Article Text

Abstract
Aims—In anaplastic large cell lymphoma (ALCL), the site of origin has been described as an important prognostic factor. Recently, a fusion protein containing anaplastic lymphoma kinase (ALK) was described in systemic nodal ALCL, and shown to be associated with a good prognosis. The aims of this study were to investigate whether the presence of ALK protein differs between ALCL of different sites of origin; to determine whether ALK expression occurs before dissemination to other sites; and, finally, to investigate whether the site of origin remains a prognostic parameter in ALK negative ALCL.
Methods—ALK expression, as detected by immunohistochemistry using the monoclonal antibodies ALK1 and ALKc, was studied in 85 ALCLs from different sites of origin. In 22 patients, ALK expression was studied in multiple biopsies from different sites (including 13 skin, 16 lymph node, and nine other). Overall survival time was analysed using the Kaplan Meier method.
Results—ALK expression was found in 20 of 51 systemic ALCLs with (primary) nodal involvement. No ALK expression was found in 15 primary cutaneous, 14 gastrointestinal, and five nasal ALCLs. Multiple and subsequent biopsies of patients showed ALK expression to be identical to that seen in the primary diagnostic biopsy. Kaplan Meier survival curves showed that in ALK negative ALCLs originating from different sites, primary cutaneous cases are associated with an excellent overall survival, whereas the other cases show a comparable five years survival of less than 40%.
Conclusions—If present, ALK expression favours systemic ALCL with (primary) nodal involvement, and can be used in differentiating between extranodal involvement of systemic (nodal) ALCL and primary extranodal ALCL. ALK is expressed consistently in multiple biopsies of a given patient, indicating that the chromosomal abnormality leading to aberrant ALK expression occurs before dissemination to other sites. Finally, in ALK negative non-cutaneous ALCLs, different sites of origin show comparable poor survival.
- anaplastic large cell lymphoma
- extranodal
- anaplastic lymphoma kinase
- survival
Statistics from Altmetric.com
In 1985, anaplastic large cell lymphoma (ALCL) was recognised as a separate disease entity,1 characterised by cohesive sheets of large CD30 positive cells with multiple or single prominent nucleoli and T cell or null cell characteristics.2 In 1993, we described differences in clinical behaviour between primary nodal and primary cutaneous ALCL.3 These differences are reflected in the two types of ALCL recognised in the revised European-American classification of lymphoid neoplasms (REAL classification).2 The first type is a systemic variant, mainly presenting in lymph nodes, with a prognosis better than that of other T cell lymphomas.4 The second is a primary cutaneous variant with a very favourable prognosis.3,5,6 Recently, at the IX meeting of the European Association for Haematopathology (Leiden, The Netherlands, April 26–29, 1998) the proposed list for the new WHO classification of leukaemias and lymphomas was presented. This included among the extranodal T cell lymphomas the enteropathy type intestinal T cell lymphoma and the (natural killer/T cell) nasal type, which are usually very aggressive, irrespective of whether their morphology is small cell or anaplastic.2,7–9 Thus, in the group of lymphomas with anaplastic morphology, distinction between different sites of origin is important, because of the differences in clinical behaviour and consequent therapeutic strategies.
About 15–85% of systemic (nodal) ALCLs contain the t(2;5)(p23;q35) translocation, which fuses the anaplastic lymphoma kinase (ALK) gene at 2p23 with the nucleophosmin (NPM) gene at 5q35, resulting in a fusion protein NPM–ALK.10 In about 15% of ALK positive cases, genetic aberrations other than the t(2;5) translocation are involved, fusing the ALK gene to a gene other than NPM.11–16 Recently, two monoclonal antibodies, ALK115 and ALKc,17 were developed that detect the ALK portion of the fusion protein in formalin fixed, paraffin wax embedded tumour specimens by immunohistochemistry. Previous to that, the polyclonal antibody p80 had been developed.18 In various studies, expression of ALK was found to be related to a more favourable clinical outcome.19–23 Expression of t(2;5) and/or ALK in ALCLs at different sites has been studied by several groups, their results depending on the detection methods used. Using cytogenetics, reverse transcriptase polymerase chain reaction (RT–PCR), in situ hybridisation (ISH), and immunohistochemistry, most groups found ALK expression in systemic (nodal) ALCL and not in primary cutaneous ALCL or lymphomatoid papulosis.15,24–26 However, in two studies NPM–ALK transcripts were detected in cutaneous ALCL by nested RT–PCR with two amplification steps.27,28 Another study29 found positive staining with the antibodies p80 and ALK1 in one of eight cases of primary cutaneous ALCL, but no evidence of ALK expression with standard RT–PCR. To our knowledge, ALK expression has not been studied in nasal T cell lymphomas with anaplastic morphology. A recent study by Ott and colleagues27 found no evidence of the t(2;5) translocation in two primary gastrointestinal ALCLs; the study on ALK positive ALCLs by Benharroch and colleagues30 included 18 extranodal samples, but did not mention whether these samples included primary gastrointestinal ALCLs.
In our present study, we investigated the expression of ALK in ALCLs arising at different sites, and whether ALK expression can be used to distinguish between systemic (nodal) ALCL and primary extranodal ALCL. Furthermore, the expression of ALK was studied in multiple and/or subsequent tumour biopsies of patients, to determine whether the t(2;5) translocation is an early pathogenic event—before dissemination to other sites. Finally, we investigated whether the site of origin in ALK negative ALCL remains an important prognostic parameter.
Methods
PATIENT SELECTION
From the files of the Comprehensive Cancer Center Amsterdam, the Netherlands; and from the department of pathology of the University of Vienna, Austria, we selected patients with systemic (nodal) ALCL (n = 51), including morphological subtypes such as the small cell variant (n = 4).30,31 Furthermore, primary cutaneous CD30 positive lymphoproliferative disorders were selected, including primary cutaneous ALCL (n = 15) and lymphomatoid papulosis (n = 7). We also selected primary gastrointestinal (n = 14) and nasal (n = 5) T cell lymphomas with anaplastic morphology, consisting of large tumour cells with pleomorphic or monomorphic round nuclei, and multiple or single prominent nucleoli. These cases are henceforward referred to in the text as primary gastrointestinal ALCL and primary nasal ALCL. All samples showed CD30 expression of virtually all tumour cells. Moreover, they were of T cell lineage (they expressed CD3 and/or CD45RO/UCHL-1, in the absence of B cell markers L26/CD20 and CD79a) or of null cell lineage (both T and B cell markers were absent).
Systemic (nodal) ALCL was defined as disease mainly involving lymph nodes, with or without extranodal tumour localisations. Patients showing coexistent nodal and extranodal localisations were categorised as systemic (nodal) ALCL if the lymph node localisations were not restricted to nodes draining the extranodal tumour. This included one patient who presented with intestinal (jejunal) ALCL concurrent with nodal (mesenteric and para-aortic) localisations.
In contrast, ALCLs that presented clinically primarily in the nose or in the gastrointestinal tract (with no or only locoregional lymph node involvement), were defined as primary nasal and primary gastrointestinal ALCLs, respectively. ALCLs arising in the skin were considered primary cutaneous if extensive staging of patients showed no extracutaneous disease within six months of diagnosis.5
From 22 patients, we obtained multiple biopsies from concurrent localisations (n = 7) or relapses (n = 31), including 13 skin localisations, 16 nodal, and nine other localisations. For each patient the following characteristics were noted from the medical records: age at diagnosis, sex, Ann Arbor stage at presentation, treatment, response, the occurrence of relapses, and cause of death.
ALK DETECTION
Expression of ALK was detected in formalin fixed, paraffin wax embedded biopsy specimens by immunohistochemistry using the monoclonal antibodies ALK1 and ALKc, which were developed in the laboratories of KP (Oxford, UK) and BF (Perugia, Italy), respectively. Both antibodies react specifically with an intracytoplasmic epitope of the ALK protein, and correlate strongly with genetic aberrations involving the ALK gene at 2p23.15,17 Staining was performed as described previously,15,17 with minor modifications. Antigen retrieval was achieved by placing dewaxed slides in citrate buffer (0.01 M, pH 6.0) and heating them in a 700 W microwave oven for 10 minutes. The slides were then removed and allowed to cool at room temperature for 30 minutes. After washing in water, endogenous peroxidase was blocked with 1% hydrogen peroxide in methanol for 30 minutes, after which slides were rinsed in phosphate buffered saline before beginning the three step staining technique using the DAKO Strept ABC complex/HRP Duet kit. Slides were incubated with ALK1 (using a 1/50 dilution) or ALKc (1/5 dilution) for one hour at room temperature, and staining was enhanced by the catalysed reporter deposition (CARD) method, which amplifies biotinylated sites.32 The peroxidase reaction was developed using 3,3`-diaminobenzidine tetrahydrochloride (DAB) and 0.01% vol/vol hydrogen peroxide. There were no discrepancies found between ALK1 and ALKc with regard to presence or absence of staining—if a tumour biopsy stained positively with ALK1 it was also found to be positive with ALKc, and vice versa. Cases were considered ALK positive if tumour cells showed positive labelling, irrespective of their number.
STATISTICAL ANALYSIS
Survival time was measured from time of initial diagnosis until death as a result of the disease, or until end of follow up. Patients who died of causes unrelated to the disease were censored at the time of death. Progression free survival time was measured from time of initial diagnosis until time of disease relapse.
Survival curves were constructed with the Kaplan Meier method, and differences between the curves were analysed using the log rank test. Comparisons of means were performed using the Kruskal-Wallis test, and qualitative variables were analysed by the Pearson χ2 or Fisher's exact test, where appropriate. All p values are based on two tailed analysis and p values below 0.05 were considered to be significant. All analyses were performed using the SPSS statistical software (SPSS Inc Chicago, Illinois, USA).
Results
ALK EXPRESSION IN SYSTEMIC NODAL AND EXTRANODAL ALCL
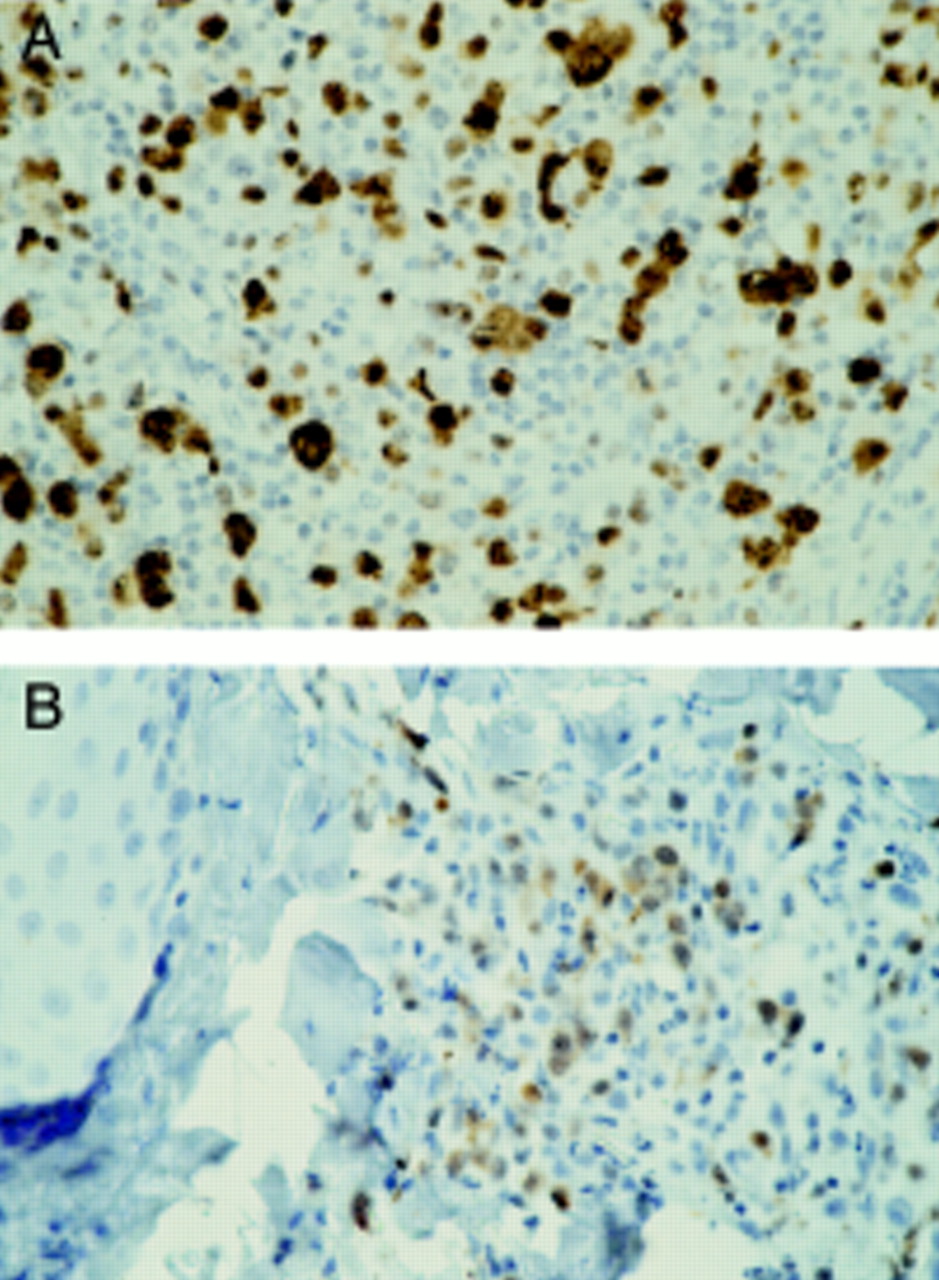
As shown in table 1, ALK expression was found in 20 of 51 (39.2%) systemic ALCLs with nodal involvement, including the patient in whom ALCL in an intestinal (jejunal) localisation was found concurrently with abdominal lymph node involvement (fig 1). Of 15 primary cutaneous ALCLs, seven lymphomatoid papulosis, 14 primary gastrointestinal, and five primary nasal ALCLs, none showed ALK expression.
ALK expression in anaplastic large cell lymphoma (ALCL) according to site of origin

Anaplastic lymphoma kinase (ALK) expression in tumour biopsies of a patient with concurrent nodal (A) and intestinal (B) anaplastic large cell lymphoma. Brown cytoplasmic and nuclear staining of the tumour cells indicates ALK expression, as detected by the monoclonal antibody ALKc. Haematoxylin counterstaining; original magnification, ×400.
Samples staining positively for ALK1 were also ALKc positive, and vice versa. When present, ALK expression was seen as brown cytoplasmic and nuclear staining of almost all tumour cells in most cases (15 of 20). In five cases, staining was restricted to the cytoplasm of tumour cells (table 1 and fig 2). ALK1 and ALKc antibodies gave the same staining pattern (cytoplasmic and nuclear as opposed to cytoplasmic only), but nuclear positivity tended to be stronger with ALKc.

A systemic (nodal) anaplastic large cell lymphoma case with brown, cytoplasm restricted anaplastic lymphoma kinase (ALK) staining of the tumour cells. The cytoplasm restricted staining pattern is the same for monoclonal antibodies ALK1 (A) and ALKc (B). Haematoxylin counterstaining; original magnification, ×600.
PRESENCE OR ABSENCE OF ALK EXPRESSION IS CONSISTENT WITHIN PATIENTS
Of the patients with systemic (nodal) ALCL, 11 had multiple biopsies taken at diagnosis and/or presented with recurrent disease. The same was true for seven patients with primary cutaneous ALCL, two with primary gastrointestinal ALCL, and two with primary nasal ALCL (table 2).
ALK expression in ALCL specimens of patients with multiple biopsies or recurrent disease
ALK expression was found to be consistent within patients; that is, if a patient presented with ALK positive ALCL, all other tumour biopsies of that patient were also found to be ALK positive. For instance, three patients with ALK positive systemic (nodal) ALCL had one or several relapses (including cutaneous and nodal localisations). ALK positivity was found in all relapses (table 2, cases 1–3; fig 3). In the patient who presented with concurrent intestinal and nodal ALCL, both tumour biopsies showed ALK positivity (table 2, case 4; fig 1). The pattern of staining (cytoplasmic and nuclear, or cytoplasmic only), as demonstrated by the primary diagnostic biopsy, remained the same in subsequent biopsies. Finally, in patients presenting with ALK negative lymphoma, all other biopsies of those patients were also found to be ALK negative (table 2).
Anaplastic lymphoma kinase (ALK) expression in tumour biopsies of a patient with systemic nodal anaplastic large cell lymphoma (A) and a cutaneous relapse (B). Brown cytoplasmic and nuclear staining of the tumour cells indicates ALK expression, as detected by the monoclonal antibody ALK1. Haematoxylin counterstaining; original magnification, ×400.
PATIENT CHARACTERISTICS AND SURVIVAL
We analysed the clinical behaviour of ALCL originating from different primary sites. A full evaluation of clinical data was possible in 48 cases of systemic (nodal) ALCL (18 ALK positive, 30 ALK negative), 10 cases of primary cutaneous ALCL, 13 cases of primary gastrointestinal, and all cases (n = 5) of primary nasal ALCL. We found that ALK positive systemic (nodal) ALCL tended to present with Ann Arbor stage 1 or stage 2 (12 of 18 cases), whereas ALK negative systemic (nodal) ALCL presented more often with stage 3 or 4 (20 of 30 cases) (Fisher's exact test, p = 0.03). Primary cutaneous ALCL usually presented as a solitary skin tumour (n = 12), whereas only a few primary cutaneous ALCLs presented as multicentric (n = 2) or generalised (n = 1) cutaneous tumours. Primary gastrointestinal ALCL was usually confined to the gastrointestinal tract, but in three of 14 cases showed involvement of one other site, such as the spleen (one case; no biopsy available) or a regional lymph node (table 2, cases 12 and 13). Two of five primary nasal ALCLs were confined to the nose, two had locoregional lymph node involvement at the time of diagnosis (no biopsies available), and one case showed involvement of a testicle (table 2, case 14).
In the group of systemic (nodal) ALCLs, ALK expression showed a predilection for younger patients and was significantly related to a favourable clinical outcome (table 3). Only two of 18 patients with ALK positive systemic nodal ALCL (one of whom refused treatment) died as a result of the disease. The patient with concurrent intestinal and nodal ALCL entered complete remission after polychemotherapy, and was alive and well (without relapse) 14 months after diagnosis.
Clinical characteristics of anaplastic large cell lymphoma of different sites of origin
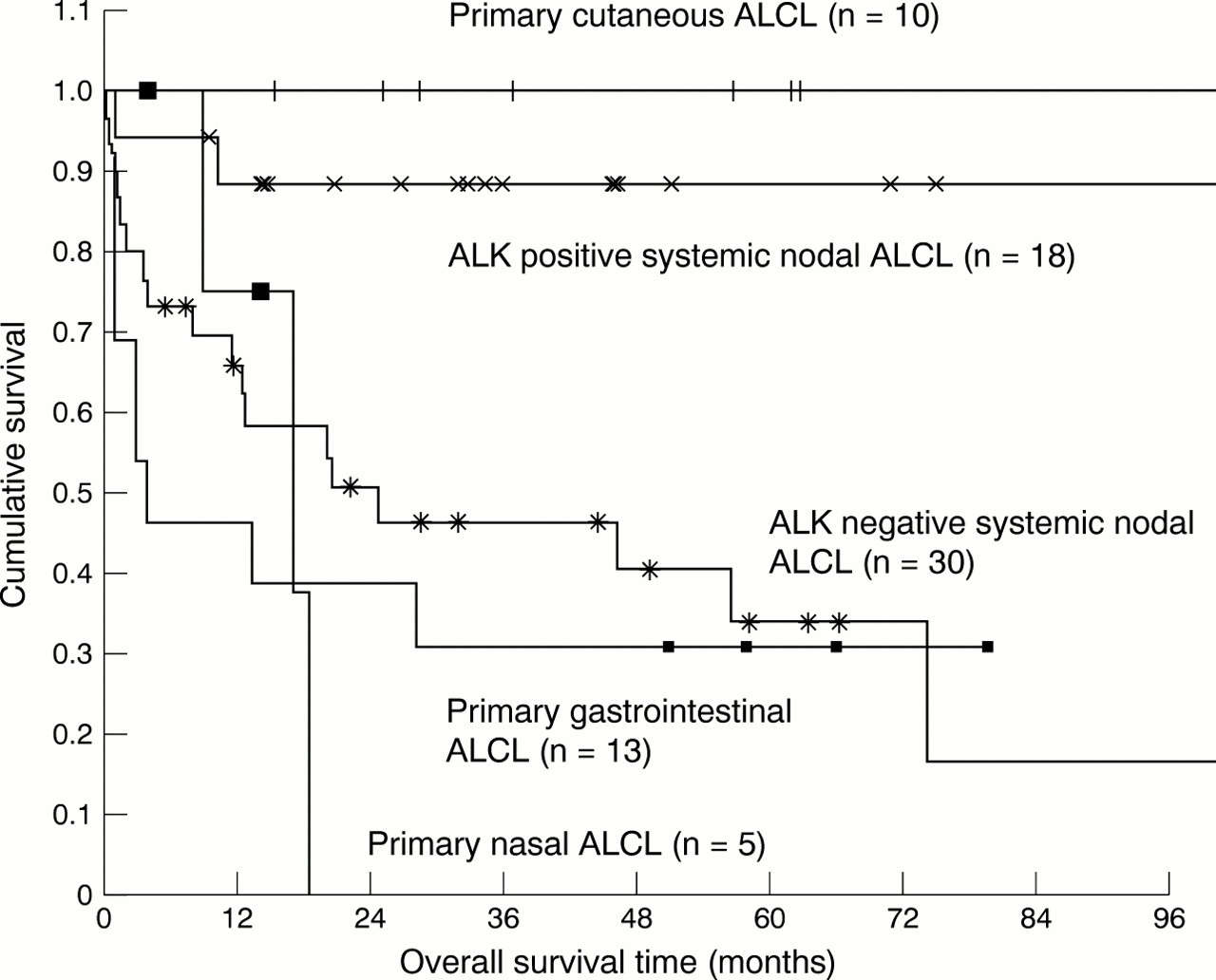
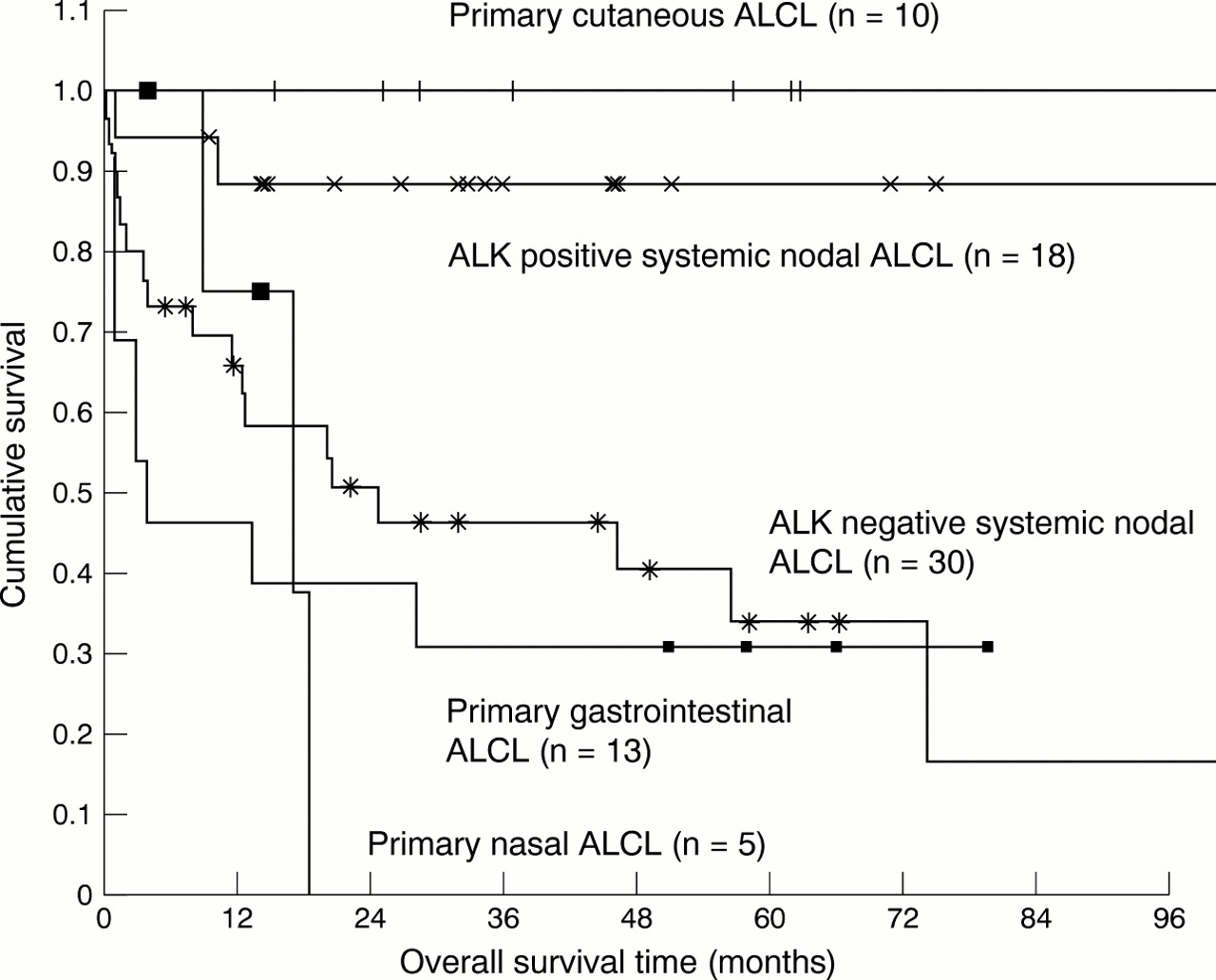
Primary cutaneous ALCL was found to have an excellent prognosis, whereas primary gastrointestinal ALCL showed a five year survival of only 30% (table 3), with more than half the patients dying within one year (fig 4). Patients with primary nasal ALCL showed an expected overall survival of less than two years. Thus, the site of origin was a strong predictor of overall survival time (p = 0.0003) (fig 4). The site of origin was also predictive of progression free survival time, with ALK positive systemic (nodal) ALCL and primary cutaneous ALCL showing better progression free survival time than ALK negative systemic (nodal), primary gastrointestinal, and primary nasal ALCL (p = 0.03).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of overall survival time in anaplastic large cell lymphoma (ALCL), according to primary site of origin and anaplastic lymphoma kinase (ALK) expression.
Because ALK positive (systemic nodal) ALCL showed good prognosis, we compared the clinical behaviour of ALK negative ALCL arising at different sites. ALK negative systemic (nodal) ALCL showed a five year survival of less than 40%, comparable to primary gastrointestinal and primary nasal ALCL (fig 4). When primary cutaneous ALCL was excluded, the site of origin was not predictive of survival in ALK negative ALCL (p = 0.7).
Discussion
We found ALK expression, as determined by immunohistochemistry using the ALK1 and ALKc monoclonal antibodies, in 20 of 51 (39.2%) systemic (nodal) ALCLs. No ALK expression was found in either primary cutaneous ALCL (n = 15), lymphomatoid papulosis (n = 7), primary nasal ALCL (n = 5), or primary gastrointestinal ALCL (n = 14). Our findings indicate that ALK expression in ALCL, if present, favours systemic disease with (primary) nodal involvement.
Expression of the t(2;5) translocation and/or ALK protein in primary extranodal ALCL remains controversial. Previous studies have shown that ALK appears to be expressed exclusively in systemic (nodal) ALCL and not in primary cutaneous ALCL, lymphomatoid papulosis, or primary gastrointestinal ALCL.15,24–26 However, two studies described NPM–ALK transcripts in one of three27 and four of nine28 cutaneous ALCLs using nested RT–PCR analysis with two amplification steps. Because nested RT–PCR analysis is extremely sensitive, false positive results might have occurred. This seems probable in at least one study,27 where the cutaneous case showing amplification with nested RT–PCR failed to stain with the polyclonal anti-ALK antibody p80. In the other study,28 the cases positive for nested RT–PCR showed variable positivity with other detection methods, including p80 immunostaining and ISH. Yet another study29 found positive staining with the antibodies p80 and ALK1 in one of eight cases of primary cutaneous ALCL, but no evidence of ALK expression with standard RT–PCR.
Differentiating between systemic (nodal) and primary extranodal ALCL has consequences for therapeutic strategies. Of peripheral T cell lymphomas, systemic nodal ALCL has been shown to run a relatively favourable clinical course,4 whereas primary gastrointestinal and nasal T cell lymphomas usually show very aggressive behaviour.2,7–9 Indeed, when comparing clinical behaviour between ALCL arising at various sites, the site of origin was found to be strongly predictive of survival, with primary cutaneous ALCL showing excellent survival, whereas primary gastrointestinal and primary nasal ALCL were characterised by poor prognosis, comparable to ALK negative systemic nodal ALCL. Excluding primary cutaneous ALCL, the site of origin was not predictive of survival in ALK negative ALCL. Although the cases studied were relatively few, this suggests that in non-cutaneous ALCL, ALK expression rather than site of origin is important in predicting clinical outcome of the disease. Indeed, ALK expression predisposed to favourable clinical outcome, in accordance with previous studies.19–23 Interestingly, the patient presenting with concurrent intestinal and nodal (ALK positive) ALCL had a favourable clinical outcome, in contrast to primary gastrointestinal or nasal ALCL. Our findings support a growing opinion that ALK positive ALCL seems to be a distinct entity, characterised by good prognosis.
In patients who had multiple biopsies taken at initial diagnosis or who had recurrent disease, ALK expression was found to be consistent for all tumour biopsies—for example, if a patient was diagnosed with ALK positive ALCL, all other tumour biopsies of that patient proved ALK positive, regardless of localisation. For instance, the patient with concurrent intestinal and nodal ALCL showed ALK positivity in both localisations. Another patient with systemic (nodal) ALCL developed cutaneous and nodal relapses, all of which showed ALK expression. Vice versa, if the primary tumour was ALK negative, all other biopsies were found to lack ALK expression as well. The same staining pattern (cytoplasmic and nuclear, or cytoplasmic only) was observed for all biopsies of a given patient. These findings indicate that the chromosomal aberration leading to expression of the ALK protein is an early pathogenic event—before dissemination to other sites. In transfection experiments, ALK has been shown to have transforming abilities in vitro,33,34 and to give rise to large B cell lymphomas in mice,35 but its precise role in the pathogenesis of ALCL remains to be elucidated.
The ALK1 and ALKc monoclonal antibodies gave identical results with regard to presence of staining, and localisation pattern of staining, the only difference being that ALKc showed stronger nuclear staining than ALK1. In 15 of 20 ALK positive cases, staining was observed in both the cytoplasm and nucleus of the tumour cells. In five of 20 cases, staining was restricted to the cytoplasm. This observation has been reported before in independent studies by other groups,11–13,17,30 the hypothesis put forward being that these tumour cells carry translocations other than t(2;5), with the ALK gene linked to a gene other than NPM.
We conclude that ALK expression, if present in an extranodal ALCL site, favours systemic disease with (primary) nodal involvement and a good prognosis. Patients presenting with ALK positive extranodal ALCL should be carefully staged to determine whether lymph nodes are involved. ALK is expressed consistently in multiple and subsequent biopsies of a given patient, indicating that the chromosomal abnormality involving the ALK gene always occurs before dissemination to other sites. Finally, with the exception of a primary skin localisation, ALK negative ALCLs originating from different sites show comparable five year survival of less than 40%. We recommend studies involving larger numbers of patients to confirm these findings.