Article Text

Abstract
Aims To investigate whether drugs others than mycophenolic acid and ipilimumab might cause graft-versus-host-like apoptotic enteropathy, the clinicopathological findings in four patients were examined who had developed watery diarrhoea and apoptotic enteropathy (three cases from colon and one case from ileal pouch) after intake of antimetabolites (methotrexate and capecitabine) and/or tumour necrosis factor-α inhibitors (etanercept and infliximab).
Methods The clinical charts, endoscopy reports and intestinal biopsies from all endoscopies were reviewed for all patients. Biopsies were evaluated semiquantitatively for apoptosis of basal crypts, dilated damaged crypts, defined as cystically dilated crypts with flattened degenerated epithelium containing apoptotic debris and few neutrophils, and mucosal architecture. Further, the presence of intraepithelial lymphocytes, chronic inflammatory cells in the lamina propria and mucosal ulcerations was recorded and immunohistochemical analysis for human cytomegalovirus and herpes simplex virus was performed.
Results Endoscopic examination revealed normal mucosa in two patients, whereas the other two showed focal ulcerations. Histological changes included increased apoptosis of basal crypts, the presence of dilated damaged crypts and architecture distortion. In all cases, a temporal association between drug intake and/or dose increase, and onset of diarrhoea, was observed, and no convincing evidence of other potentially underlying causes of colitis/enteritis was found, including infections.
Conclusions Pathologists should be aware of the expanding spectrum of drugs that can cause apoptotic enteropathy, including antimetabolites and tumour necrosis factor-α inhibitors.
- Gastroenterology
- Apoptosis
- Diagnostics
Statistics from Altmetric.com
Introduction
Colitis may be caused by the adverse effects of many different types of drugs. Patterns of colitis associated with drug reactions include focal active colitis, diffuse active colitis, chronic active colitis, ischaemic colitis and microscopic colitis, among others. Mycophenolic acid (MPA) is an immunosuppressive drug that blocks de novo purine synthesis required for DNA synthesis and cell division.1 MPA-induced enteropathy (figure 1A) is characterised by an increased number of crypt cell apoptosis, reminiscent of colonic graft-versus-host disease (GVHD).2 ,3 To the best of our knowledge, the only drugs that have been associated with this pattern of colitis are MPA or the monoclonal anti-CTLA-4 antibody ipilimumab.4
{kind=link}
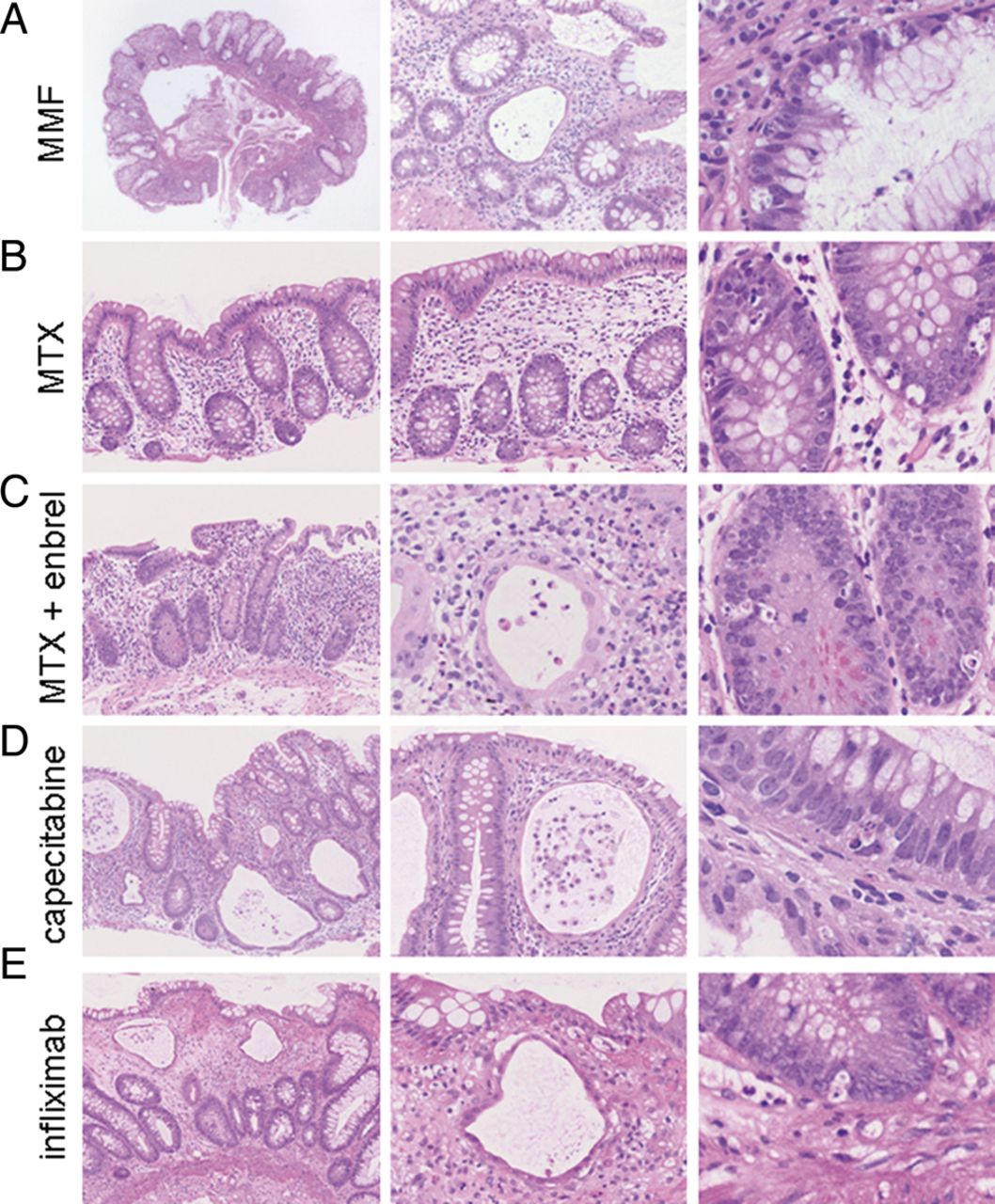
(A) Mycophenolic acid (MPA) enteropathy is characterised by architectural distortion, atrophic cystically dilated crypts and mitoses in the basal crypt epithelium. (B) Colon biopsy from a patient with methotrexate (MTX) therapy showing preserved architecture and numerous apoptosis in the basal crypt epithelium. (C) Pouch biopsy from a patient under combination therapy with MTX and etanercept revealing cystically dilated crypts with cellular debris, distorted architecture and numerous apoptotic cells in the basal crypts. (D) Colon biopsy from a patient with capecitabine chemotherapy showing significantly distorted architecture, an empty appearing lamina propria, numerous cystically dilated crypts with atrophic epithelial lining and cellular debris, and apoptosis of the basal crypt epithelium. (E) Colon biopsy from a patient with infliximab therapy revealing architectural distortion, empty appearing lamina propria, cystically dilated crypts with atrophic epithelial lining and scattered apoptosis of basal crypt epithelium.
In this report, we describe the clinical and pathological features of four adult patients, all of whom developed GVHD-like apoptotic enteropathy after the intake of drugs other than MPA or ipilimumab. These drugs include methotrexate (MTX) and capecitabine (Xeloda), both of which are antimetabolites, and the tumour necrosis factor-α (TNF-α) antagonists etanercept (Enbrel) and infliximab (Remicade). MTX functions by inhibiting folate-dependent enzymes, thus blocking the de novo purine synthesis,5 whereas capecitabine is a fluoropyrimidine carbamate, which works as a prodrug enzymatically converted to the pyrimidine analogue 5-fluorouracyl (5-FU) and irreversibly inhibits the enzyme thymidylate synthase, necessary for the synthesis of thymidine.6 Etanercept is a TNF-receptor fusion protein conjugated with the Fc region of human IgG,7 whereas infliximab is a chimeric anti-TNF-α monoclonal antibody.8
All four patients had a diarrheal illness that was temporally related to the patient’s drug intake and had no clinical, serological or pathological evidence of another potentially underlying cause of apoptotic enteropathy. To the best of our knowledge, this is the first report to observe an association between the abovementioned drugs and apoptotic enteropathy in humans.
Materials and methods
This study consisted of four adult patients who developed diarrhoea due to drug-induced apoptotic enteropathy in their colonic mucosal biopsies. These patients, and their colon biopsies, were retrieved from the clinical and surgical pathology files of the Institute for Surgical Pathology, University of Zurich, between July 2009 and March 2010. For all patients, the clinical charts, endoscopy reports and all colonic biopsies from all endoscopies were reviewed for a wide variety of clinical and pathological information. For all patients, a complete medical history was obtained with specific attention to the frequency, timing and dose of drug intake. All patients had follow-up clinical and pathological material available for analysis. This study was performed in accordance with the institutional ethic rules.
All biopsies were fixed in 10% buffered formalin and processed routinely. Three-micrometre-thick sections were cut and stained with H&E and Alcian blue/periodic acid-Schiff (AB-PAS) for histological evaluation. Each biopsy was evaluated semiquantitatively for apoptosis of basal crypts, dilated damaged crypts and mucosal architecture distortion. The following scoring system was used: none/minimal (−), rare/focal (+), numerous/strong (++). Dilated damaged crypts were defined as cystically dilated crypts with flattened degenerated epithelium containing apoptotic debris and few neutrophils.3 ,9 Also recorded was the presence of intraepithelial lymphocytes, chronic inflammatory cells in the lamina propria and mucosal ulcerations. In addition, immunohistochemistry for human cytomegalovirus (CMV) was performed in all cases and for herpes simplex virus (HSV) in three cases.
Results
Patient 1
The first patient, suffering from seropositive rheumatoid arthritis, chronic renal insufficiency, arterial hypertension, as well as struma nodosa treated with radioactive iodide, had received atenolol (150 mg/day), levothyroxine (0.1 mg/day), esomeprazole (40 mg/day), betahistine (16 mg/day) and prednisone (5 mg/day) for treatment of these diseases. Due to aggravating symptoms related to seropositive rheumatoid arthritis, additional therapy with MTX (20 mg/week subcutaneously) was started. After a few months, the patient developed watery diarrhoea, without mucus or blood. Fifteen months after beginning treatment with MTX, during which time the general health and weight were stable, the patient underwent a colonoscopy after bowel preparation with polyethylene glycol. This procedure revealed two small polypoid lesions, a few millimetres each in size, located in the transverse colon and rectum. No other abnormalities were noted. Histological examination of biopsies obtained from the colon and rectum, including the polypoid lesions, exhibited numerous apoptotic bodies (++) in the basal portions of the crypts. The crypt architecture was preserved, and no increased inflammation was detected in the lamina propria or epithelium (figure 1B). Immunohistochemical staining for CMV was negative.
At the time of colonoscopy, folic acid (5 mg, 3 times a week) was started, and the MTX dose was reduced, first to 15 mg/week, and later to 10 mg/week, since MTX was clinically suspected as the cause of the patient's diarrhoea. This led to complete normalisation of symptoms within a few weeks. A follow-up colonoscopy was not performed.
Patient 2
The second patient was taking prednisone (7.5 mg/day) for a 7-year history of a SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis). The patient had a past history of ulcerative colitis treated with proctocolectomy and ileo-anal pouch 13 years ago. Both MTX (12.5 mg/week) and folic acid (5 mg, twice/week) were used for treatment of the SAPHO syndrome. Due to worsening symptoms in the right foot, 2 months later, MTX was increased to 30 mg/week and etanercept (50 mg/week subcutaneously) was started. Four months later, the patient was admitted to our hospital with dehydration and acute renal insufficiency due to persistent watery diarrhoea. The patient had no clinical evidence of malabsorption. Patient's other medications also included bisoprolol (2.5 mg/day) and hydrochlorothiazide (6.25 mg/day) for arterial hypertension, both of these had been administered for more than 5 years, at constant dose.
During the stay in the hospital, endoscopy of the ileo-anal pouch was performed after bowel preparation with polyethylene glycol, which showed multiple ulcers. Biopsies of the ileo-anal pouch containing ileal and colonic type mucosa showed focal ulcerations. In addition, the non-ulcerated mucosa revealed distorted and cystically dilated crypts (+) with numerous apoptotic cells (++), mainly in the basal crypts, that contained necrotic cellular debris (figure 1C). Immunostains for CMV and HSV were negative.
Since it was noted that the episodes of diarrhoea were more frequent on the day following MTX injection, MTX was stopped, whereas etanercept was continued. Thereafter, the diarrhoea disappeared. Four months later, endoscopy was performed after bowel preparation with polyethylene glycol. This revealed small ulcerations. Biopsies of the pouch showed mild acute inflammation and only a slightly increased number of apoptosis in the basal crypts (+). CMV and HSV immunostains were negative.
Patient 3
The third patient was suffering from chronic renal insufficiency and arterial hypertension and was taking losartan (100 mg/day), hydrochlorothiazide (12.5 mg/day) and aspirin (100 mg/day) for the previous 5 years. The patient underwent a colon resection following a diagnosis of invasive adenocarcinoma of the sigmoid colon (pT3, G2). Adjuvant chemotherapy with capecitabine (750 mg/day) was started, which caused nausea and watery diarrhoea. Endoscopy was then performed after bowel preparation with polyethylene glycol. It revealed normal mucosa. Biopsies from the caecum and anastomosis were unremarkable except for the presence of scattered epithelial apoptosis in the crypt bases (+). Biopsies of the descending colon showed strong increased number of apoptosis (++) in the basal crypt epithelium, distorted crypt architecture (++), numerous cystically dilated crypts (++) with degenerated epithelium and containing cellular apoptotic debris and neutrophils, and a paucity of inflammatory cells in the lamina propria (figure 1D). Immunostains for CMV and HSV were negative.
Due to nausea and watery diarrhoea, capecitabine was discontinued after 11 days. This was followed by a rapid disappearance of gastrointestinal symptoms. For this reason, no further colonoscopy was performed.
Patient 4
The fourth patient had a clinical history of chronic renal insufficiency and relapsing polychondritis associated with systemic vasculitis and had been treated with prednisone (20–50 mg/day) for 3 years. Additional treatment with azathioprine (150 mg/day) and, subsequently, MTX (20 mg/day) provided no improvement. As a result, both medications were stopped, and then infliximab (400 mg every 4 weeks) was started. After 4–5 months, the patient developed watery diarrhoea. For the 2 years preceding the development of diarrhoea, the patient also received esomeprazole (40 mg/day) and lisinopril (10 mg/day). A colonoscopy was then performed after bowel preparation with polyethylene glycol. A small ulceration in the sigmoid colon was identified, but it was otherwise normal. Histological examination of biopsies from the sigmoid showed crypt architectural distortion (++), paucity of inflammatory cells in the lamina propria, cystically dilated crypts with degenerated epithelial lining (++) and cellular necrotic debris, as well as increased number of apoptosis in the basal crypts (+) (figure 1E). Immunostains for CMV and HSV were negative. Biopsies of the small bowel were not obtained.
After colonoscopy, infliximab was stopped and MMF (500 mg/day) was started. However, MMF was stopped after 2 weeks due to pancytopenia. A week after having stopped MMF (ie, 1 month following the last dose of infliximab), the patient reported great improvement in diarrhoea. A repeat endoscopy after bowel preparation with polyethylene glycol showed a few ulcers in the sigmoid colon. Biopsies from the sigmoid revealed regenerative changes, and those of the remaining colon revealed mild architectural distortion (+) and increased number of apoptotic cells in the crypt epithelium (+) (not shown). Biopsies obtained from the terminal ileum and duodenum were normal, and biopsies from the stomach showed a minimal increase in the number of apoptotic figures.
Discussion
In this study, we present four patients who developed watery diarrhoea and histological changes in their colon or ileal pouch biopsies reminiscent of apoptotic enteropathy after intake of antimetabolites (MTX and capecitabine) and/or TNF-α inhibitors (etanercept and infliximab). Endoscopic examination revealed normal mucosa for two patients, whereas the other two showed small ulcerations. In all cases, a temporal association between drug initiation and/or dose increase, and onset of diarrhoea, was observed, even though the time periods for the development of clinical symptoms ranged from few days to 5 months (clinical, endoscopic and histological findings are summarised in tables 1 and 2). In order to support a possible causal relationship of the association, the clinical history of the patients has to be considered in detail.
Summary of clinical findings
Summary of endoscopic and histological findings
Patient 3 developed symptoms few days after initiating capecitabine and discontinuation after 11 days was associated with rapid disappearance of the symptoms, which strongly suggests a causal relationship. Further, other features of chemotherapy-related damage, such as significant cytologic atypia, were not present. In addition, patient 3 was receiving aspirin. Aspirin intake was not temporally related to diarrhoea, and neither an increase in lamina propria eosinophils nor intraepithelial lymphocytes were found. Moreover, aspirin dosage was low, and no effects attributable to aspirin were observed in the upper gastrointestinal tract. Finally, patient 3 was treated with losartan, an angiotensin II antagonist. Interestingly, olmesartan, another antihypertensive drug of the same family, was previously shown to cause diarrhoea. However, olmesartan-related histological changes are characterised by sprue-like villous atrophy in the small intestine and lymphocytic and collagenous colitis in the colon,10 ,11 which differ from those observed in the patient described here. Moreover, losartan intake in this case was not temporally related to the patient's gastrointestinal symptoms.
The remaining patients developed the described symptoms with a delay of up to 4–5 months; nevertheless, both the rapid disappearance of symptoms after drug removal/dosis reduction and the clinical history suggest a causal relationship. In particular, patient 1 developed watery diarrhoea few months after starting MTX, but a close temporal association between withdrawal of MTX and cessation of complaints was observed. This fact, together with lack of any other potential clinical explanation, strongly suggested that MTX was the cause of the diarrhoea in this patient.
Patient 2 was hospitalised due to persistent watery diarrhoea 4 months after MTX dosis increase and starting etanercept; however, once MTX was stopped, the diarrhoea disappeared. Since patient 2 had a history of ulcerative colitis, the differential diagnosis included drug-induced changes and IBD. However, except for mild (nonspecific) pouchitis, the histological findings were most compatible with drug-induced apoptotic enteropathy. Neither marked crypt architectural disarray nor increased lymphoplasmacellular infiltrates of the lamina propria were present.
Patient 4 also showed a delay of 4–5 months in the development of the diarrhoea after starting infliximab. The clinical history of this patient was complicated by the fact that MMF was administered for 2 weeks shortly after stopping infliximab. However, a rapid improvement in diarrhoea was reported a week after having stopped MMF. Regarding the administration of MMF, histological features compatible with MPA-induced changes had been observed prior its administration when the patient was only taking infliximab. The reasons for the delay between drug initiation and onset of symptoms are not clear and are a matter of speculation. In case of MTX, the delay might represent the time needed by MTX to deplete the folate storage.
MTX is indicated for the treatment of neoplastic and autoimmune diseases, such as rheumatoid arthritis, whereas capecitabine is approved for the treatment of carcinomas of the gastrointestinal tract and breast. For both, diarrhoea, nausea and vomiting are frequent adverse effects and represent the most prominent dose-limiting toxicities.12 A direct cytotoxic effect via impairment of enterocyte proliferation has been proposed for MPA.13 ,14 Since MTX and capecitabine also are antimetabolites, it is conceivable that both share this mode of toxicity with MPA. Alternatively, they could modulate the immune system, which may result in a reaction against enterocytes, as in patients with immunodeficiency or immune disregulation.15 ,16
The TNF-α inhibitors, infliximab and etanercept, are indicated for treatment of autoimmune diseases, such as rheumatoid arthritis, psoriasis and inflammatory bowel diseases. Gastrointestinal side effects of TNF-α inhibitors are rare.17 Recently, diarrhoea and anorexia, anal abscesses and oral ulcers, together with inflammatory bowel disease, have been reported in some patients treated with etanercept for juvenile idiopathic arthritis.18 Increased apoptosis was not described in these patients. Six patients achieved complete remission of gastrointestinal symptoms after switching treatment from etanercept to infliximab. This difference may be due to the fact that etanercept binds not only to TNF-α, but also to lymphotoxin-α.18 Histological changes in the gastrointestinal tract after treatment with TNF-α inhibitors were found to be related to modulation of the immune system and impaired clearance of bacteria.19
Apoptotic cells are rarely found in normal intestinal mucosa. When present, they are usually confined to the surface epithelium due to normal cell turnover. In contrast, apoptosis in the deep portions of the crypts is considered abnormal.2 Increased crypt apoptosis (ie, one apoptotic body/biopsy20 or more than five apoptotic bodies/100 crypts21) should alert pathologists to seek for additional histological changes, such as acute or chronic inflammation, mucin depletion, crypt loss, cryptitis and Paneth cell metaplasia, which can help in attributing the findings to a particular aetiology.22
Clinical history is crucial for the identification of the cause for an increase in apoptosis in the colon, with particular regard to drug intake.3 Non-steroidal anti-inflammatory drugs (NSAIDs) can induce apoptosis by both COX-2-dependent and COX-2-independent mechanisms.23 NSAID injury in the colon is usually present only with high dosage and changes, which are more prominent in the upper gastrointestinal tract,24 ,25 are accompanied by an increase of lymphocytes and eosinophils in the lamina propria, and increased intraepithelial lymphocytes.21 Sodium phosphate-containing bowel preparation formula for colonoscopy can also induce apoptosis of the intestinal mucosa. However, bowel preparation in our patients was performed with polyethylene glycol, which is not known to cause pathological changes in the bowel.26 Thus, it is very unlikely that bowel preparation-related changes accounted for the histological changes found in the four cases presented in this study. Other potential causes for increased apoptosis in the colon include chronic variable immunodeficiency, autoimmune enterocolitis and GVHD following bone marrow or, more rarely, solid organ transplantation. Furthermore, viral infectious diseases can also cause increased apoptosis, but none of our cases was CMV or HSV positive by immunostain.
In summary, we describe four patients who developed diarrhoea temporally related to, and presumably caused by, intake of antimetabolites and/or TNF-α inhibitors, all of whom developed histological changes in the colon reminiscent of apoptotic enteropathy.
Take home messages
-
We have observed histological changes reminiscent of intestinal graft-versus-host disease (GvHD)-induced and mycophenolate-induced colopathy in four patients presenting with diarrhoea and mostly unremarkable endoscopic findings after treatment with antimetabolites (methotrexate, capecitabine) and/or tumour necrosis factor-α (TNF-α) inhibitors (etanercept, infliximab).
-
The close temporal association between drug intake and diarrhoea suggests that clinical symptoms and histological changes were treatment related and indicate that TNF-α inhibitors and antimetabolites other than mycophenolate can cause GvHD-like and mycophenolate-like histological changes.
-
Pathologists should be aware of the expanding spectrum of drugs causing GvHD-like and mycophenolate-like histological changes in intestinal biopsies, which might be confined to aberrant (basal) crypt apoptosis, and comment these findings in their reports in order to allow an adequate treatment approach.
Acknowledgments
We thank our clinical colleagues for providing information on patients.
References
Supplementary materials
Abstract in German
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in German - Online German-Abstract
Footnotes
-
Contributors DS analysed the data of the study, drafted the manuscript and performed the tables. AG, MM and TR made initial pathological diagnosis and acquired clinical data. GR helped acquire the clinical data. RO reviewed the cases and revised the manuscript critically. AW conceived and designed the study, reviewed the cases, revised the manuscript and assembled the figure. All authors read and approved the final manuscript.
-
Funding This work was supported by a grant from the Swiss National Research Foundation (SNF; project 310030_146940/1) to AW.
-
Competing interests None.
-
Ethics approval This study was performed in accordance with the ethic rules of the University Hospital and University of Zurich.
-
Provenance and peer review Not commissioned; externally peer reviewed.