Article Text

Abstract
Introduction Whole slide images (WSI) have been used in many pathology applications such as teleconsultation, teaching and research, but not in primary diagnostics. The aim of this study was to test the feasibility of using WSI in primary diagnostics of paediatric pathology specimens and placental tissue.
Materials and methods Eighty consecutive tissues biopsies and resections from patients under 18 years old were selected, as well as 20 placentas. These cases had been diagnosed in the year 2009 by a single pathologist. The same pathologist who had performed the original diagnosis based on light microscopy was asked to rediagnose these 100 cases on WSI scanned at 20× magnification as well as by light microscopy having the original clinical information available, but blinded to the original light microscopic diagnoses. The original diagnoses were compared with WSI based diagnoses and rediagnoses by light microscopy and classified as concordant, mildly discordant (without clinical consequences) and discordant (with clinical consequences).
Results The original diagnoses were concordant with WSI and light microscopic diagnoses in 90% and 93% of cases respectively, which was not significantly different. Digital reassessment yielded eight mild discrepancies and two discrepant cases (2%) where the difference in diagnoses could have clinical implications for the patient. Light microscopic reassessment showed seven mild discrepancies. It turned out to be difficult to identify nucleated red blood cells on WSI, even when scanned at 40×.
Conclusions Primary diagnostics of paediatric tissue biopsies and resections can generally well be done on WSI. However, some difficulties were encountered in examining placenta tissue where the identification of nucleated red blood cells may need higher resolution or even scanning at multiple focus depths, which is well possible on most current slide scanners.
- Paediatric Pathology
- Digital Pathology
- Diagnostics
- Histopathology
Statistics from Altmetric.com
Introduction
Imaging technology has revolutionised the field of pathology by the introduction of new ways of tissue examination and rendering diagnosis.1 ,2 This is achieved by automatic digitisation of the complete glass slides, producing what is commonly referred to as Digital Slides or Whole Slides Images (WSI). The current technology allows the examination of tissue section on a computer screen by the aid of viewers enabling the examination of the complete slide in a way comparable to conventional microscopy, navigating through the slide in any direction and at varying magnifications.3–5 Exploration of the same digital slide by multiple examiners from different locations, examination of multiple slides at the same time (allowing side-by-side comparison of different staining of the same specimen), the presence of an overview image facilitating the navigation within the digital slides, easy integration of annotations into WSI are all supplementary features provided by image viewers.1 ,3 ,6 The aforementioned criteria have supported the use of WSI in different applications in pathology for example, remote consultations, primary frozen section diagnosis, quality assurance, education and research.1 ,7–11 However, WSI for upfront diagnostics are the least practised application of digital pathology. Nevertheless, they have been used for upfront diagnostics in some laboratories after performing their local validation studies, for example, in Atrium Medical Center Heerlen, Heerlen, The Netherlands12 and Kalmar County Hospital, Kalmar, Sweden.13
The integration of WSI for daily routine diagnostics is accompanied by many challenges such as controlling image quality, standardisation of image storage and retrieval, integration of WSI into software systems in place and legal aspects, which are crucial issues that need to be discussed before WSI for primary diagnostics become common practise in pathology. Moreover, WSI have not been approved yet by the Food and Drug Administration (FDA) for primary diagnostics. Gaining FDA approval will definitely encourage the general use of WSI for upfront diagnostics, especially in the USA, but it may also warrant extensive validation studies to test the feasibility of WSI for this purpose, especially because the FDA has classified whole slide scanners as Class III medical devices (Slide scanner classification).
The aim of the present study was to evaluate the use of WSI for upfront diagnostics of placental tissue, and biopsies and resection from different body systems of patients under 18 years of age. To our knowledge this is the first article examining the validity of WSI for upfront diagnostics in paediatric pathology. This study is part of a large project aimed for systematic validation of WSI for upfront diagnostics in different areas of pathology.14–16
This study has been conducted in the Department of Pathology, University Medical Center Utrecht, a medium sized academic pathology laboratory in The Netherlands handling about 144 000 surgical pathology and 12 000 cytology slides each year. Since November 2007, all histopathology slides have routinely been scanned after they had been diagnosed on a light microscope. Scanning is performed on ScanScope XT scanners (Aperio, Vista, California, USA). The produced WSI are stored on a dedicated mass storage environment and linked to the pathology report, based on the recognised barcode on the slide label.
Primary paediatric pathology diagnostics on WSI
For the first part of this study 80 consecutive tissues (67 biopsies and 13 resections) from patients under 18 years and 20 placentas with a complete set of well focused WSI (20× magnification) were selected. These cases had been diagnosed by light microscopy by one pathologist in 2009. The same pathologist who did the original diagnosis was asked to rediagnose his own cases blinded to the original diagnosis on two other occasions; first digitally and then microscopically. The wash out time between rendering diagnosis by each modality was more than 1 year. Table 1 gives an overview of the anatomical site and the specimen type of the 100 cases included in this study.
Overview of the anatomical site and the specimen type of 100 paediatric pathology cases rediagnosed on WSI
Digital and new microscopic diagnoses were compared with the original diagnoses by three independent pathologists and categorised as in our previous articles into:14–16:
-
Concordant; complete agreement between the original diagnosis and second diagnoses (digital and microscopic)
-
Mildly discrepant; mild differences between original and second diagnoses (digital and microscopic) which would not have any clinical or prognostic implications
-
Discrepant; differences with clinical and/or prognostic implications for the patient
-
The percentage agreement, 95% CI and the level of significance (using Fisher's exact test) was calculated using SPSS software.
Identification of nucleated red blood cells on WSI
The second part of the study tested if the identification of nucleated red blood cells (NRBCs) in placental WSI scanned at 40× would work better than on 20×, which was found to be difficult in the first part. Six months after the 20× digital diagnosis, the placenta cases were presented for the second time to the same pathologist to be examined by light microscopy first and 3 months later on WSI scanned at 40×. The pathologist was asked only to note the presence or absence of NRBCs; for which the light microscopic and 40× digital diagnoses were compared.
Results
Primary diagnostics on WSI
WSI based diagnoses and microscopic diagnoses were concordant with the original diagnoses in 90% (95% CI 0.84 to 0.96), 93% (95% CI 0.88 to 0.98) of cases respectively (p=0.144).
Digitally there were 10 discrepancies, 8 (8%) of them showed mild discordance between digital and original diagnoses without clinical or prognostic implications for the patient. However, in two cases (2%) the difference in the diagnosis could be associated with clinical implications. Only seven mild discrepancies were seen between original and second light microscopic diagnoses. Table 2 shows the rates of concordance between digital, microscopic and original diagnosis in different body systems.
Overview of discrepancies between original light microscopy based diagnosis and digital rediagnosis on WSI of paediatric pathology cases
Out of 100 cases, there were about 66 cases from different regions of the gastrointestinal tract for which WSI based diagnosis and light microscopic diagnoses were concordant with the original diagnosis in 93.9% (62/66, CI 0.88% to 0.99%) and 98% (65/66, CI 0.95% to 1.0%) of cases, respectively.
Digitally there were four discrepancies between original and WSI based diagnosis. Two of them (cases 1, 2, table 3) were mild while the other two (cases 3, 4, table 3) were discrepant with potential effects on the patient. Case number 3 concerned a biopsy from the rectum. The clinical history in this case was suggestive of M. Hirschsprung. The report from WSI confirmed the absence of ganglion cells and presence of hyperplastic nerve tissue bundles in three stains (hematoxylin and eosin stain, acetylcholinesterase, succinic dehydrogenase) but the presence of one ganglion cell was suspected on the Nicotine Amide Diamine Hydrogenase stained slide. Based on the latter stain the diagnosis Morbus Hirschsprung was rejected. This case had been diagnosed before as Morbus Hirschsprung on light microscopy. On revision, the light microscopy diagnosis was deemed the better one. The other case (case 4) concerned a small intestinal resection. The light microscopy diagnosis was ‘Small intestinal resection with perforation and ulceration with evidence of candidiasis’ while WSI based diagnosis was ‘Mild reactive changes with ischaemia, ulceration and necrosis. No candidiasis’. On revision, Candidiasis turned out to have been missed while performing the digital diagnosis. Figure 1 is a snapshot from an area of the WSI from this resection showing the site with Candidiasis.
Original and WSI based diagnosis of the 10 discrepant cases digitally.

Snapshot from an area of the whole slide images (WSI) from small bowel resection showing the site of Candida infection (green arrows) which was missed on WSI based diagnosis. This figure is only reproduced in colour in the online version.
Light microscopically there was only single mild discrepancy where the microscopic descriptions were similar but the final interpretation differed. Table 4 details the discrepancies between original and light microscopic diagnoses.
Original and light microscopic diagnosis of the light microscopically discrepant cases
A lower concordance rate (70%, CI 0.48 to 0.92) between original, WSI based diagnoses and microscopic diagnoses was encountered in the placenta cases. Out of the 20 placenta cases included in this study, there were six mild discrepancies (digitally and microscopically) where the pathologist missed the presence of inflammation either in the villi, chorion or umbilical cord. These discrepancies were mild without any further effect on patient treatment and prognosis (tables 3 and 4).
In cases from the skin, tonsil, genitourinary and respiratory system there was 100% agreement between the original and the second diagnoses (digital and microscopic) (table 2).
In further analysis by side-by-side comparison of glass slides and WSI of the 10 discrepant cases, nine original diagnoses were considered better and in one case the WSI diagnosis was deemed the better one (table 3)
Identification of NRBCs on WSI
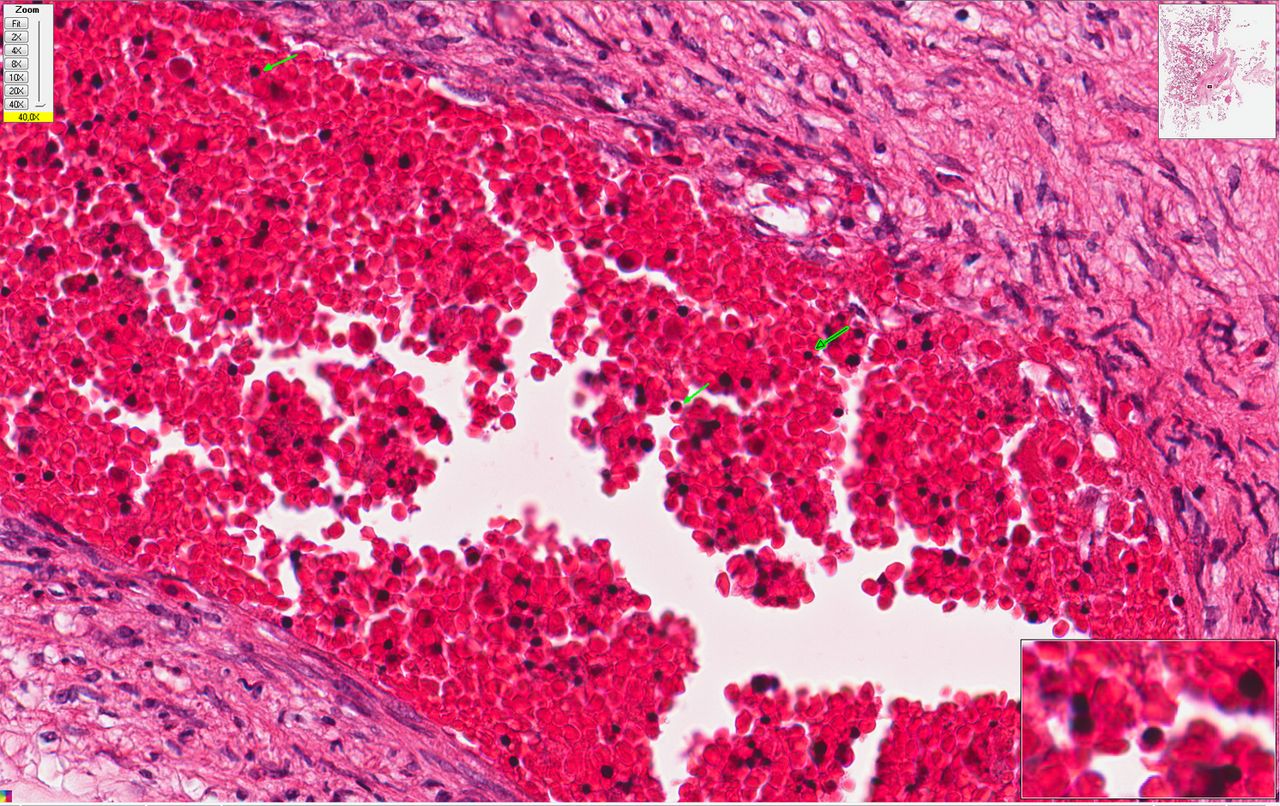
For the second part of the study with 40× digital placenta sections, 16/20 cases were positive for NRBCs by light microscopy and four cases were negative for NRBCs. On WSI, the pathologist reported 10 cases as positive for NRBCs and three cases as negative for NRBCs, while in seven cases the pathologist could not confidently give a diagnosis. WSI diagnoses in regard to NRBCs were thus concordant with light microscopy diagnosis in only 65% of the cases (CI 0.42 to 0.88). Figure 2 is a snapshot of WSI from placenta section showing nucleated RBCs.

{kind=link}
{kind=link}
Snapshot of whole slide images from placenta section showing nucleated RBCs (green arrows). This figure is only reproduced in colour in the online version.
Discussion
The aim of this study was to test the validity of WSI for primary diagnostics of paediatric pathology. WSI based and light microscopic rediagnoses were concordant with the original diagnosis in 90% and 93% of cases, respectively, which was not significantly different. There was a mild discrepancy between original and WSI based diagnoses in 8% of cases without clinical or prognostic implications for the patient, and 2% discrepant cases where the difference in the diagnosis could affect patient treatment and prognosis. All of the discrepancies in the second round of light microscopy were mild without clinical implication for the patient. We would therefore consider the WSI discrepancy rate to fall within the range of the intraobserver variability in light microscopic pathology as shown in the present study and by others.17 ,18 The 90% concordance rate between the original and WSI based diagnoses is also within the range of that in several other validation studies which examined the performance of the WSI for primary or secondary histopathological diagnosis.19–24 In line with this, for one case the WSI based diagnosis was even considered to be the better one.
Digitally, there were two discrepant cases with clinical implication to the patient. In case 3 (see table 3), the pathologist rejected the diagnosis of Morbus Hirschsprung because of the suspected presence of one ganglion cell in one stain. In routine practise, if the pathologist is not sure about the diagnosis of Morbus Hirschsprung and clinical features are suggestive of the disease, contact between the pathologist and the paediatrician should take place to make a plan to arrive at a more certain diagnosis. However, such contact was missing within the research context described in this paper. We assume that if WSI are adopted in the routine work, the same working standards for routine pathological diagnosis based on conventional microscopy will be adopted. This fact has been supported by the Royal College of Pathologists in their 2003 guidelines ‘Code of practise for pathologists participating in remote reporting of histopathology or cytopathology’. In this report, it has been stated that the remote pathologist should take into consideration that all the necessary data (clinical, laboratory feedback, contact with clinician) are available to guarantee a good quality of the pathology report irrespective of the diagnostic modality (whether based on glass slides or telepathology system) (Remote reporting pdf).
The identification of microorganisms like Candida albicans, Helicobacter pylori and Giardia lamblia was sometimes difficult. Scanning at 40× magnification would probably have given a more confident diagnosis of microorganisms. Scanning at higher magnification may therefore be preferable and will likely be the future standard, but appears not to be very relevant for most cases while adding scanning time and necessitating significantly more storage. Missing microorganisms happened in only one case in the present study where the pathologist was not sure about the presence of microorganisms (case 4; table 3) which resulted in a discrepant diagnosis.
A high concordance rate of 100% was seen in cases from skin, tonsils, genitourinary and respiratory system. The number of cases for these systems was however low which could be a limitation of the present study.
Digital diagnosis of cases from the placenta was slightly problematic. First, exploration of placental WSI was felt to be more time consuming than light microscopy, although no formal time measurements were performed. This might be related to the fact that a computer mouse is not the optimal tool for exploring WSI. Presenting WSI on a multi-touch screen of high resolution probably with horizontal format (SurfaceSlide)25 where navigating WSI is allowed in a simple and intuitive way may lead to better and faster exploration of WSI. Comparable solutions are available like Ergo Controller (Nikon) and iSlide input device (BioImagene). Second, placental sections require careful search for inflammatory cells and NRBC in addition to other possible abnormalities which was shown to be easier under the microscope. In the present study, the pathologist indeed missed the inflammation either in the umbilical cord or in the villi or chorion in a few cases on WSI, but similar discrepancies were also seen when rediagnosing light microscopically (table 4). Using advanced image viewers that aid in better image presentation or assist in tracking the examined areas may aid in better digital diagnostic outcomes. Third, WSI scanned at 20× were insufficient for the identification of NRBCs in placental slides. Thus, it was decided to rescan the placenta slides at 40× magnifications to test if a higher magnification helped, and this indeed worked for some cases of the placenta with low density of erythrocytes in the vessels. However, in 7/20 cases the pathologist could still not reliably establish the presence or absence of NRBCs due to thick preparations with cells crowding in vessels. Scanning at multiple focus levels as some scanners allow may further facilitate more confident diagnosis of NRBCs.26 However, such technology will cost more storage and scanning time, which is for the time being inconvenient for routine diagnostics.27 Running image analysis algorithms in the background to identify inflammatory cells, NRBCs and/or microorganisms in scanned tissue sections before being presented to the pathologist will definitely help in increasing the productivity and accuracy of pathology reports.
In conclusion, histopathological diagnosis of biopsies and resections can generally be done well on WSI acquired using today's scanning technology. However WSI scanned at 20× magnification were not optimal for exploring placental tissue. A higher resolution may be necessary for more confident identification of NRBCs and inflammatory cells in placental tissue, and also multilayer scanning may be required in some cases.
Take home messages
-
Upfront diagnosis of paediatric biopsies and resections can generally be done well on WSI acquired using today's scanning technology
-
Scanning slide on 20× were insufficient for identification of nucleated RBCs in placenta sections. Scanning on higher resolutions (40×) could provide confident diagnosis in 65% of the cases. However scanning at multiple levels is still required for some cases for more satisfactory results.
-
The availability of scanners which are able to scan on higher resolution at high speed and the presence of optimal user interface that allow easier and faster exploration of WSI, would definitely help in better acceptance of WSI in daily diagnostics.
-
Further progress in image analysis, computer aided diagnosis and 3D reconstruction of WSI will open new ways for less subjective diagnosis making in histopathology.
Interactive multiple choice questions
This JCP review article has an accompanying set of multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://jcp.bmj.com/education. Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into JCP with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
Footnotes
-
Contributors The plan of this project was suggested by PJvD. The basic data, access to the WSI archive, related clinical patient information and making use of special software for creation of the rediagnosis lists were all arranged by AH. Case selection, controlling WSI quality, rescanning glass slides, arranging rediagnosis sessions based on WSI and light microscopy and finally arranging sessions for interpreting the preferred diagnosis were performed by SAJ. During these rediagnosis sessions PGJN was asked to give the pathological description of the lesion and the final diagnosis. The comparison of the original light microscopy diagnoses with the second diagnoses (digital and microscopic) and reassessing the glass slides and WSI of the discrepant cases for assigning the best diagnosis were performed by FJWtK, PGJN and PJvD. Literature search was performed by SAJ as well as the primary formulation of the article. This article has been reviewed by all participating authors. All authors have substantially contributed to writing, reading and approving the final manuscript.
-
Funding None.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.