Article Text

Abstract
Aim An audit of serrated polyps diagnosed over a 4-year period: 2009 to 2012 was undertaken to ascertain the reporting trends of sessile serrated polyps (SSP).
Methods All right sided hyperplastic polyps (HP) proximal to the splenic flexure and all polyps designated SSP were retrieved from the study period. Three pathologists blinded to the original diagnosis re-examined the slides. Recent American College of Gastroenterology guidelines for the diagnosis of SSP was utilised.
Results No cases of SSP were diagnosed in 2009. In 2010, 32 right-sided cases were encountered, 83 confirmed in 2011 and 134 confirmed in 2012. The vast majority of these were right-sided.
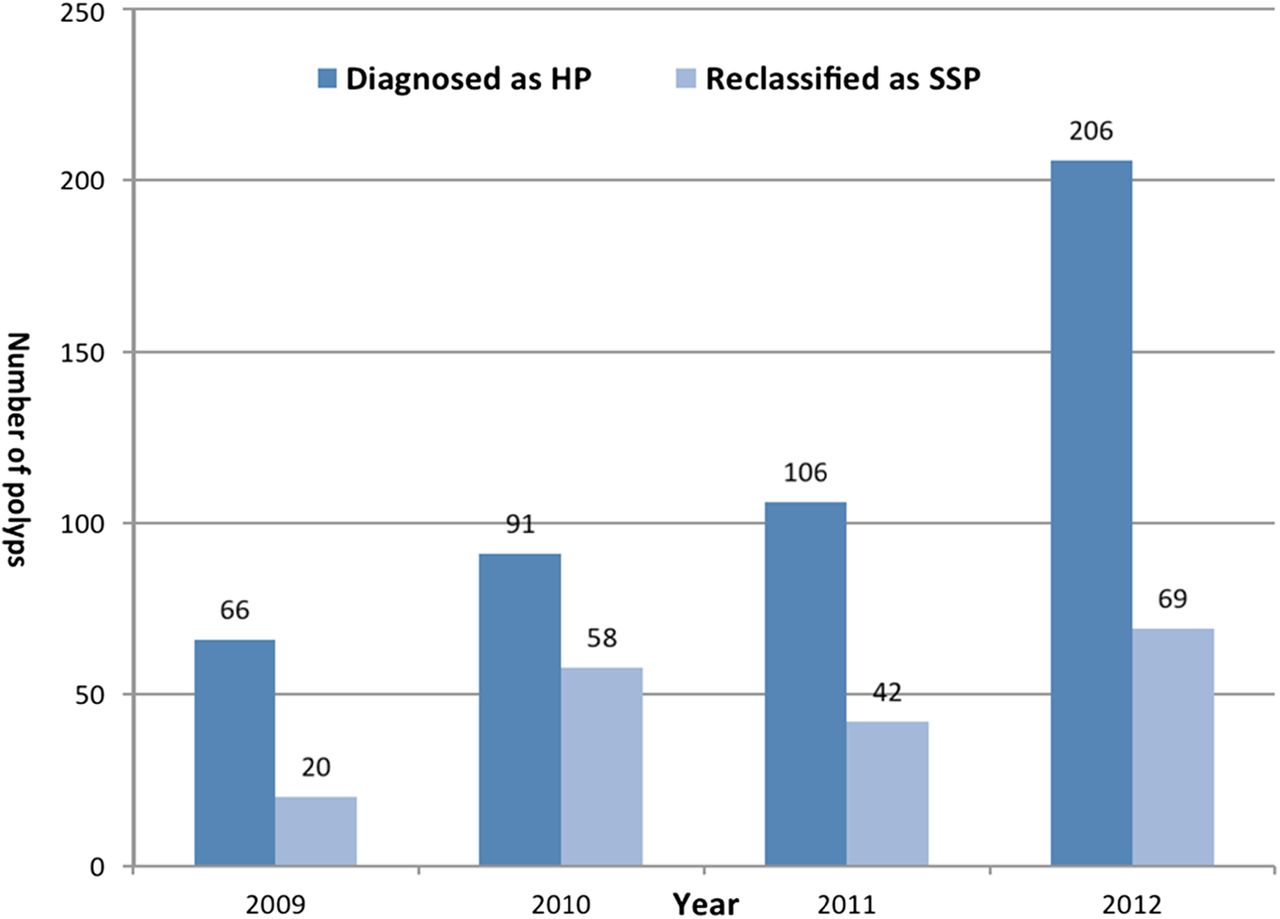
With regards to right-sided HP that were re-classified as SSP the data is as follows: 20 of 66 in 2009 (30%); 58 of 91 in 2010 (64%); 42 of 106 (40%) in 2011 and 69 of 206 in 2012 (33%).
Conclusions This study has demonstrated an almost exponential increase in the diagnosis of SSP over a 4-year period. In addition, 30 to 64% of right-sided HP were re-classified as SSP over the 4-year period suggesting that greater awareness of the diagnostic criteria for SSP is required.
SSP is an important precursor lesion in the serrated pathway of colorectal cancer. Its recognition is important for surveillance and therapeutic strategies.
- GASTROINTESTINAL DISEASE
- COLORECTAL CANCER
- AUDIT
Statistics from Altmetric.com
It is now well accepted that colorectal cancers evolve through distinct molecular pathways. The serrated pathway to carcinogenesis has been recognised as resulting in so-called serrated adenocarcinomas, which account for up to 7.5% of all colorectal cancers.1 Conventional adenomas are regarded as precursor lesions to colorectal adenocarcinoma via the chromosomal instability pathway. Similarly, serrated polyps, especially sessile serrated polyps or adenomas (SSPs/As), are thought to be precursor lesions in the serrated carcinogenesis pathway.
Screening programmes have been introduced in several cancers to detect early lesions, thus ensuring early, pre-emptive, and hopefully, curative treatment strategies to be employed. In addition to bowel cancer-screening initiatives, endoscopy has evolved to the extent that small precursor lesions can now be removed readily, thereby reducing morbidity later. SSP/A have been increasingly recognised over the last 5–8 years by pathologists and gastroenterologists worldwide, especially in North America.
The purpose of this study was to explore the extent to which SSPs/As have been recognised and diagnosed correctly over a 4-year period (2009–2012 inclusive) in an academic teaching hospital encountering a large number of gastrointestinal biopsies.
Materials and methods
A search of the computerised records of the Department of Cellular Pathology, Oxford University Hospitals, Oxford, UK, for all lesions diagnosed as SSP using a natural language search option, was performed. In addition, a search for all lesions diagnosed and coded as hyperplastic polyps (HPs) proximal to the splenic flexure was undertaken using both the natural language and SNOMED coding options. All slides from the relevant cases were retrieved and reviewed, initially, by two pathologists (RC and PG). Randomly selected and/or contentious cases were reviewed, independently, by a third pathologist (LMW). Consensus was obtained in contentious cases by discussion among the three pathologists.
For a diagnosis of SSP/A, the recent guidelines recommended by the American College of Gastroenterology were employed.2 This panel of experts regarded even ‘a single unequivocal architecturally distorted, dilated, and/or horizontally branched crypts, particularly if it is associated with inverted maturation, is sufficient for a diagnosis of SSA/P’.2 This was supplemented by the histological criteria recommended by the WHO for the diagnosis of SSP/A.3
All cases of SSP/A (diagnosed anywhere in the large bowel) and HP proximal to the splenic flexure were evaluated using the above criteria. Those cases not fulfilling the minimum criteria unequivocally were not classified as SSP/A. These included superficial biopsies, tangentially or obliquely sectioned material or any other technical reason that prevented an unequivocal diagnosis of SSP/L. Some cases with luminal dilatation and irregularity of architecture but not quite fulfilling the architectural features of SSP/A were considered suspicious for or possible SSP/A. These lesions were separated from diagnostic, unequivocal SSP/A or HP and were diagnosed very sparingly.
Reporting pathologists in the institution over the 4-year study period included several locum pathologists (some with an interest in gastrointestinal (GI) but not GI monospecialists) and pathologists who reported GI together with at least one other specialty but having a major interest in GI pathology. In 2012, three GI monospecialists were responsible for the reporting of GI cases, in addition to three others who were a combination of locums and non-GI monospecialists.
Results
These are illustrated and summarised in figures 1 and 2. The year-by-year analysis is as follows:

Right and left-sided sessile serrated polyps diagnosed initially and then confirmed after re-evaluation. Access the article online to view this figure in colour.

Right-sided serrated polyps initially diagnosed as hyperplastic polyps and then reclassified as sessile serrated polyps. Access the article online to view this figure in colour.
2009:
SSP/A: No cases were diagnosed as SSP/A.
Right-sided HP: A total of 66 HP occurring in 58 patients proximal to the splenic flexure were retrieved. Of these, 20 were reclassified as SSP/As (30%), including 3 with low-grade dysplasia. One right-sided HP was reclassified as a traditional serrated adenoma (TSA). The remaining 45 HPs remained as HP and no ‘possible’ SSPs/As were encountered.
2010:
SSP/A: A total of 46 polyps in 39 patients were diagnosed as such; 32 proximal to the splenic flexure and 14 left sided. Re-evaluation of the right-sided SSPs/As showed 100% agreement with the initial diagnosis and no cases were reclassified. Of the 14 left-sided cases diagnosed as SSPs/As, 8 were reclassified as HPs, 1 as a TSA and 1 as a mucosal prolapse-induced polyp. Four cases remained as bona fide left-sided SSPs/As.
Right-sided HP: Seventy patients with 91 HPs initially diagnosed were retrieved. Of these, 58 were reclassified as SSPs/As, including 1 case with low-grade dysplasia (64% reclassification rate as SSPs/As). An additional HP was reclassified as a TSA. The remaining 11 HPs remained as HPs. Again, no cases were interpreted as possible SSP/A.
2011:
SSP/A: One hundred and nine polyps from 80 patients were labelled as SSP/A, 87 from the right side and 22 from the left side. Of the 87 cases initially diagnosed as SSP/A, 83 were confirmed; of the 4 non-agreements, 2 were reclassified as HP, 1 as TSA and 1 as a conventional tubular adenoma. With regards to the 22 cases labelled as left-sided SSP/A, 13 were reclassified as HP, 3 as tubular adenomas and 1 as a TSA, leaving 5 polyps as SSP/A occurring in the left colon.
Right-sided HP: A total of 106 HPs occurring in 88 patients were re-evaluated. Forty-two cases were rediagnosed as SSPs/As, including 2 with low-grade dysplasia (40% reclassification as SSP/A). A further case was rediagnosed as a TSA, and in 23 cases, no evidence of a polyp was seen. The remaining 40 cases remained as HPs.
2012:
SSP/A: A total of 173 SSPs/As were diagnosed in 127 patients. Of these, 147 were located proximal to the splenic flexure, while 26 were deemed to be left sided. One hundred and thirty-four were agreed as SSPs/As. Thirteen right-sided polyps were reclassified from SSP/A to: three TSA, one Peutz-Jegher polyp, seven as possible or equivocal SSP/A and in two cases no obvious polyp was seen. Twenty-one of the 26 left-sided cases were reclassified as: 15 mucosal prolapse-induced polyps, 2 TSA, 3 conventional tubular adenomas and 1 possible or equivocal SSP/A. The remaining five left-sided lesions were regarded as true SSPs/As.
Right-sided HP: There were 206 HPs from 158 patients. Sixty-nine cases were reclassified as SSPs/As (reclassification 33%), including one case with low-grade dysplasia. A further 7 cases were thought to represent possible or equivocal SSPs/As, 1 was a tubulovillous adenoma, and in 25 cases, no evidence of a polyp was noted. The diagnosis of HP in the remaining 104 polyps remained as HP.
Discussion
Three distinct entities exist under the general rubric of ‘serrated polyps’: HP, SSP/A and TSA. The latter two types of polyp are considered as precursor lesions that follow the serrated pathway to colorectal cancer. Although somewhat contentious, it is even thought that the microvesicular variant of HP may be a precursor lesion to SSP/A. There is persuasive clinical evidence that the serrated pathway follows an accelerated course culminating in cancer.4 ,5 Thus, precursor lesions in this pathway are important and should be recognised, so that patients can be appropriately monitored and treated.
The diagnostic criteria for serrated polyps are well established and have been in use in routine diagnostic pathology for the last 7–8 years, especially in North America. The basis of this study was to explore the pathology reporting trends in the UK pathology department receiving a large number of GI biopsies.
The analysis of right-sided serrated polyps showed that over a 4-year period there is an obvious increase in awareness of the entity as evidenced by the exponential increase in its diagnosis. In 2009, no cases were diagnosed as SSP/A, while in 2012 a total of 173 cases were diagnosed. However, it is still quite clear that several SSPs/As in the right colon are still being labelled as HP, and there is a misdiagnosis of SSP/A in the left colon. Most of the SSPs/As in the right colon that are not diagnosed, or incorrectly labelled as HP, is due to lingering lack of awareness, suboptimal biopsy material, incorrect application of the diagnostic criteria and not adopting the minimum single crypt diagnostic criterion (as advocated by the American College of Gastroenterology). With regard to the left colon, the overdiagnosis of SSP/A is due to misinterpretation of HP with or without associated mucosal prolapse and other adenomas that may have a serrated appearance.
From this audit, it would appear that the concept and diagnosis of SSP/A have not occurred as readily as in North America. However, the entity was first described fairly recently, and of late there has been a plethora of papers in the UK/European literature highlighting diagnostic, molecular and therapeutic considerations.4–8 With this, increasing awareness and recognition of the entity are occurring along with its acceptance as a precursor lesion to cancer. Other important factors leading to the increase in diagnosis of SSP/A in Oxford were in-house clinico-pathological education sessions on SSP/A (with illustration of typical cases and discussion of diagnostic criteria) and the move to GI monospecialist reporting. Although interobserver comparison was not an objective of this study, analysis of the reporting trends showed remarkably good correlation between initial lesions diagnosed as SSP/A and subsequent re-evaluation, especially among GI monospecialist pathologists. Once the concept of SSP/A as a diagnostic entity was discussed among the pathologists (from 2010), the correct diagnosis was made on a consistent basis. This is reflected in zero cases being reclassified in 2010 (0%), four cases in 2011 (4.6%) and seven cases in 2012 (4.8%). This reclassification rate of under 5% is acceptable in standard routine pathology practice for any diagnostic entity.
The relatively high reclassification rates of right-sided HP to SSP/A over the 4-year period (30%, 64%, 40% and 33%, respectively) indicate that there is still a deficiency. Potential reasons include experience, expertise and awareness. Although the reclassification is high, the trend over the last 3 years shows a decrease and these figures have also to be interpreted in the face of increasing numbers of polyps being biopsied.
There is an overall increase in numbers of polyps of all types (including SSP/A) being sent for pathological evaluation over the 4 years of the survey. This is due to dedicated gastroenterologists with experience, expertise and an interest in polyps, and the implementation of a bowel cancer-screening programme in 2010 in Oxford.
There are several conclusions emanating from this audit. Awareness of SSP/A is increasing among pathologists in a large teaching hospital in the UK. Application of reproducible diagnostic criteria and awareness of histological mimics has resulted in the correct diagnosis of SSP/A being made increasingly over the 4-year study period. We suggest a diagnostic algorithm as a guideline when confronted by serrated polyps in the gastrointestinal tract (see figure 3).

{kind=link}
{kind=link}
{kind=link}
Suggested diagnostic algorithm for serrated lesions. Access the article online to view this figure in colour.
Reporting by GI specialist pathologists has also contributed to the increase in accuracy. This study also illustrates the impact of discussion and an education session among a team of pathologists. There was remarkable consistency and accuracy in the reporting of SSP/A. An increasing number of polyps including SSP/A are being sent to pathology for histological examination. From a practical point of view, we advocate the use of serial sections in poorly orientated biopsies in right-sided serrated polyps. Often times, the characteristic architectural features are revealed only in the deepest section. A useful aide memoire is as follows: if one encounters a right-sided serrated polyp, SSP/A should first be excluded and this may necessitate examining deeper sections. If one encounters a left-sided serrated polyp, the histological mimics (HP with or without mucosal prolapse and other types of adenomas, diverticular disease) should be considered first before labelling the lesion a SSP/A. SSPs/As do exist in the left colon but are distinctly less common compared to the right colon. If they do occur, then the right side should be checked for coexistent SSP/A. Similarly, HPs exist in the right colon, but every effort should be made to exclude a SSP/A first.
SSP/A is an important precursor lesion to colorectal cancer and their detection is an important aspect of early cancer prevention strategies. An increasing number of these lesions are being submitted for pathological examination and it is incumbent on pathologists to be aware of the lesion, its diagnostic criteria and how best to make the diagnosis, the differential diagnosis and the impact on patient management.
Take-home messages
-
Sessile serrated polyps (SSP) are being diagnosed more frequently.
-
Right-sided hyperplastic polyps should be carefully evaluated to exclude SSP.
-
Left-sided SSP are rare and other histological mimics must be excluded.
Footnotes
-
The necessary permission from the audit committee of Oxford University Hospitals was obtained to perform this audit.
-
Contributors All authors have contributed equally.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.