Article Text

Abstract
Background: Activating epidermal growth factor receptor (EGFR) mutations have been implicated in non-small cell lung cancer (NSCLC), and have also been clinically correlated with patient sensitivity to targeted EGFR inhibitors.
Aim: To describe a technique for determining EGFR mutation status on archival fine needle aspirate (FNA) specimens from advanced NSCLC patients.
Methods: Eleven archival FNA slides from patients with advanced NSCLC were examined for diagnostic material to identify tumour cell-enriched regions. EGFR mutation status was determined using a slide-scrape DNA extraction protocol of selected tumour cell regions on the smear slides, followed by real time PCR and high resolution melt analysis (HRMAA) of EGFR exons 18, 19, 20, and 21, followed by sequence analysis.
Results: All DNA samples were successfully amplified by PCR. Three adenocarcinoma patient samples contained EGFR mutations in exon 19 (L747-P753insS). One of the three had an additional exon 19 mutation (A755D).
Conclusions: Archival cytology slides from patients with NSCLC can be used to determine EGFR mutation status by PCR, HRMAA, and sequencing. The ability to use archival cytology slides greatly increases the potential material available for molecular analysis in diagnosis and selection of patients for targeted therapeutic agents.
Statistics from Altmetric.com
Mutations in the epidermal growth factor receptor (EGFR) gene (7p12.3-p12.1) in non-small cell lung carcinoma (NSCLC) have been investigated because of a reported correlation between mutations and tumour response to treatment with targeted tyrosine kinase inhibitors (TKI), particularly gefitinib (Iressa, AstraZeneca Pharmaceuticals LP, Wilmington, DE, USA) and erlotinib (Tarceva, OSI Pharmaceuticals Inc., Melville, New York, USA).1–4 These drugs are orally active small molecule quinazolinamine derivatives that bind and block the active site of the epidermal growth factor receptor. Drug response has been shown to depend in part on increased sensitivity to TKI conferred by EGFR mutations at the ATP binding site.5 6 These mutations have shown some correlation with demographic and histopathologic categories, being often identified in tumours with bronchioloaveolar histology, and in patients who are female, non-smokers, and of Asian descent. EGFR mutations are found in approximately 10% of cases of NSCLC in North America and 30–50% of NSCLC patients of East Asian descent.7 8
Clinical studies as well as functional studies performed with tissue culture cells and mouse models provide supporting evidence that certain EGFR mutations in the ATP binding domain of the EGFR protein confer greater sensitivity to TKI.9–14 However, EGFR gene mutations may not be the sole determinants of tumour response, and other factors, such as EGFR gene copy number, may be implicated.15 16 Further clinical studies will be necessary to confirm that patients with activating mutations in EGFR are more responsive to TKI therapy.
The detection of EGFR mutations in NSCLC patients is considered valuable both for guidance in therapy and for clinical investigations. However, in advanced stage lung carcinoma in particular, pathological diagnosis may be made by small biopsy or cytology alone because surgery does not usually play a role in treatment. In these cases, adequate tissue samples may not be available for analysis by immunohistochemistry, fluorescence in situ hybridisation or other ancillary studies requiring formalin-fixed, paraffin embedded (FFPE) tissue.
In this report, we screened for EGFR mutations in 11 patients for whom the only diagnostic material consisted of air-dried, Romanowsky-stained slides made from fine needle aspiration biopsy (FNA) specimens. DNA was extracted from selected tumour cell-enriched regions by a slide-scrape lysate procedure, followed by real-time PCR amplification of exons 18, 19, 20, and 21, where EGFR activating mutations reside. Mutations were detected by high resolution melting amplicon analysis (HRMAA), a rapid screening method previously reported to detect EGFR mutations in FFPE tissue,17 and in a recent report, archival Papanicolaou-stained cytology slides.18 The goals of our study were: (1) to establish a method of scraping selective tumour cell fields from archival Romanowsky-stained FNA slides for DNA extraction; and (2) to determine if DNA extracted from the FNA smears could be used to ascertain the EGFR mutation status of NSCLC patients using PCR and HRMAA.
PATIENTS AND METHODS
Case selection
The cases chosen for this retrospective study were diagnosed with NSCLC during the period March 2003 to 15 July 2005, and are part of an ongoing clinical trial begun at the Huntsman Cancer Institute (Salt Lake City, Utah, USA) in which 40 patients with advanced NSCLC were selected to receive TKI therapy. EGFR mutation status information was not known at the time of treatment. The 11 cases selected for this study had been diagnosed solely on the basis of FNA cytology specimens as opposed to surgical pathology specimens; a 12th FNA case was excluded because of scant cellularity. Patients ranged in age from 49–86 years at the time of diagnosis.
Slide selection
Slides were carefully screened by two pathologists to ensure that adequate diagnostic material would remain for archival purposes after tumour cells were removed for the assay, and to confirm the diagnosis of non-small cell lung carcinoma. The use of human tissue for this study was approved by the Institutional Review Board at the University of Utah (IRB #17373).
Deoxyribonucleic acid isolation by slide-scrape lysate
We have previously described similar procedures.19 20 After Romanowsky-stained slides were screened by two pathologists, areas containing the highest tumour content were indicated with a diamond-tipped pencil and coverslips were removed by soaking the slides in xylene. One slide per case was used for the extraction procedure; to confirm results for three cases, an additional slide was used to carry out repeat extractions and PCR amplifications.
Slides were rehydrated through a series of ethanol washes and distilled water, then destained in 1% hydrochloric acid in 70% ethanol, then washed sequentially in running and Scott’s tap water. A buffer solution (1% Tween 20 in 50 mM Tris, 1 mM EDTA, pH 8.0) was pipetted onto regions marked with a diamond pencil, and these areas were carefully scraped with a sterile scalpel blade to dislodge cells from the slide surface. Scraped material and buffer were then pipetted into a microcentrifuge tube and incubated with proteinase K for 12–16 h at 56°C. Samples were subsequently centrifuged at 12 000 rpm for 5 min and the supernatant was transferred to a clean microcentrifuge tube, followed by a 10 min incubation at 95°C to inactivate proteinase K. Sample DNA was estimated by measuring absorbance using a NanoDrop ND-1000 instrument (NanoDrop Technologies, Wilmington, Delaware, USA). DNA extracts were then directly used for PCR using exon-specific primers and were evaluated by HRMAA. Samples with melt profiles that deviated from wild type were sequenced to determine if mutations were present.
Reagents and primer design
Reagents and primer design have been described previously.17 20–22 Primer sequences and expected amplicon sizes are shown in table 1.
PCR and high resolution melting curve analysis
These procedures have been described previously.17 Briefly, PCR was performed in a capillary cuvette (total volume 20 μl) on a Light Cycler (Roche Diagnostics, Indianapolis, Indiana, USA), with reactions using dUTP instead of dTTP. Prior to PCR the samples were incubated with 1 unit of uracil N-glycosylase (Amperase, Applied Biosystems, Foster City, California, USA) to prevent “carry-over” contamination. All samples contained the double stranded DNA binding dye, LCGreen I (Idaho Technology, Salt Lake City, Utah, USA). After an initial pre-incubation step at 95°C (to denature the uracil glycosylase and activate the FastStart Taq DNA polymerase), PCR was carried out for 45 cycles. Each cycle included denaturation at 95°C for 10 s, followed by annealing at 60°C for 10 s, and finally extension at 74°C for 0 s. Transition rates were 20°C/s from denaturation to annealing, 1°C/s from annealing to extension, and 20°C/s from extension to denaturation. After PCR, the samples were momentarily heated to 95°C and then cooled to 40°C. Sample cuvettes were then transferred individually to the HR-1, a high resolution DNA melting analysis instrument (Idaho Technology, Salt Lake City, Utah, USA) and melting analysis was performed as described.17 Because melt profile may vary depending on DNA concentration, serial dilutions of genomic DNA were used as control standards. All patient samples were run in triplicate.
DNA sequence analysis
Bidirectional DNA sequencing was performed at the core facility of the University of Utah on all samples with abnormal melt profiles. Sequence analysis was performed with DNA Sequencher 4.1.4 software from Gene Codes Corporation (Ann Arbor, Michigan, USA).
RESULTS
Patient characteristics
Eleven patients with a diagnosis of advanced stage non-small cell carcinoma of the lung were assessed; four females and seven males, with ages ranging from 49–86 years (table 2). Five cases were metastatic NSCLC with diagnosis based on cytomorphology of FNA smears from the liver, rib mass, or adrenal mass; the other six samples were from lung. Cases included seven adenocarcinomas, three squamous cell carcinomas, and one poorly differentiated carcinoma.
Cell distribution on cytology slides
All specimens tested consisted of archival FNA smears with varying cellularity as well as distribution and number of normal, inflammatory, and carcinoma cells. The approach to scraping and removal of the cells was adjusted accordingly, and the volume of buffer spread over the region varied depending on the size of the tumour cell containing area. Table 3 summarises the variation in tumour cell content and resulting areas scraped for DNA extraction for the 11 NSCLC cases. The areas scraped ranged from 6.9–299 mm2, with the percentage of tumour cell DNA in those slide regions estimated to range from 80 to >90%. In all cases, sufficient DNA was obtained by extraction of the selected tumour cell-enriched regions from a single slide. However, in three cases (cases 1, 6, and 7) repeat scrape extractions of an additional slide for each case were carried out to confirm PCR and HRMAA results.
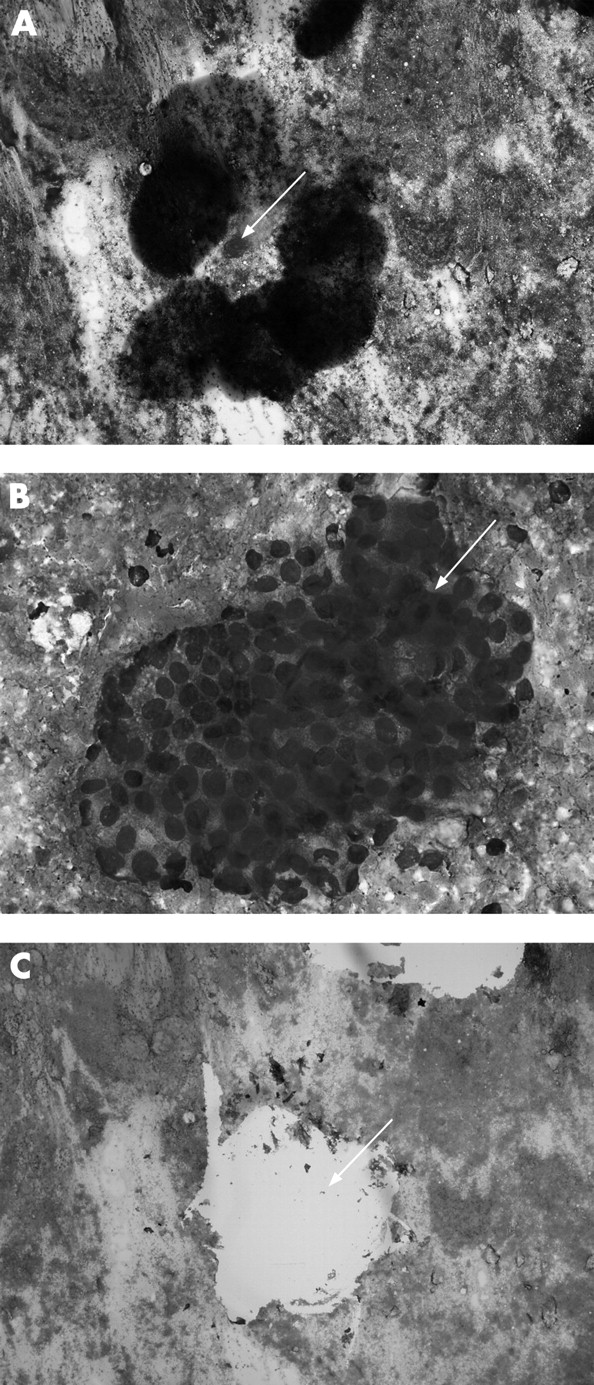
Figure 1 shows the distribution of tumour cells (circled) from one NSCLC case (fig 1A, arrow). An enlarged image of this group of tumour cells is shown in fig 1B (arrow). In most cases, clumps of tumour cells made up a high percentage of sampled material, and the primary contaminants consisted of red blood cells or necrotic material in the background of the smear. After marking the area with a diamond pencil, coverslip removal and destaining, the area containing the tumour cells was scraped from the slide into extraction buffer. The cell-free area of the slide (fig 1C, arrow) indicates that the cells had been successfully removed. Although tumour cells from multiple areas of the slide were removed, it was possible to preserve other diagnostic tumour cell groups on the slide for archival purposes. Identification and scraping of selected regions of tumour cells effectively minimised contamination by inflammatory cells in HRMAA analysis. Even slides that appeared to have very scant cellularity showed evidence of amplification. All 11 extracted samples contained adequate DNA for PCR amplification, ranging from 79 to 233 ng/μl, with total yields estimated at 7.9 μg to 20.8 μg.
HRMAA for EGFR exons 18, 19, 20, 21
All cases of NSCLC were screened by HRMAA to detect EGFR activating mutations. A total of 44 exons were screened in this study (4 EGFR exons per case). Mutations have been reported in each of these four exons, which together encode the cytoplasmic ATP binding pocket of the receptor. To confirm the accuracy of HRMAA in the detection of EGFR mutations, all abnormal melting curves for specific exons were followed up by direct DNA sequencing of PCR products.
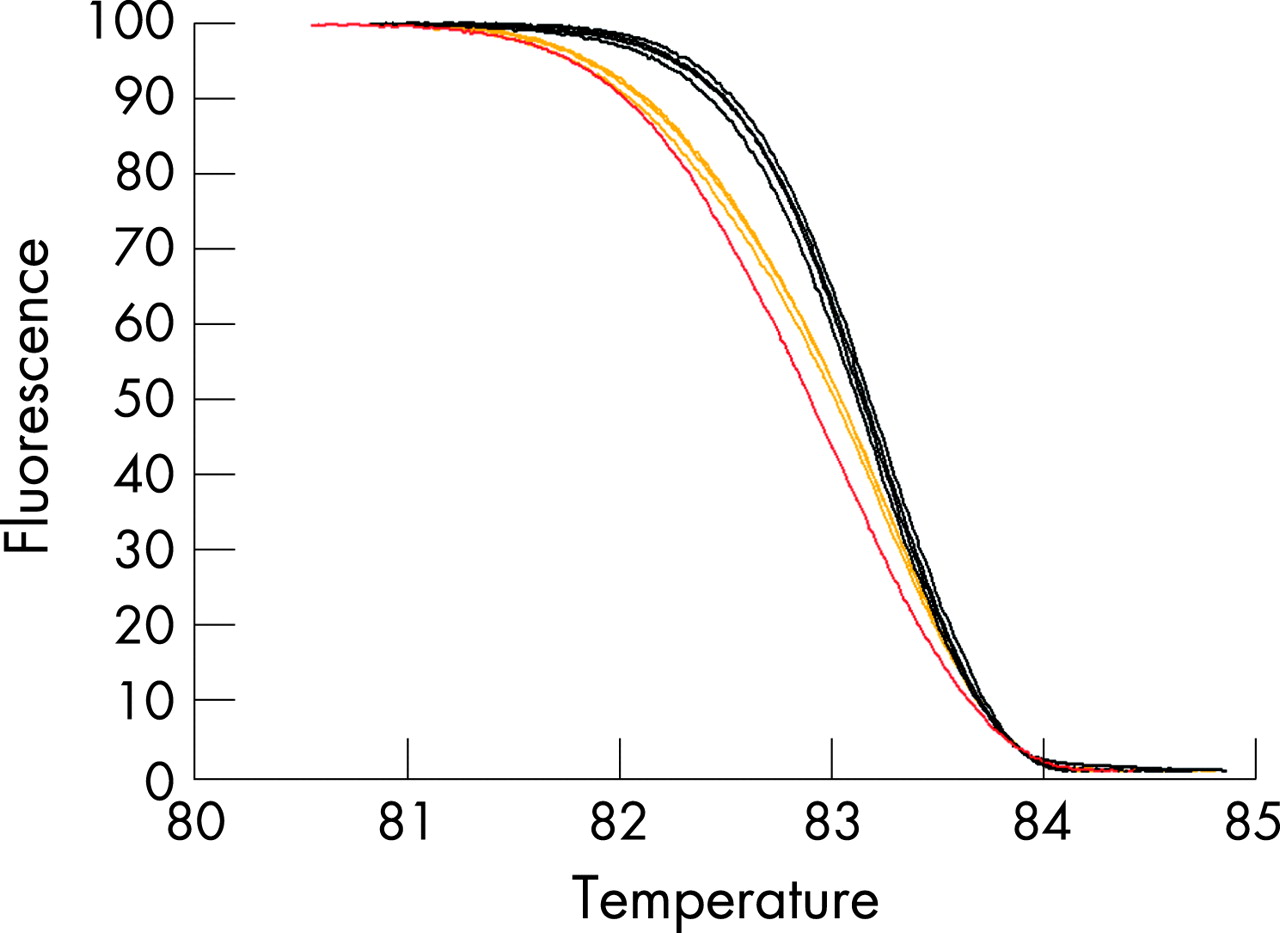
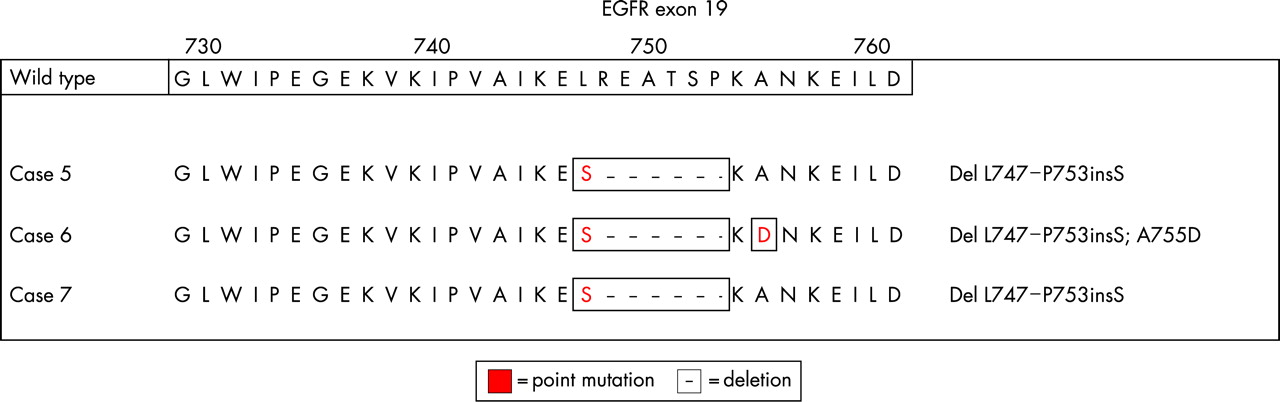
Table 4 summarises the sequencing results from cases in which abnormal melts were observed for EGFR exons. Of the 11 cases screened, 3 (cases 5, 6 and 7) contained the in-frame deletion mutation/insertion in exon 19 that has been previously described to be an activating EGFR mutation.8 An example of the HRMAA curve obtained from a case containing an EGFR exon 19 mutation (L747-P753insS) is shown in fig 2, with the replicated patient DNA displaying melt profiles resembling that of the mutant control sample. The L747-P753insS mutation in exon 19 would result in the deletion of the amino acids LREATSP with the insertion of S in all three of these cases, as shown in fig 3.


{kind=link}
{kind=link}
{kind=link}
One of the three cases with the exon 19 deletion/insertion mutation (case 6) contained a second point mutation in exon 19 (A755D) that is not listed in the Welcome Trust Sanger Institute or City of Hope databases, nor is it reported in the National Center for Biotechnology Information (NCBI) single nucleotide polymorphism (SNP) database. A sequencing electropherogram showing the area of the deletion for this case is shown as supplementary material. Efforts to extract DNA from normal cells to determine if this represents a somatic mutation rather than a germ-line mutation have given insufficient DNA for PCR amplification.
All three cases in which the exon 19 mutation was found were from patients with adenocarcinoma, two of which were poorly differentiated. Two of the three cases were diagnosed from liver FNAs. Ages of the three patients ranged from 53–77 years, and two of the three were women.
In addition to the in-frame deletion and mis-sense mutations in exon 19, we identified a common silent mutation located in EGFR exon 20 at nucleotide position 2361 (G to A) in 9 of 11 cases, with 5 cases that were heterozygous, and 4 cases that were homozygous for the polymorphism. We also detected in one case (case 8) an additional polymorphic silent mutation in exon 21 (R836R, CGC → CGT).
DISCUSSION
Currently, EGFR mutation status testing in NSCLC patients typically relies on the use of FFPE specimens. However, in our experience, roughly one-third of NSCLC primary diagnoses are made on cytology specimens, and no additional biopsy materials are available for molecular studies. To augment the specimen types available for EGFR mutation and other molecular analysis, we investigated the possibility of using archived Romanowsky-stained FNA smears for DNA extraction and EGFR mutation scanning.
EGFR mutations are generally identified by sequence analysis of PCR-amplified exons in which the activating mutations are frequently found. However, sequencing all four of the pertinent EGFR exons that potentially harbour mutations is time-consuming, costly, and requires expertise in interpretation that is not readily available in all clinical settings. In addition, some studies suggest that sequencing may be less sensitive than other mutation screening assays.23 Unlike DNA sequencing, HRMAA can be accomplished in as little as 15 min after PCR of the appropriate exon, and is a more sensitive screening technique for identifying EGFR mutations. As previously reported, this method is unlikely to give false negatives if the sample consists of at least 50% tumour content.20 24 In the present study all abnormal melting curves obtained by HRMAA also contained an abnormal DNA sequence, either a mutation or a polymorphism.
Of the 11 NSCLC cases examined, 3 harboured an in-frame deletion/insertion in exon 19 (L747-P753insS). This mutation and closely related variants are the most prevalent of the activating mutations reported in the literature, representing 45% of those described.8 The size of the deletion varies from 9–24 base pairs, and is always in-frame. The mutation typically causes minimally the deletion of leu-arg-glu-ala (one negatively charged, one positively charged and two non-polar amino acids), which alters the binding constant for ATP in the kinase domain.
Take-home messages
This proof-of-concept study was undertaken to determine if archival fine needle aspiration (FNA) slides could be used to determine epidermal growth factor receptor (EGFR) mutation status using samples from patients that had been cytologically diagnosed with advanced non-small cell lung carcinoma (NSCLC), and treated with the tyrosine kinase inhibitor Tarceva without knowledge of mutation status.
We confirm archival FNA samples can be used to determine EGFR mutation status using PCR and high-resolution melt analysis.
Regions of tumour cells can be selectively scraped from the smears to reduce normal cell contamination during DNA extraction and PCR.
Three patients were found to have the in-frame deletion in exon 19 (L747-P753insS) that is one of two commonly found mutations among TKI-responding adenocarcinoma patients.
One of the three patients had an additional mutation in exon 19 (A755D), which would result in a non-conservative amino acid substitution of alanine for aspartic acid, which could theoretically alter enzyme activity.
One of the three patients with the in-frame exon 19 deletion carried an additional, previously undescribed mutation. This mutation, A755D, would cause the non-polar amino acid alanine to be substituted by the negatively charged amino acid aspartic acid, a change that might impact the three-dimensional structure of the ATP binding pocket. To our knowledge, this mutation has not been previously described, although Cortes-Funes et al25 have described a mis-sense mutation K754R occurring in a patient with the in-frame deletion delL747-P753insS. The K754R mutation would represent a more conservative change, resulting in the substitution of one positively charged amino acid, lysine, for another positively charged amino acid, arginine. The functional significance of these mis-sense mutations to the EGFR protein is unknown.
As has been reported previously, a common silent mutation is located in EGFR exon 20 at nucleotide position 2361 (G to A). This results in a codon change from CAG to CAA but it does not change the glutamine located at amino acid residue position 787. The high prevalence of this silent mutation complicates HRMAA for EGFR exon 20. In our study we identified this common polymorphism in nine of 11 cases, and although they produced abnormal melting curves, they were negative for activating mutations in exon 20. We additionally identified in one case a polymorphic silent mutation in exon 21 (R836R, CGC → CGT).
The presence of these polymorphisms coding for silent mutations can lead to unnecessary sequencing of amplicons in the absence of other mutations. Although the major activating EGFR mutations are primarily in exons 19 and 21, with the in-frame deletion in exon 19 and L858R accounting for ∼90% of reported mutations, additional mutations do occur in exons 18 and 20 that account for >8% of mutants.8 In addition to activating mutations, there are reports of resistance mutations in exons 18, 19 and 20 appearing in patients treated with TKIs.26–29 To adequately monitor patients it may be important for clinical assays to scan all four EGFR exons. Further investigation in this area is warranted to avoid sequencing false positive tests resulting from the presence of polymorphisms.
As our study was nearing completion, a separate study reported using HRMAA and cytology slides to determine EGFR status in NSCLC patients.18 Our study differs from that of Nomoto et al in several significant ways. Whereas our study used tumour-enriched areas of Romanowsky-stained slides from FNA samples only, the Nomoto study used Papanicolaou-stained slides from some FNA but primarily exfoliative samples, which might be expected to have a higher population of contaminating normal cells. For most of the patient samples, the Nomoto investigation used entire slides for extraction. Our study scanned for EGFR mutations in exons 18, 19, 20 and 21, and used direct sequencing of PCR products to confirm mutations, whereas the Nomoto inquiry focused only on exons 19 and 21, and used sequencing results from FFPE samples of a prior study to infer the presence of specific mutations in the study patients rather than direct sequencing of PCR products.18 Nomoto suggested that of 29 patients, the exon 19 in-frame deletion was present in 8 patients (27.6%) and the exon 21 L858R mutation was detected in 6 patients (20.7%) for a total of 48.3%. Our study detected the exon 19 deletion mutation in 3 of 11 patients (27%). The frequency of the activating mutations is higher in Asian populations.4 The two studies demonstrate that EGFR mutation status can be determined using DNA extracted from cytology slides and PCR followed by HRMAA.
In our study we have shown that PCR amplification and HRMAA can be used to identify mutations in EGFR exons 18, 19, 20, and 21 using archival FNA Romanowsky-stained slides. For this type of analysis to be successful, our research suggests that it is very important that slides be fully destained before DNA extraction is carried out, as residual stain in the extract appears to interfere with PCR amplification and melt analysis. Although the Nomoto study did not discuss stain interference with PCR amplification, our prior experience and that of others30 suggests that it is also important to fully destain archival Papanicolaou-stained slides to avoid PCR difficulties. The two studies together suggest that slides prepared with either Romanowsky or Papanicolaou stains can be used for PCR and HRMAA mutation evaluation.
Because tumour cell genotype may differ from that of non-tumour cells, assay sensitivity depends on the ratio of tumour cells to normal cells in the sample. We have demonstrated that it is possible to extract DNA from tumour-cell-enriched regions of a slide, thus increasing the possibility of obtaining results that reflect the EGFR mutation status of tumour cells, rather than contaminating normal cells. With FNA sampling it is often the case that only one slide will contain tumour cells; with selective slide scraping of tumour groups from the slide, tumour-cell containing regions on the same slide can still be preserved for archival purposes. The availability of cytology specimens for EGFR mutation screening has important clinical relevance for the identification of patients that may be responsive to TKI inhibitors, but also has broader implications for the potential expanded use of cytology slides from different body sites for molecular studies and in clinical diagnosis and treatment strategies.
Consistent with previous reports showing that activating EGFR mutations occur more commonly in adenocarcinomas,31 in our study all three cases that were positive for an exon 19 deletion mutation were diagnosed as adenocarcinomas. Treatment options for NSCLC patients may vary depending on whether a patient is diagnosed as having adenocarcinoma, squamous cell carcinoma, or another type of NSCLC; patients with adenocarcinoma are more likely to respond positively to TKI.
The presence of EGFR activating mutations in NSCLC has been correlated with tumour response to targeted TKI chemotherapy.1–3 8 Studies with transfected cultured cells and mouse models provide strong support for the role of these deletions in altering EGFR activity, and increasing the sensitivity of EGFR to TKI.9–14 Currently, there is some controversy regarding the best predictor of response and overall survival to the EGFR inhibitors, with some studies suggesting that the response of NSCLC to EGFR inhibitors may be more closely related to other factors such as gene copy number or EGFR overexpression.15 16 One difficulty with resolving the issue is that EGFR mutations, amplifications, and overexpression frequently co-occur.8 Additional clinical trials are needed to better elucidate these relationships.
Because therapy with EGFR inhibitors in the treatment of NSCLC may require EGFR mutation analysis, and because tissue samples for this purpose often consist of scant material or FNA smears, we investigated and confirmed the potential of providing this information rapidly and efficiently with a slide-scrape DNA extraction procedure to enrich for tumour cells, followed by exon-specific real time PCR and HRMAA. These findings may help to expand the pool of patients eligible for future prospective clinical trials to fully investigate the relationship between the presence of activating EGFR mutation and response to TKI. In addition, larger retrospective reviews may be possible, using cases where only archival cytology material is available and molecular studies were not previously considered feasible.
Acknowledgments
The authors would like to thank Dr Joe Holden for reviewing the manuscript, and Leslie Rowe for sharing protocols and demonstrating the slide-scrape extraction procedure for cytology specimens.
REFERENCES
Supplementary materials
web only figure 61/4/487
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: This work was supported in part by the Associated Regional and University Pathologists (ARUP) Institute for Clinical and Experimental Pathology.