on all sections, and 21 Welcan units for a strategy of only cutting levels if PALI was present on the initial section. These costs were sensitive to the frequency of giant cell arteritis in cases with PALI and to the relative extra cost of moving from cutting single section to routine levels.
Conclusions—Routinely examining a temporal artery biopsy at multiple levels does not increase the diagnostic yield of the test, although selective further examination may be indicated in some cases. The significance of PALI is uncertain. The cost-benefit of the different strategies in terms of clinical decision making revolve around the perceived risk inherent in not making a diagnosis of giant cell arteritis.
- temporal artery biopsy
- economic analysis
- decision analysis
Statistics from Altmetric.com
Giant cell or temporal arteritis is a vasculitis that affects large and medium sized vessels in people over the age of 50 years; its diagnosis is established by the demonstration of granulomatous arteritis in a temporal artery biopsy.1–3 Increasing awareness of this disease has led to greater numbers of temporal artery biopsies.4–11 When positive, temporal artery biopsy provides the most definite evidence of giant cell arteritis, but the positive yield of this test is low, varying from centre to centre, reflecting the clinical threshold for doing the procedure,12–14 bilaterality of the biopsy procedure,15 the length of artery sampled, how many sections are scrutinised, the pathological criteria for diagnosing arteritis, the patchy nature of the disease, and perhaps a true variation in the incidence of the disorder. There is no gold standard for this test, and probably the most sensible gold standard would be a persisting clinical diagnosis at long term follow up.16
In this study, we have analysed the cost-effectiveness of three strategies for examining biopsies based on data from cases examined over the past 10 years in our laboratory.
Methods
All temporal artery biopsies reported in our department over 10 years were retrieved. The biopsies had been performed by various rheumatologists and ophthalmologists in the region, for a wide variety of clinical signs and symptoms suggestive of temporal arteritis (headaches, tender or pulseless temporal arteries, visual symptoms with or without increased erythrocyte sedimentation rate, plasma viscosity, or C reactive protein). None of the patients had been treated with steroids before the biopsy (although in some cases steroids were started concurrently with the decision to undertake the biopsy). The majority of the cases were from patients in their sixth, seventh, or eighth decade (range 46 to 90 years, median 70). The male to female ratio was 1:3.
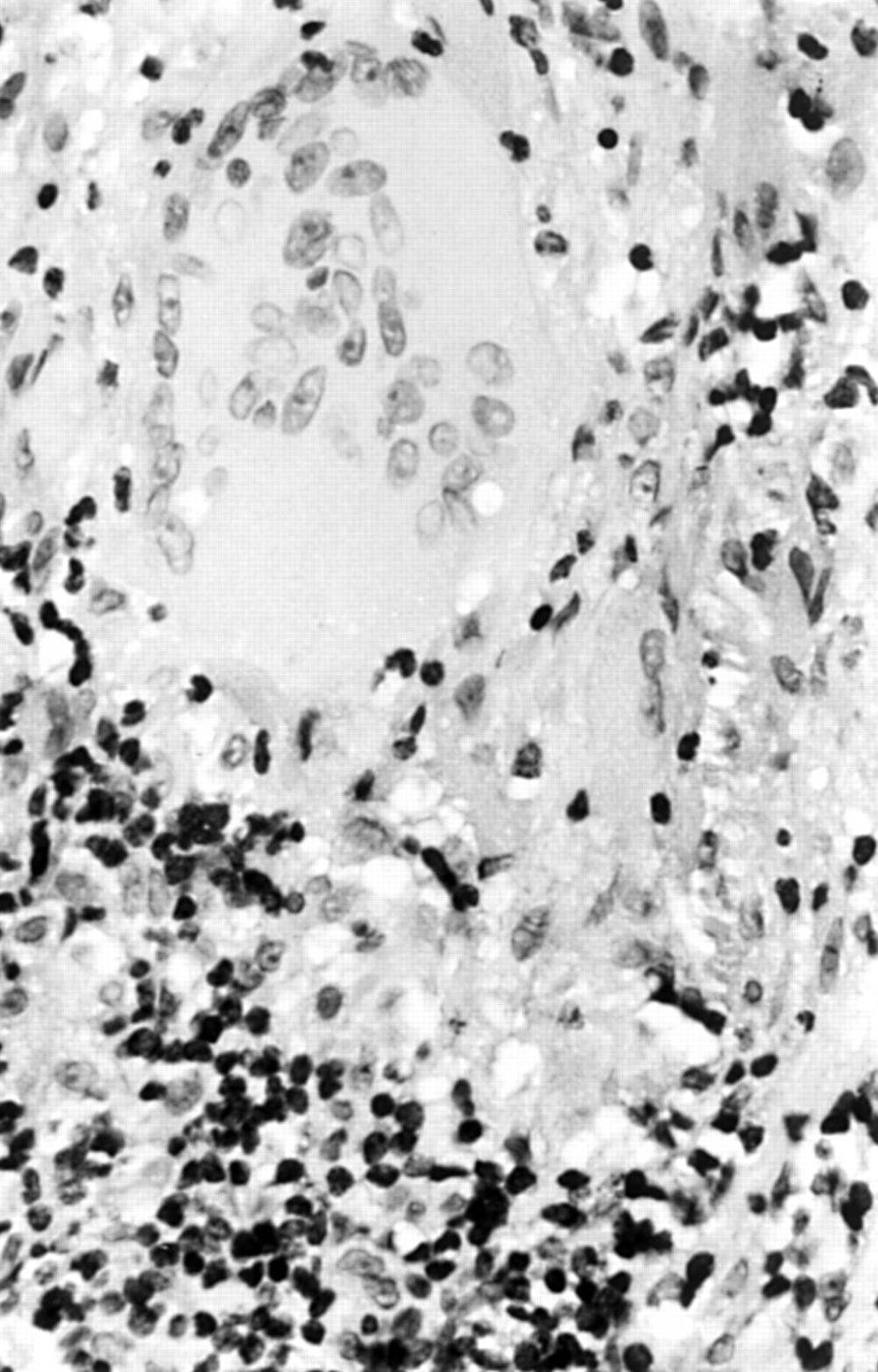
A diagnosis of giant cell arteritis was made on recognising a pattern of destructive panarteritis with or without multinucleated giant cells (fig 1).
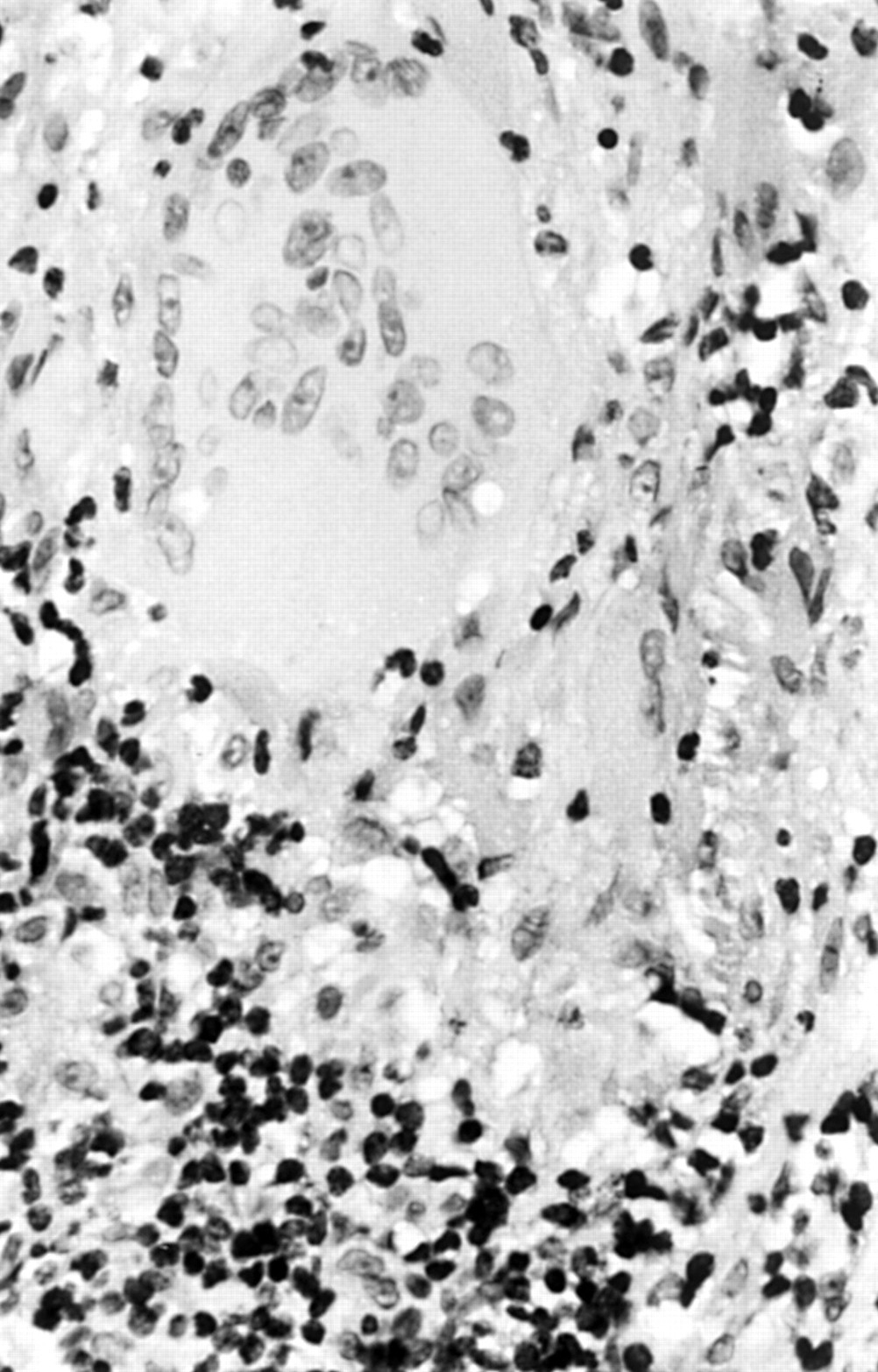
Giant cell arteritis characterised by dense lymphocytic infiltration and multinucleated giant cells. (Haematoxylin and eosin.)
The biopsy length varied considerably, ranging from 1 mm to 50 mm (mean and median, 10 mm). When sufficiently long—that is, at least 6 mm—the artery was examined in one longitudinal section, and two transverse sections, one from either end of the artery segment. Smaller biopsies were examined in multiple transverse sections only.
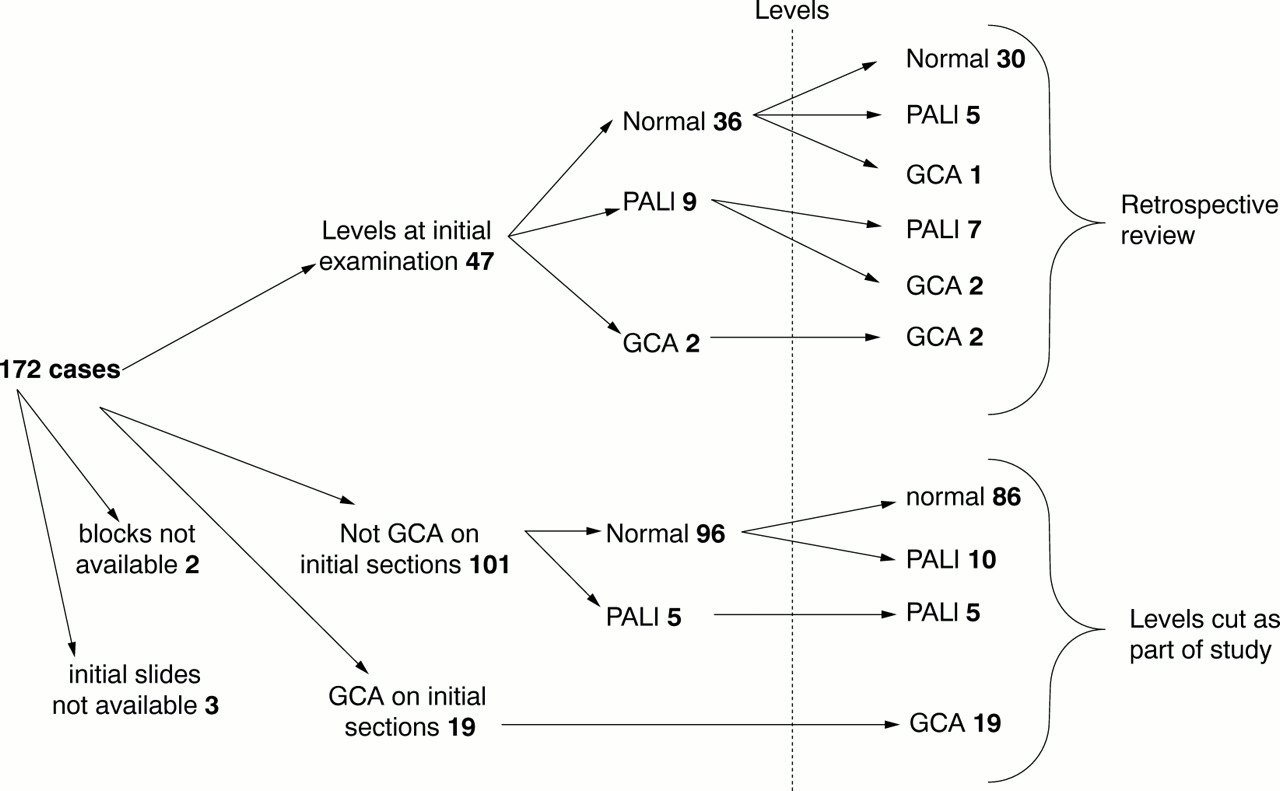
In all there were 172 temporal artery biopsies; five were unsuitable for further analysis, 47 already had levels done (therefore were initially excluded from the examination), and 120 had levels done as part of the study. Of these 120 cases, 19 were originally diagnosed as giant cell arteritis and therefore were included as controls in the study; of the remaining 101 biopsies, 96 were normal and five had periarterial lymphocytic infiltration (PALI) (fig 2).

Temporal artery with a focus of lymphocytic infiltration around a periarterial venule. (Haematoxylin and eosin.)
Two neuropathologists examined 120 biopsies (19 with giant cell arteritis, 101 without giant cell arteritis) blind and independently, after cutting multiple levels of both transverse and longitudinal sections (sections were cut at three levels, each level at a quarter of the thickness of the tissue; therefore the distance between levels for every tissue sample was different depending on the total tissue thickness). Sections were stained with haematoxylin and eosin (H&E).
The sections (before and after levels) from the 47 initially excluded biopsies were then examined retrospectively and blindly by one pathologist and the data included in the construction of an economic model.
Welcan units were used for construction of the diagnostic model and economic and sensitivity analyses. (Welcan Units: Workload Measurement System for Pathology, September 1988, Welsh Office). Welcan is a system which provides a proven scientific basis for the measurement of laboratory activity, of which the quantitation of technical workload is one aspect. Workload measurement involves identification of laboratory procedures carried out, accurately counting the number of procedures performed daily as defined for workload recording, and converting the number of procedures into units to obtain the average technical, clerical, and aide time required to perform a laboratory procedure. Therefore one Welcan unit is equal to one minute of technical, clerical, and aide time. In histopathology, the unit value allocated for preparing one H&E stained slide is 3.
Results
REVIEW OF CASES INITIALLY EXAMINED BY A SINGLE SECTION
There was complete concordance in the observations made by the two pathologists. The length of the biopsied section of artery in cases diagnosed as giant cell arteritis differed only very slightly from that of the negative biopsies (giant cell arteritis biopsies: range 2–33 mm, median 9 mm; negative biopsies: range 1–50 mm, median 10 mm; Mann–Whitney U test p = 0.58). None of the 101 initially negative biopsies revealed giant cell arteritis after examination of the tissue at multiple levels; however, 15 of these cases showed lymphocytic infiltration (previously observed in only five cases: 14.9% v 5.0%; 95% confidence limits of the difference 1.8% to 18%), restricted to either the interstitium or vasa vasorum (fig 2) and designated as PALI. The infiltrate was perivascular in nature, without any destruction of the small vessel walls (fig 2). There was no associated inflammation, fibrosis, or damage to the tunica media of the temporal artery. In some cases, there was associated calcification or fragmentation of the internal elastic lamina and mild thickening of the tunica intima (fig 3).

Temporal artery with calcification of the elastic lamina (arrow) and a focus of periarterial lymphocytic infiltration. (Haematoxylin and eosin.)
REVIEW OF CASES INITIALLY EXAMINED WITH LEVELS
In the group of 47 biopsies in which levels had already been cut, these had been requested in 31 cases (65.9%) at the time of cut up before looking at the histology, in three cases (6.3%) because the biopsy was of a small size, in one case (2.1%) because the tissue was fragmented, in three cases (6.3%) owing to an incomplete transverse section of the initial section, and in nine cases (19.1%) because the initial section showed adventitial lymphocytes of varying density.
Thirty six biopsies were normal at initial section, of which 30 (83.3%) remained normal after levels, five (13.8%) showed foci of adventitial lymphocytes, and one (2.7%) showed giant cell arteritis. In the latter case the fragmented nature of the biopsy had prompted a request for levels. The frequency of PALI was significantly higher after examination with levels (0% v 13.9%, 95% confidence limits of the difference 2.5% to 25%).
Nine biopsies showed adventitial lymphocytes of varying density at initial section, seven (77.8%) still showed adventitial lymphocytes, and two (22.2%) showed giant cell arteritis; two biopsies showed giant cell arteritis at initial section and after levels (fig 4).

Diagnostic pathway of cases under study. GCA, giant cell arteritis; PALI, periarterial lymphocytic infiltration.
CONSTRUCTION OF DIAGNOSTIC MODEL
The total sample consisted of 172 cases. Of these, material from five was not available for review. The data from the remaining 167 cases were used to construct a diagnostic tree with eventual diagnostic outcomes (fig 5). On the basis of these figures, a computer model of the decision tree was constructed from which the diagnostic yield from three different strategies was calculated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Structure of economic model. GCA, giant cell arteritis; PALI, periarterial lymphocytic infiltration.
The strategies were:
-
Single examination only (no levels).
-
Routine levels on all cases.
-
Levels only in cases of PALI.
Costs for each strategy were calculated, based on an assumption that if the cost for a case examined at a single level was 3 Welcan units, the cost of doing routine levels was 50% higher than a single level (4.5 Welcan units), and the cost of doing selected (later) levels was doubled for each case (6 Welcan units). Marginal costs and yields, and the cost per extra case of giant cell arteritis, were derived for each strategy. Costs were calculated with reference to the data in fig 5 and the costs for each of the 167 cases examined. More details of the cost calculations are given in the appendix.
The upper and lower confidence limits of the various diagnostic outcomes, after levels had been examined, were calculated and incorporated in the model. For example of 14 cases initially diagnosed as PALI, two were diagnosed as giant cell arteritis after levels had been examined. This yields a rate of 14.3% with confidence limits of 42.8% to 1.8%. These limits were subsequently used in the sensitivity analyses which allowed calculation of economic outcomes if the frequency of giant cell arteritis was as high as the upper confidence limit or as low as the lower limit. The sensitivity of the results to the assumptions about the differential cost of the various strategies was also examined.
ECONOMIC ANALYSES
The analyses were based on the diagnostic data from 167 cases detailed in the previous section: 132 were diagnosed as normal, 14 as having PALI, and 21 as having giant cell arteritis after the initial examination (before levels were cut). When these cases were examined at three levels, of the 132 “normal” cases, 116 were classified as normal, 15 as PALI, and one as giant cell arteritis. Of the 14 cases initially classified as PALI, 12 were classified as PALI and two as giant cell arteritis.
The average cost per case of giant cell arteritis diagnosed with a single section was 23.86 Welcan units. The total cost of strategy A was 501 Welcan units, of strategy B 751.5 units, and of strategy C 543 units. These are equivalent to 3.0, 4.5. and 3.25 Welcan units/specimen, respectively.
The two alternative strategies for cutting levels were compared with the strategy of examining samples with a single section.
Strategy A (single section only) compared with strategy B (routine levels on all cases)
The data on diagnostic yields and costs of the two strategies are shown in table 1. Implementing a strategy of routine levels would have yielded three more cases of giant cell arteritis and 13 more cases of PALI. The cost for each extra case of giant cell arteritis diagnosed was 83.5 Welcan units. The cost for each extra case of giant cell arteritis or PALI diagnosed (if all were considered together) was 15.66 Welcan units.
Comparison of yields and costs of strategy A (examination of a single section) with strategy B (routine levels)
Strategy A (single section only) compared with strategy C (levels on all cases of PALI)
The data on diagnostic yields and costs of the two strategies are shown in table 2. Implementing a strategy of levels only for cases with PALI would have yielded two more cases of giant cell arteritis. The cost for each extra case of giant cell arteritis diagnosed was 21 Welcan units.
Comparison of yields and costs of strategy A (examination of a single section) with strategy C (levels cut if initial section shows PALI)
Strategy B (routine levels) compared with strategy C (levels on all cases of PALI)
From the data in tables 1 and 2 it can be calculated that strategy B yields one extra case of giant cell arteritis over strategy C but costs an extra 208.5 Welcan units, which is nearly 10 times the marginal cost of changing from a strategy of single section to one of cutting levels only in cases with PALI (21 Welcan units).
SENSITIVITY ANALYSES
The sensitivity of results was tested against the assumptions of frequency of giant cell arteritis in cases with PALI, and the assumptions of the relative costs (in Welcan units) of the three strategies. The results are shown in table 3 and are compared with the results derived directly from the study data. It can be seen that the results are sensitive to the assumptions of the frequency of giant cell arteritis in cases with PALI and the relative extra cost of moving from cutting a single section to cutting routine levels. If the frequency of giant cell arteritis in cases with PALI was as high as the upper confidence limit (42.8%) the marginal cost of strategy C (compared with strategy A) falls dramatically to 7.01 Welcan units. However, these values are based on a small number of cases with correspondingly wide confidence limits and studies on far larger series would be necessary to derive a more robust estimate.
Analysis of sensitivity of economic model to assumptions of frequency of giant cell arteritis (GCA) in cases with periarterial lymphocyte infiltration (PALI) and relative costs of diagnostic strategies
Discussion
Our study has addressed the question of the optimum strategy for the examination of temporal artery biopsies taken as part of the investigation of possible giant cell arteritis. The central issue is the balance between the risk of missing a case of giant cell arteritis and the cost of unnecessarily undertaking extensive histological examination of cases without giant cell arteritis.
Giant cell arteritis is typically described as having skip lesions and can be found in temporal artery segments as short as 330 μm in length.17,18 We believe that by sampling the temporal artery with two transverse sections from the two extremes of the arterial segment and a longitudinal section from the intervening middle portion, one can reasonably overcome the chance of missing lesions. Lesions of giant cell arteritis usually involve the entire area of a transverse section and are not segmental in terms of cross sectional area, and it is therefore unlikely that a lesion will be missed in a longitudinal section.
In our first group of 101 cases, examining the temporal artery at multiple levels did not increase the diagnostic yield of the test in terms of cases of giant cell arteritis diagnosed; the clinical threshold for performing the biopsy may, however, be a critical factor.16 Nevertheless, examination at multiple levels has picked up a significantly larger number of cases with periarterial inflammation (PALI) than were apparent from the initial single section.
The significance of PALI is uncertain; it may reflect normal lymphoid populations, part of changes associated with ageing,1 residual inflammation from previous arteritis,19,20 close proximity of full blown vasculitis, or a systemic vascular disorder.21 Most of the cases in our study were from an elderly population and so lymphocytic infiltrates in surrounding tissues reflecting age changes cannot be excluded in this group of patients. An eventual diagnosis of giant cell arteritis was made on examination of levels in only two of 14 cases with PALI.
Vasculitis of the vasa vasorum of the temporal artery may be an indicator of various types of systemic disorders including well characterised diseases such as giant cell arteritis and polyarteritis nodosa. This picture resembles the well known vasculitis located in vasa nervosum of the peripheral nerve or in epimysial and perimysial vessels of skeletal muscles in a range of conditions including relapsing polychondritis, rheumatoid arthritis, cholesterol embolism, and glomerulonephritis, among others.
Our study shows that, although examination of temporal artery biopsies at multiple levels does result in a small increase in the diagnostic yield in terms of cases of giant cell arteritis diagnosed, it also picks up cases with periarterial inflammation. This has been held to warrant clinical surveillance for systemic vasculitic syndromes,16 although this assertion is based on a highly selected case series rather than a representative population sample.
Based on the assumptions inherent in the economic model and on the data from the current series of cases, switching to a strategy of routinely cutting levels on all temporal artery biopsies would detect around two extra cases for every 100 temporal artery biopsies examined, at a cost of 83.5 Welcan units for each extra case detected. The value of this information, in terms of clinical decision making, is related to the perceived risk inherent in not making a definitive diagnosis of giant cell arteritis and the opportunity costs of 83.5 Welcan units. On the face of it, the strategy of only doing levels on cases where there is, a priori, a higher probability of finding giant cell arteritis (in our series these would be the cases with PALI) is more cost-effective, with a marginal cost for each extra case of 21 Welcan units. However, if value (in terms of a potential contribution to clinical decision making) is ascribed to the presence of PALI, then the strategy of routine levels has a lower marginal cost of 15.66 Welcan units. The earlier discussion on the significance of PALI leaves the matter unresolved.
The sensitivity of the marginal cost estimates to the assumptions of the relative costs of the three strategies is evident from the sensitivity analyses. In practice the decision is more likely to depend on the absolute costs of each strategy (which will depend on the frequency with which the examination is undertaken by the laboratory), and whether the risks inherent in examining a single section only are acceptable given the pattern of clinical management being followed.
Our study took place in a setting where the prevalence of giant cell arteritis in the population of patients biopsied was approximately 14%, the majority (87.5%) diagnosed on a single initial section. The model constructed for this study is clearly sensitive to the assumptions of prevalence in cases not diagnosed as giant cell arteritis after an initial section. In effect a strategy of routine levels involves cutting levels “unproductively” in nearly 70% of biopsies but identifies the remaining 15% of cases of giant cell arteritis. If a negative temporal artery biopsy is considered as a definitive exclusive test then clearly the risks inherent in missing 15% of cases of giant cell arteritis would not be acceptable; however, in the face of strong clinical suspicion it is unlikely that effective treatment would be stopped, given the recognised risk of a negative biopsy owing to skip lesions.
This series was constructed retrospectively from cases in which levels had already been cut and examined, as well as cases which had been examined only at a single level. While overall, three extra cases of giant cell arteritis were diagnosed after examination at levels, all these cases were in the group that had originally been examined in this way; in the cases in which levels were cut subsequently (for the purposes of this study), no cases of giant cell arteritis were found, although 15 cases with PALI were found in 101 cases examined. This would suggest that a strategy of examining a single section initially and then deciding whether to cut levels depending on the findings is safe (although not formally analysed in this study), if one is solely concerned with detecting giant cell arteritis as a histological diagnosis and not PALI.
In summary the decision on whether or not to examine temporal artery biopsies at multiple levels depends on the view one takes of the importance of periarterial lymphocytic infiltrates rather than on any proven increase in the detection rate of giant cell arteritis (when compared with an examination of a longitudinal and two transverse sections at a single level). There are differences in cost-effectiveness in alternative strategies for examining temporal artery biopsies, but any strategy that does not involve routine examination at multiple levels should incorporate explicit judgement on which cases require further study.
Appendix
BASIS FOR COST CALCULATIONS
In this study, a case examined at a single level was allocated 3 Welcan units. The cost of doing selected (later) levels was doubled for each case (6 Welcan units), on the basis that the later work was similar to that involved in the original (initial) section. The cost of doing routine levels was 50% higher than a single level (4.5 Welcan units), as the extra work was limited to mounting and staining extra slides with no extra work involved in setting the block and little in the extra cutting. These values are based on professional and technical judgement and while they may not reflect exact time values involved in the work undertaken, they do reasonably reflect the relative time involved in each strategy.
In strategy A all cases cost 3 Welcan Units and in strategy B all cases cost 4.5 Welcan units. In strategy C (levels only if PALI present in initial sections), reference to table 2 indicates that 132 cases would be diagnosed as normal at a cost of 3 Welcan units each (costing 396 units); 14 cases of PALI would have levels yielding 12 cases of PALI (costing 72 units, that is, 12 × 6 Welcan units) and two cases of giant cell arteritis (costing 12 units, that is, 2 × 6 Welcan units); and 21 cases of giant cell arteritis are diagnosed at the initial section (costing 63 units, that is, 21 × 3 Welcan units). Thus the costs of 543 Welcan units for strategy C (in table 2) are made up of 396 units for normal, 72 units for PALI, and 75 units for giant cell arteritis
Acknowledgments
We are grateful to Peter Jackson for technical assistance.