Article Text

Abstract
Background During the last decade, whole slide images (WSI) have been used in many areas of pathology such as teaching, research, digital archiving, teleconsultation and quality assurance testing. However, WSI have not regularly been used for routine diagnosis, because of the lack of validation studies.
Aim To test the validity of using WSI for primary diagnosis of skin diseases.
Materials and methods 100 skin biopsies and resections which had been diagnosed light microscopically one year previously were scanned at 20× magnification, and rediagnosed by six pathologists (every pathologist assessed his own cases), having the original clinical information available, but blinded to the original diagnoses. The WSI diagnoses were compared to the initial light microscopy diagnosis and classified as concordant, slightly discordant (without clinical consequences) or discordant.
Results The light microscopy and the WSI based diagnosis were concordant in 94% of the cases. The light microscopy and WSI diagnosis were slightly discordant in 6% of the cases. For one of the slightly discrepant cases the WSI diagnosis was considered better, while the original diagnosis was preferred for the other five cases. There were no discordant cases with clinical or prognostic implications.
Conclusion Primary histopathological diagnosis of skin biopsies and resections can be done digitally using WSI.
- Whole slide images
- digital pathology
- dermatopathology
- diagnostics
- validation
- digital pathology
- breast cancer
- cancer research
- breast pathology
- molecular pathology
- gut pathology
- pancreas
- tumour markers
- gastric cancer
- colorectal cancer
- GI neoplasms
- stomach
- breast
- proliferation
- quantitation
- image analysis
- comparative genomic hybridisation
- morphometry
- cell cycle regulation
Statistics from Altmetric.com
- Whole slide images
- digital pathology
- dermatopathology
- diagnostics
- validation
- digital pathology
- breast cancer
- cancer research
- breast pathology
- molecular pathology
- gut pathology
- pancreas
- tumour markers
- gastric cancer
- colorectal cancer
- GI neoplasms
- stomach
- breast
- proliferation
- quantitation
- image analysis
- comparative genomic hybridisation
- morphometry
- cell cycle regulation
Introduction
Whole slide imaging is the process of digitising glass slides by means of a dedicated slide scanner to present the acquired image on a computer screen.1 2 Digital slides or whole slide images (WSI) can be explored by image viewers facilitating tissue examination in a way comparable to a regular microscope, also called virtual microscopy.3 4 However, additional features are often supplied by the image viewers, for example the ability to explore several slides at the same time and an overview image next to the high power view providing more orientation within the slide.5 6 Moreover WSI can be explored simultaneously by multiple viewers from different locations.7 Multiple access of WSI by different users at the same time supports their use for many applications in pathology such as teleconsultation and education. Consultations using WSI will save the time needed for transferring glass slides to remote places for obtaining second opinions. In pathology education, having the opportunity to show all students exactly the same slide has many benefits over handing out consecutive sections.5 8–10 Other pathology applications such as frozen section diagnosis,11 12 quality assurance testing,13 slide conferences and tumour boards5 are examples where WSI can be used efficiently.
Despite the fact that some pilot studies suggest that WSI is as useful as conventional glass slides for rendering diagnosis,14–17 WSI based diagnosis has not been integrated within the routine pathology workflow until now (with a very small number of exceptions). There are several reasons why the use of WSI in daily routine work is still not common, among which are scanning speed, storage capacity (and pricing), software integration and lack of systematic validation studies for their use for primary diagnosis.5 18
Many developments have taken place over the last few years which may help in reducing the impact of some of these issues, for example the tangible reduction of scanning time.2 5 Second, the technique of image acquisition is also improved. Some scanners are able to scan in continuous auto-focusing mode instead of scanning in image stripes or capturing image tiles.1 5 This will minimise the focusing errors within the WSI. Third, suitable navigation instruments (replacing the ordinary computer mouse) for easy and more ergonomic handling of WSI in a way very similar to handling glass slides are also becoming available. Fourth, standardisation according to the DICOM image format (also generally being used for storing images in radiology and radiotherapy imaging modalities) for storing WSI is a big step forward, which will ease the integration and exchange of images between different institutions and systems. Fifth, the increase of storage capacity with reduction of the cost per unit of storage is also expected in the near future, providing the opportunity to store more images for the same price. All of these factors will increase the acceptance of using WSI for primary diagnostics in pathology.
In previous articles we have described the setup of a workflow enabling scanning and archiving all diagnostic slides in the daily routine.1 These digital slides, which are routinely scanned in our laboratory now, are being used for clinicopathological meetings, comparisons with new material (digital archive), education and research. Furthermore, we have reviewed the current status of the field of digital pathology and described our perspective on the future of digital pathology.5 The aim of the present study was to evaluate the suitability of WSI for daily routine digital sign out in dermatopathology, generally a large part of the case mix in diagnostic histopathology.
Materials and methods
This study was performed at the Department of Pathology, University Medical Center Utrecht (UMCU), a medium-sized academic pathology laboratory in The Netherlands. We handle about 144 000 surgical pathology slides (from about 25 000 specimens) and 12 000 cytology slides per year. Since November 2007, scanning was started on a daily basis for all histopathology slides after they had been diagnosed by light microscopy. Scanning is performed on three ScanScope XT scanners (Aperio, Vista, California, USA). The whole process of scanning runs automatically (including selection of the area of the slide that contains tissue, placing focus points, calibration, etc.). Scanning slides of 15×15 mm on 20× took on average 2.5 min. The produced WSI are stored on a dedicated mass storage environment and linked to the pathology report,1 based on the recognised barcode on the slide label. WSI can be accessed through our pathology reporting system (U-DPS, PALGA, Utrecht, The Netherlands), as well as other images, such as gross images and scanned order forms.
One hundred skin biopsies and resections with a complete set of well focused WSI that had been diagnosed light microscopically by six pathologists in 2009 were selected, to guarantee a period of 6–12 months between the first (light microscopic) and the second (WSI based) diagnosis. The same pathologists who did the initial diagnosis were asked to rediagnose their own cases on WSI (the cases are therefore not equally distributed over the six pathologists). The participating pathologists had varying experience using WSI, but at least 3 years' experience.
WSI were presented to the pathologists per case together with the original clinical information, without showing them the original report based on light microscopy examination. The WSI were displayed on standard consumer quality Samsung 245B (Samsung, Seoul, South Korea) displays of 24” (having a resolution of 1920×1200 pixels). The selected cases consisted of 46 biopsies and 54 resection specimens with different entities of skin diseases. Table 1 shows a summary of the number of cases in relation to the type of specimen (either biopsy or resection) and their diagnostic entity.
Type of the specimen (biopsy or resection) and diagnostic category of 100 dermatopathology cases evaluated on whole slide images
At the end of this experiment we have 100 WSI based diagnoses and 100 light microscopy based diagnoses rendered by six pathologists, each on their own cases. The original light microscopy and the WSI based diagnoses were compared by three independent pathologists to judge the concordance of both diagnoses as:
Concordant; complete agreement between the first original signed out diagnosis and the diagnosis as determined on the WSI.
Slightly discrepant; mild differences which would not have any clinical or prognostic implications.
Discrepant; differences with clinical and/or prognostic implications for the patient.
The CIs were calculated and the preferred one of the two diagnoses (light microscopy or WSI based) was also noted.
Results
For 94 of 100 cases (94%) the original light microscopy and WSI based diagnoses were concordant, while the remaining six cases (6%) showed slight discordance between the digital and the light microscopy diagnoses. The percentage agreement between light microscopy and WSI based diagnosis falls within the 95% CI (0.87 to 0.97). Moreover none of these discrepancies were associated with clinical or prognostic implications for the patient. Reassessment of the glass slides and WSI by the reviewing pathologists showed that in one case the WSI diagnosis was preferred over the diagnosis by conventional light microscopy. For the other five cases the original light microscopy diagnosis was considered to be better. Table 2 details these six slightly discrepant cases.
Overview of diagnostic features of six dermatopathology cases showing slight discrepancies when comparing diagnosis on conventional slides and whole slide digital images
The first case concerned a skin biopsy from a patient with previous history of lichen sclerosus and differentiated vulvar intraepithelial neoplasia (VIN), presenting with features of hyperkeratosis. The clinical question was whether there was any evidence of premalignancy. Both the light microscopy and the WSI based diagnosis agreed about the absence of signs of malignancy, but disagreed about the type of lichenoid reaction seen within the biopsy. On WSI it was considered as ‘lichen ruber’, while using light microscopy it had been considered as ‘lichen sclerosus’. After revision of the glass slides and WSI, the diagnosis ‘lichen ruber’ was deemed best. Figure 1 shows a snapshot of the WSI showing the lichenoid inflammation within this vulvar skin biopsy.

Snapshot of whole slide images (WSI) showing lichenoid inflammation within vulvar skin biopsy. This case was misdiagnosed conventionally as ‘lichen sclerosus’ but correctly classified as ‘lichen ruber’ on WSI.
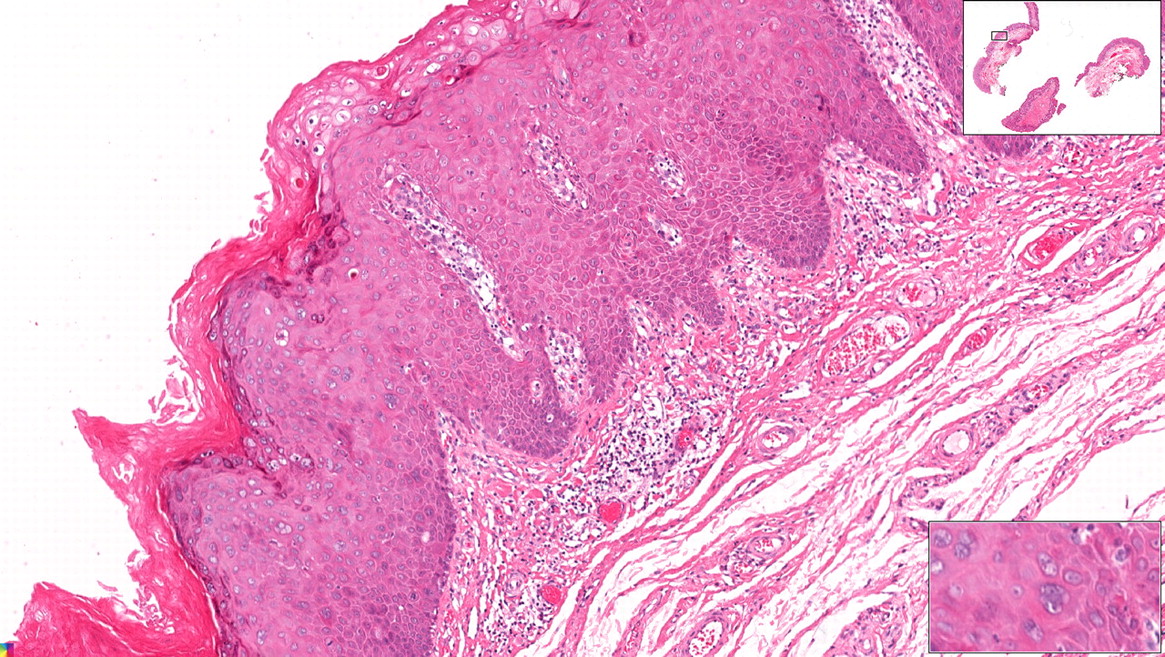
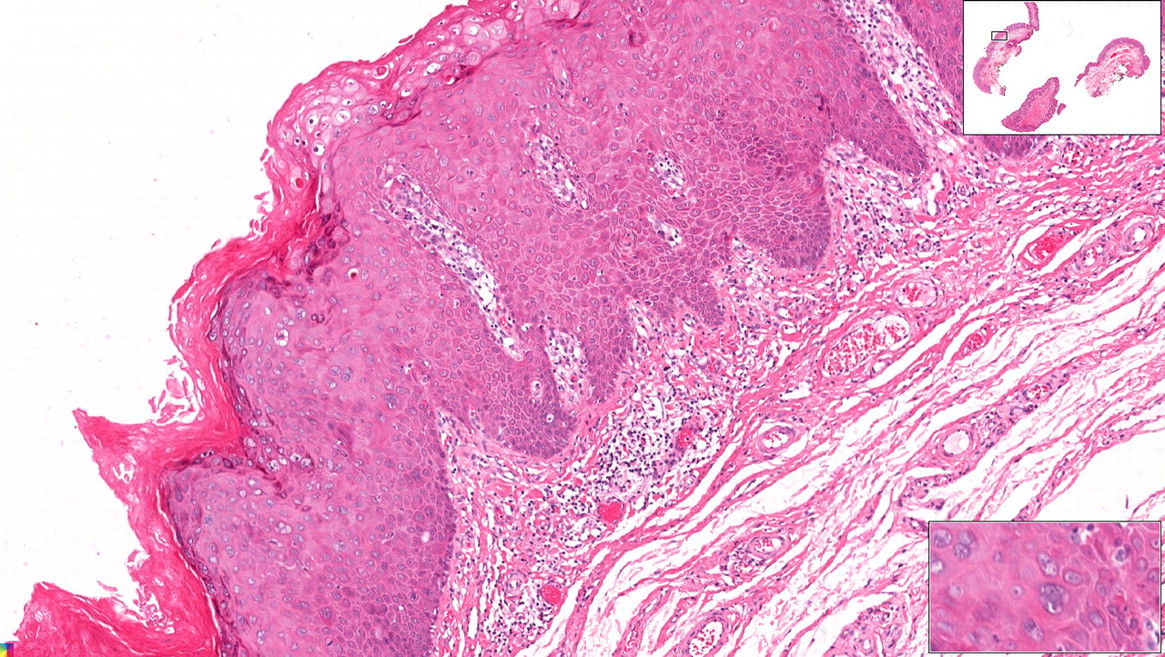
The second slightly discrepant case concerned a skin biopsy of a papule below the nail of the fourth toe. The original light microscopy diagnosis was ‘fibrokeratoma’ while the diagnosis after reviewing the WSI was ‘verruca vulgaris’. After revision, the light microscopy diagnosis was considered to be better. Figure 2 is a snapshot of a part of the WSI showing the microscopic features suggesting fibrokeratoma.

Snapshot of whole slide images (WSI) of skin biopsy showing the microscopic features suggestive of ‘fibrokeratoma’. This case was erroneously classified as ‘verruca vulgaris’ on WSI.
The third case was a skin re-excision assessing the status after resection of melanoma. Both light microscopy and WSI based diagnosis agreed that there was no remnant of melanoma, but additionally a small nevus was detected on light microscopy which had been missed on the WSI. Figure 3 is a snapshot of a section of the WSI showing the overlooked nevus.

Snapshot from whole slide images (WSI) of skin resection showing a small nevocellular nevus in a re-excision specimen for previous melanoma, which was overlooked while performing the diagnosis using WSI.
The fourth case concerned an anal resection with condyloma. The diagnoses on both light microscopy and WSI agreed on the presence of features suggesting viral infection and anal intraepithelial neoplasia (AIN), but the diagnoses disagreed about the grade of the lesion. On light microscopy it was considered as grade II, but it was considered to be grade III on WSI. On review, the reviewing pathologists agreed with the original light microscopy diagnosis. Figure 4 is a snapshot from an area of the WSI of this specimen showing the site of condyloma with AIN II.
Snapshot from whole slide images (WSI) of an anal skin specimen showing a condyloma with AIN II, graded as AIN III on WSI.
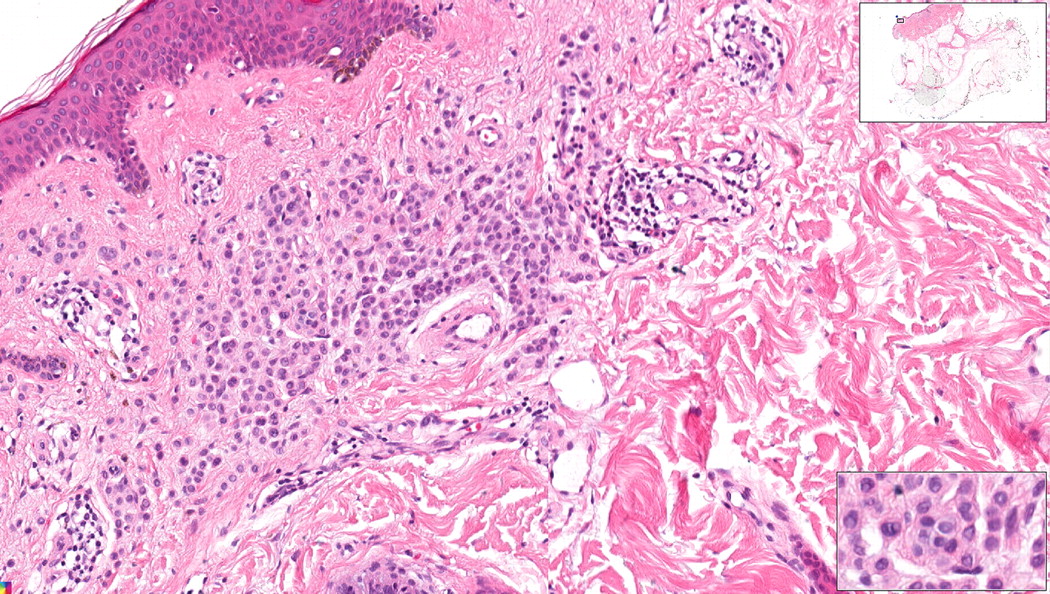
The fifth case concerned a skin resection from the nipple of a patient with a strong family history of malignant melanoma. This skin lesion was diagnosed clinically as ‘nevus’; a biopsy was taken to confirm the benign nature. This lesion had been diagnosed using light microscopy by two pathologists as irritated junctional nevus with the presence of some atypical hyperchromatic melanocytic cells. It was later referred to the Dutch Melanoma Panel who suggested the diagnosis of ‘Spitz nevus’. This resection has been diagnosed as ‘dysplastic nevus’ on WSI. The cause of this discrepancy was not because of the diagnostic method used but because of the interpretation of the pathological changes seen in this difficult lesion. Figure 5 is a snapshot from an area of interest from the WSI of this skin resection.
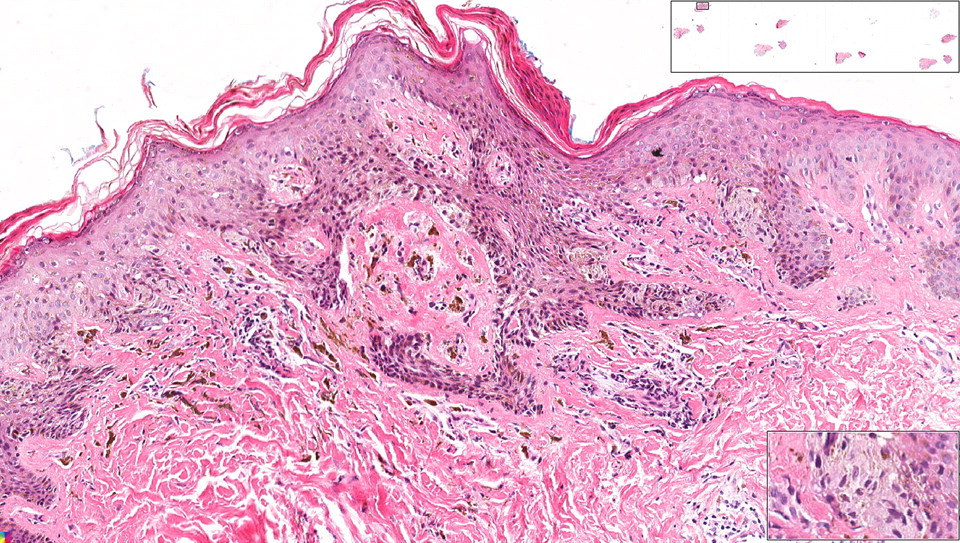
Snapshot from whole slide images (WSI) of a skin resection specimen showing a ‘Spitz nevus’, diagnosed finally as such after consultation with the Dutch Melanoma Panel. Originally, it was deemed an atypical nevocellular nevus. On WSI, it was diagnosed as dysplastic nevus.
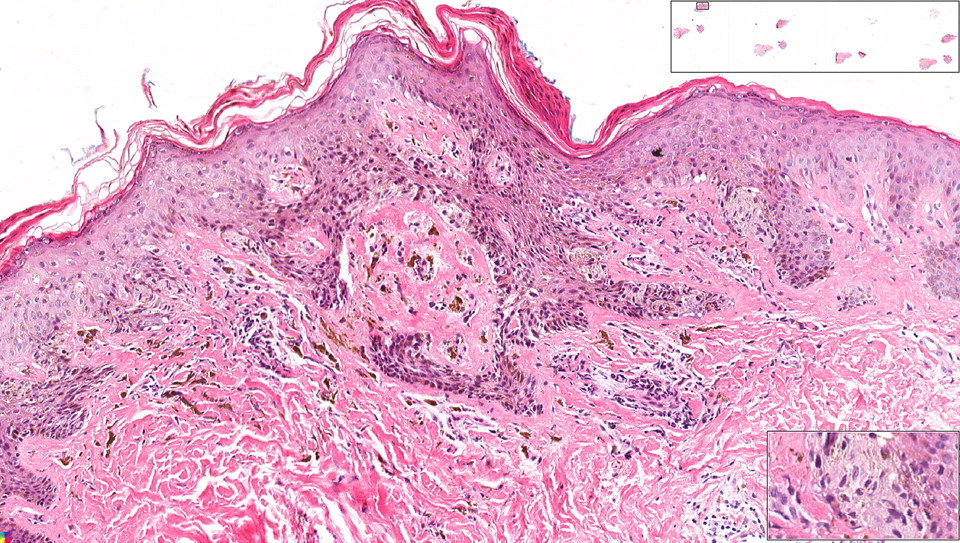
The sixth case was a biopsy of a skin papule. On light microscopy it was diagnosed as ‘benign lichenoid keratosis’ while it was diagnosed as ‘eczema’ on the WSI. Revision of the clinical presentation and the pathological changes supported the original diagnosis. Figure 6 is a snapshot from an area from the WSI of this skin biopsy showing the microscopic features of the lesion.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Snapshot from whole slide images (WSI) of a skin biopsy showing ‘benign lichenoid keratosis’, misdiagnosed as ‘eczema’ on WSI.
Discussion
The aim of this study was to test the feasibility of using WSI for the diagnosis of skin specimens. From the archive we selected 100 skin biopsies and resections received in 2009 which were blindly rediagnosed using WSI (only clinical information was presented) at 20× magnification. The rediagnosis was done by the same pathologist who did the initial diagnosis to avoid inter-observer variations. The rediagnoses were concordant with the original conventional diagnosis in 94% of cases. Interestingly, this is irrespective of the fact that pathologists would have used the 40× magnification on and off during the original diagnostic process, as no restrictions applied at the time. The remaining 6% (three biopsies and three resections) were slightly discordant, without clinical or prognostic implications. This indicates that WSI may well be used for performing primary histopathological diagnosis of skin specimens. This is supported by the high percentage agreement between the diagnoses performed by the two diagnostic modalities and the narrow CI (0.87 to 0.97). The sample size is sufficient, since theoretically the CI would not get much narrower if we even doubled the sample size (0.91 to 0.97).
We consider this rate of mild discrepancies within the range of generally observed intra-observer variability in pathology19 20; a similar rate of discrepancies would likely be seen if cases were rediagnosed microscopically instead of using digital slides. The discrepancy rate is in line with the fact that for one of the six slightly discrepant cases the WSI was in the end considered to be the better one. Additionally, none of the discrepancies was related to the perceived magnification or WSI quality, but mostly to different interpretation of difficult or borderline cases. In two of the cases, overlooking diagnostically important areas was the cause of discrepancy. In one case, overlooking one of the skin fragments present on the WSI led to missing the correct diagnosis, while in the other case, overlooking a small area in one slide from a series of 13 WSI led to the discrepancy. This may be related to the lack of experience in reviewing WSI.
The 94% concordance rate is within the range of other validation studies which examined the performance of using WSI for primary or secondary histopathological diagnosis.21–24 These results are also comparable to the other validation studies which were specific to skin pathology.14 25–27 Okada et al and Leinweber et al assessed the diagnostic accuracy of WSI based teledermatology. Their studies showed a high concordance rate between diagnoses based on WSI and diagnoses based on light microscopy. However, these latter two studies focused only on the diagnosis of melanocytic tumours.25 26 In a study by Gilbertson et al, assessing the validity of WSI diagnosis in 25 genitourinary and dermatology specimens, it was concluded that WSI produced by current slide scanners contain sufficient information for rendering diagnosis. A limitations of that study is the low number of cases and the fact that some WSI with focal areas of poor image quality were included, which were responsible for some discrepant results.27 The validity of using WSI for routine diagnosis of skin tumours was studied by Nielsen et al on 96 skin biopsies and shaves, from which one glass slide was created for each case. The participating pathologists diagnosed the first on WSI and after a few weeks by light microscopy. Then they compared the two new diagnoses with the gold standard diagnosis from a highly experienced dermatopathologist. The diagnostic accuracy was 89.2% and 92.7% for WSI and glass slides, respectively. The limitation of this study is that the participating pathologists were blinded to the clinical information which could affect the diagnostic outcome and also none of them had previous experience with using WSI. In addition, the short time period between performing the diagnosis by the two modalities was another limitation, since pathologists may have remembered the cases.14
During digital evaluation, the pathologists did not have many difficulties in rendering the diagnosis at the applied 20× magnification. The fact that we checked the quality of all WSI (and rescanned when necessary) before showing them to the pathologists may have helped here. When routinely using WSI for primary diagnostics one would also demand adequate quality of the scanned slides for a confident diagnosis. Scanning at higher magnification may be preferable in general to avoid any possible issues related to the lack of resolution, and routinely scanning at 40× will become possible in the near future when scanners are faster and storage price has come down. On the other hand, a higher magnification seems not to be relevant for most cases, and for now saves scanning time and storage requirements.
Despite advantages of WSI and the fact that the participating pathologists were comfortable using WSI, most of them still prefer to view slides under the microscope. This may be due to the fact that the WSI based diagnostic process was perceived to be slower (although no formal timing was performed) and a mouse may not be optimally suitable as a navigation tool for examining WSI. Devices allowing easier handling of WSI during diagnosis are currently available, such as the Ergo Controller (Nikon) or the iSlide input device (BioImagene), although they are specific for use together with image viewers specific for the slide scanners from these vendors. These devices assist the pathologists to view the WSI in a way more comparable to the conventional light microscope, which may minimise errors resulting from improper navigation of WSI. Also better monitors with resolutions up to 6 megapixels, having a very small picture pitch and with sRGB calibrated colours (like the ones used in radiology) will help, but current viewers first need to be optimised to handle these high resolutions.
A potential advantage of WSI is that it becomes possible to perform image analysis and eventually also computer assisted diagnosis, possibly improving the diagnosis and decreasing inter-observer variability. This may also assist in the objective diagnosis of aggressive skin tumours such as malignant melanoma.28–30 Tissue counter analysis of dermatoscopic31 and microscopic images has been investigated for differentiation of molluscum contagiosum from normal skin and also for classification of melanocytic skin tumour with acceptable results.32–35 In another study on malignant melanomas and its correlation with patient survival, the authors concluded that automated measurement of cross-sectional areas of malignant melanoma on digital slides can help in assessing patient prognosis.36
Some legal issues arise from the use of WSI for primary diagnosis, related to image quality, image presentation (monitor quality), storage space, adequate backup, document transfer, patient confidentiality and the confidence of the pathologist to sign-out a pathology report depending on WSI. We expect that most of these issues will be settled in the near future. Several digital pathology vendors are currently seeking approval from the US Food and Drug Administration (FDA) for using WSI in primary diagnosis, which will definitely encourage the general use of WSI in primary diagnostics after conditions for the above issues have been defined. One aspect of FDA approval is systematic validation of WSI for primary diagnosis in sufficient sized populations, as this study does for skin tissue. In Europe, the Royal College of Pathologists in its August 2003 guidelines, ‘Code of practice for pathologists participating in remote reporting of histopathology or cytopathology’, declared the necessity of remote reporting services, especially when no regional pathologist is available. However, the remote pathologist should take into consideration that all the necessary data (clinical, laboratory feedback, contact with clinician) are available to guarantee a good quality of the pathology report (http://www.rcpath.org/resources/pdf/FINALREMOTEREPORTINGOFHISTCYTOonweb.pdf). This issue has been also reported in its guidelines for the year 2005, where it was stated that: ‘The conclusions of that report are relevant whether the remote reporting is achieved by transfer of microscopic slides or by telepathology’ (http://www.rcpath.org/resources/pdf/G026-Telepathology-May05.pdf).
The Dutch Society of Pathology already considers WSI an alternative for stored glass slides (http://www.pathology.nl/nvvp/nvvpcms3.nsf/uploads/FE035749A30F70BEC125775B0031BC5D/$FILE/Advies%20bewaartermijnen%20definitief.pdf). In September 2010 an extension to the DICOM file format has been accepted by the DICOM committee to support storage and exchange of WSI, which is an important development in the field of digital pathology.5 Further systematic validations in addition to solving some practical issues will help the adoption of WSI for primary pathology diagnosis.
WSI diagnosis did not have a major clinical impact in the current study in terms of patient management, and we feel that the discrepancies between conventional and WSI based diagnosis are within the ranges of generally inter- and even intra-observer variation. Therefore, we do not expect WSI based diagnosis to affect cancer registries and incidence rates in general.
In conclusion, it seems that primary histopathological diagnosis of skin biopsies and resections can well be done on WSI acquired using today's scanning technology.
Take-home messages
Up front histopathological diagnosis of routine skin biopsies and resections is feasible on whole slide images (WSI) acquired using today's scanning technology.
More and more facilities are acquiring WSI that support their use in routine daily practice as well as other pathology applications. A major property of WSI is that they can be shared by different examiners from different places, supporting their use for quality assurance, primary and secondary teleconsultation, etc.
The use of WSI for education of undergraduates and postgraduates has been increasing in recent years.
Further progress in image analysis and computer aided diagnosis of WSI will open new ways for less subjective diagnosis in histopathology.
Acknowledgments
We thank Dr Roxana Ion, Philips Digital Pathology, Eindhoven, The Netherlands, for help with statistics.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.