Article Text

Abstract
The detection and correction of vitamin B12 (B12) deficiency prevents megaloblastic anaemia and potentially irreversible neuropathy and neuropsychiatric changes. B12 status is commonly estimated using the abundance of the vitamin in serum, with ∼148 pmol/L (200 ng/L) typically set as the threshold for diagnosing deficiency. Serum B12 assays measure the sum of haptocorrin-bound and transcobalamin-bound (known as holotranscobalamin) B12. It is only holotranscobalamin that is taken up by cells to meet metabolic demand. Although receiver operator characteristic curves show holotranscobalamin measurement to be a moderately more reliable marker of B12 status than serum B12, both assays have an indeterminate range. Biochemical evidence of metabolic abnormalities consistent with B12 insufficiency is frequently detected despite an apparently sufficient abundance of the vitamin. Laboratory B12 status markers that reflect cellular utilisation rather than abundance are available. Two forms of B12 act as coenzymes for two different reactions. Methionine synthase requires methylcobalamin for the remethylation of methionine from homocysteine. A homocysteine concentration >20 µmol/L may suggest B12 deficiency in folate-replete patients. In the second B12-dependent reaction, methylmalonyl-CoA mutase uses adenosylcobalamin to convert methylmalonyl-CoA to succinyl-CoA. In B12 deficiency excess methylmalonyl-CoA is hydrolysed to methylmalonic acid. A serum concentration >280 nmol/L may suggest suboptimal status in young patients with normal renal function. No single laboratory marker is suitable for the assessment of B12 status in all patients. Sequential assay selection algorithms or the combination of multiple markers into a single diagnostic indicator are both approaches that can be used to mitigate inherent limitations of each marker when used independently.
- COBALAMIN
- LABORATORY TESTS
- B12
- DIAGNOSIS
Statistics from Altmetric.com
Introduction
The clinical utility of approaches taken by laboratories for the assessment vitamin B12 (B12) status are generally poorly understood by service providers and by their users alike. Consequently, opportunities to diagnose B12 deficiency are often not realised. This best practice review highlights the inherent advantages and limitations of diagnostic markers of B12 status and makes recommendations for the application of laboratory assays when used independently and in combination.
Background
B12 is essential for the transformation of methyltetrahydrofolate to tetrahydrofolate for DNA synthesis and for fatty acid metabolism. The timely detection and correction of B12 deficiency prevents megaloblastic anaemia and potentially irreversible neuropathy and neuropsychiatric changes.1 ,2 Crucially, patients who have developed peripheral neuropathy or subacute combined degeneration of the cord may have no discernable haematological diathesis.3
Of at least four distinct laboratory markers of B12 status, it is the total abundance of B12 in serum that has habitually been used for many years by the majority of laboratories. However, automated assays for holotranscobalamin (marketed as ‘active B12’) have recently become available offering an alternative approach for the evaluation of B12 status. Holotranscobalamin is the form of B12 taken up by cells to meet metabolic demand.
Assays for sensitive functional markers of B12 status, such as the determination of total homocysteine (tHcy) and methylmalonic acid (MMA) in serum, have also been automated. These can be used to detect subtle disturbances in B12-dependent metabolic pathways that stem from B12 insufficiency several years before deficiency-induced pathologies materialise. Unfortunately, it is not yet possible to reliably triage which asymptomatic patients flagged as B12-insufficient using contemporary laboratory diagnostics will ever go on to develop a deficient state of clinical significance. This dilemma is illustrated by a 1.0–3.9-year follow-up study of 432 individuals not treated with B12 after an initial observation of an elevated MMA concentration (defined in the study as >280 nmol/L) showed a longitudinal variation in levels of 34%. As the study progressed, a substantial increase in MMA concentration was detected in only 16% of participants, whereas 44% showed a decrease.4 The imperfect prognostic utility of MMA is set against the readiness with which B12 insufficiency may be corrected, and an increasing emphasis in healthcare on disease prevention rather than disease treatment. Low-dose preparations of B12 are available; for example, oral cyanocobalamin (BNF, 50 μg) is licensed within the UK and may ‘normalise’ laboratory markers of B12 in patients,5 with the caveat that it is essential to guard against the suboptimal treatment of latent and emerging pernicious anaemia.5
Laboratory markers of vitamin B12 status
A progressive decline in B12 status initially decreases the abundance of holotranscobalamin in the circulation. Subsequently, tissue stores of B12 are used and begin to diminish, leading to impaired performance of B12-dependent pathways and elevations in serum concentrations of the metabolites tHcy and MMA. Ultimately, an advanced deficient state manifests pathologically. The serum concentration of B12 responds slowly to a deterioration in B12 status.
First-line assessment of B12 status in the laboratory
The serum B12 and holotranscobalamin assays have both been highly automated using competitive binding luminescence technologies, making them suitable for the large-scale screening of B12 status in patient populations. tHcy assays are also available using these technologies but poor preanalytical sample stability limits utility. More rarely, automated MMA assays are available using liquid chromatography-mass spectrometry-based platforms.
Serum B12 assays
Screening of patients with macrocytic anaemia
The serum B12 assay is appropriate for the screening for B12 deficiency in patients with macrocytic anaemia. A serum B12 concentration below the lower limit of the laboratory reference range is sufficient to diagnose B12 deficiency.5 ,6 In these patients, the abundance of B12 has decreased to a point at which DNA synthesis has become impaired and cell nucleus maturation impeded.7–10 The net impact of these pathological changes may be an increase in the mean red cell volume (MCV) of up to 130 fl. If on investigation a serum B12 concentration within or above the reference range is found, then folate deficiency should be considered since it is the interplay between folate and B12 that is responsible for the megaloblastic anaemia seen as a consequence of both vitamin deficiencies. B12-independent causes of an increase in MCV have been widely described.9 A coexisting iron deficiency or thalassaemia trait complicates interpretation because macrocytic changes may be masked.9
Utility as a screening test in mixed patient populations
The majority of patients with suspected B12 deficiency do not have anaemia—and it is these patients that present the greatest diagnostic challenge. Common neurological symptoms include symmetric paresthesias, numbness and gait problems.3 ,11 It is not known why the severity of megaloblastic anaemia does not correlate with neurological dysfunction.3 ,11 Other symptoms of B12 deficiency include pallor, oedema, pigmentary changes in the skin, jaundice, impaired vibration sense, impaired position and cutaneous sensation, ataxia and weakness. It is essential to note that because serum B12 assays provide an estimate of total B12 abundance rather than direct evidence of metabolic utilisation, it is not possible to confidently exclude B12 deficiency when results fall in the indeterminate range of 125–250 pmol/L. This inherent limitation is clearly evidenced by the evaluation of a serum B12 assay for the detection of B12 deficiency against an MMA cut-off of 750 nmol/L (a concentration indicative of ‘definite’ B12 deficiency) in which sensitivities of ∼35% and ∼85% were found at 125 and 250 pmol/L, respectively. The corresponding assay specificity was ∼95% and ∼45%, respectively.12 To put this into context, the lower serum B12 cut-off for diagnosing B12 deficiency is typically set at ∼148 pmol/L (200 ng/L).13 In practice, detectable disturbances in metabolic networks consistent with possible B12 deficiency occur as high as 300 pmol/L.14 Up to 45% of B12-deficient patients may be overlooked when serum B12 assays are used in isolation.14 Further investigation using a second-line test is necessary for serum B12 results that fall within the indeterminate range.
Physiological variation in serum B12 concentration and impact on result interpretation
The difficulty of establishing B12 status during pregnancy serves to emphasise commonly faced, but not universally recognised, physiological changes that impact on serum B12 assay result interpretation. The recommended daily allowance for B12 increases during pregnancy from 2.4 to 6.0 μg/day, but a commonly seen decrease of almost 50% by the third trimester in serum B12 levels is more likely to be a consequence of haemodilution and a fall in the abundance of haptocorrin, one of the two primary B12-binding proteins, than signalling a tissue deficiency as a consequence of increased demand.15 Although a corresponding small increase in MMA levels may also be seen during pregnancy and post partum, authors question whether this is caused by an increased metabolic rate during pregnancy and lactation rather than indicative of B12 deficiency.15
Variation in the abundance of B12-binding proteins occurs in the wider population too, with up to 15% of patients with low serum B12 likely to have a low haptocorrin level rather than B12 deficiency.
Interpretation results >1000 pmol/L
Serum B12 levels >1000 pmol/L are not uncommon. With the exception of ongoing B12 replacement regimens, an unexpectedly high concentration of B12 in serum can frequently be traced to changes in the abundance of B12 binding proteins.
An increase in the abundance of haptocorrin is a feature of some malignant diseases including chronic myeloid leukaemia, polycythaemia vera and some solid malignant tumours. This phenomenon has been exploited diagnostically with the abundance of B12-unsaturated binding proteins (unsaturated vitamin B12 binding capacity (UBBC)) used as a marker of fibrolaminar hepatoma.16 Manual methods to determine UBBC are available.17 The reference range for UBBC is 670–1200 ng/L;18 for plasma collected into EDTA-sodium fluoride, it is 505–1208 ng/L;19 for haptocorrin, 49–132 ng/L; and for transcobalamin, 402–930 ng/L.
An increased level of serum B12 can also be caused by the presence of autoantibodies against transcobalamin, which does not appear to be related to the development of B12 deficiency.20 High B12 levels may also be a consequence of immunoglobulin-complexed B12, resulting in assay interference.
Analytical challenges associated with serum B12 assays based on competitive binding luminescence technologies
Automated assays for the measurement of serum B12 are based on competitive binding luminescence technologies. In the presence of high-titre anti-intrinsic factor antibodies in serum from patients with pernicious anaemia, assays based on competitive binding luminescence technologies generate spurious results.21 A study illustrated failure rates of serum B12 assays in the analysis of samples from patients previously diagnosed unequivocally with pernicious anaemia. Also, 6 of 23 (26%) patients were missed by the Beckman Coulter Access assay, which used the UniCel DxI 800 Immunoassay System, 5 of 23 (22%) by the Roche Elecsys Systems Modular Analytics E170 and 8 of 23 (35%) by the Siemens Advia Centaur assay. 21
Assay calibration
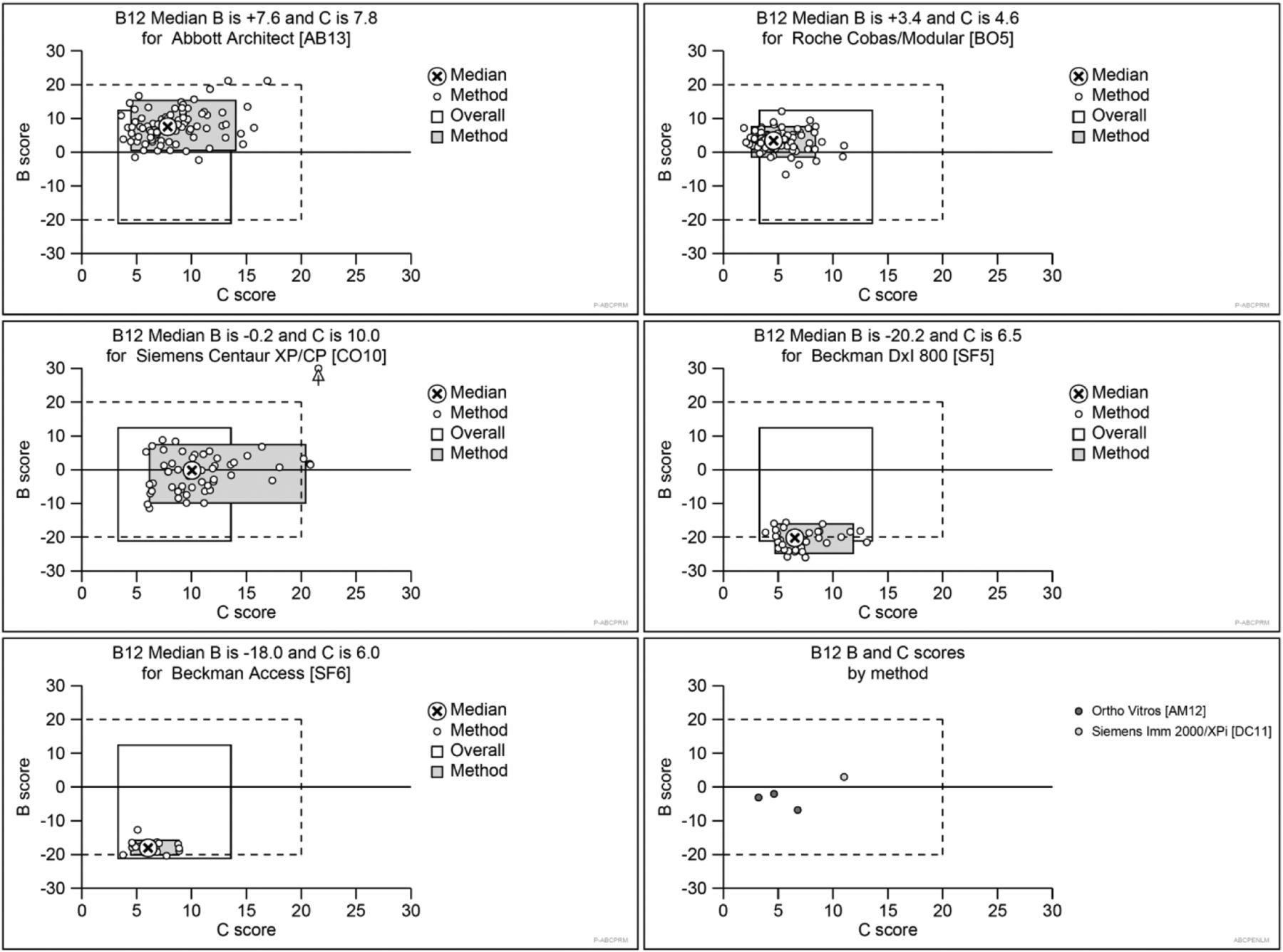
The use of assay calibrants that are traceable to metrological standards assists with assay harmonisation and the meaningful comparison of population data. The WHO International Standard for serum B12, 03/178, was ratified in 200722 as a consensus of B12 protein-binding assays. However, poor alignment of the seven main analytical platforms continues. Figure 1 shows consistent manufacturer-specific assay bias for serum B12 analysis. It is essential that laboratories adopt reference ranges that are compatible with their chosen platform.

Data from the UK NEQAS Haematinics Scheme showing performance calculated over a rolling window of 6 months (18 External Quality Assurance specimens circulated) by the seven analytical methods used for the analysis of vitamin B12 in serum. Methods clockwise from top left (UK NEQAS method abbreviation): Abbott Architect (AB13); Roche Cobas/Modular (BO5); Beckman DxI 800 (SF5); Ortho Vitros (AM12) and Siemens Immulite 2000/XPi (DC11); Beckman Access (SF6); Siemens Centaur (CO10). The B score is the average bias of all Specimen % biases [(result – target)/target]×100% during the rolling 6-month window. The C score is the SD of the B score and shows consistency of bias over the same rolling time period. The grey box indicates the 5th to 95th centiles for each method. The unfilled box indicates the overall 5th to 95th centiles irrespective of method. The dotted box indicates limits of acceptable performance defined as ±20% B score and 20% C score. All analyses were performed during 2015. With permission from Birmingham Quality, University Hospitals Birmingham NHS Foundation Trust.
Holotranscobalamin assays
Serum B12 assays are unable to discriminate between haptocorrin-bound (referred to as holohaptocorrin) and transcobalamin-bound (holotranscobalamin) B12. It is holotranscobalamin that is taken up via receptors to meet metabolic demand—holohaptocorrin and holotranscobalamin transport ∼0.1 and 4.0 nmol/day of B12 into cells, respectively.23 The adoption of holotranscobalamin assays,24–26 to determine the abundance of the physiologically active form of cobalamin,27 is increasingly widespread in Australia, Austria, Canada, Germany, Holland, Nordic countries, Switzerland and the UK. However, the mode of application is variable, that is, used as a sole status indicator,28 as a first-line screening test in conjunction with a second-line test24 and as a second-line test in conjunction with a serum B12 assay.29 Until recently, the automated ‘active B12’ assay was only available using the Axis-Shield/Abbott Architect assay from Abbott. However, in February 2016, Siemens launched the Centaur Active-B12 (AB12) assay for use outside of the USA.
Nexo et al 30 described a manual ELISA method permitting measurement of total transcobalamin and holotranscobalamin.23 This technique has been used to demonstrate that ∼10% of circulating transcobalamin is B12-saturated with a reference range of 5–20%; and that 15–50% of B12 is bound to transcobalamin. In B12 deficiency, transcobalamin saturation falls to 0.4–3%.18
Utility as a screening test in mixed patient populations
A holotranscobalamin concentration <25 pmol/L strongly suggests B12 deficiency. It is not possible to confidently exclude B12 deficiency for holotranscobalamin results that fall in the range 25–70 pmol/L. Further investigation using a second-line test is necessary. An evaluation of the holotranscobalamin assay for the detection of B12 deficiency against an MMA cut-off of 750 nmol/L showed sensitivities of ∼65% and ∼90% at 30 and 60 pmol/L, respectively. The corresponding assay specificity was ∼90% and ∼55%, respectively.12
Calibration
In response to the growing application of ‘active B12’ assays, a consensus value for holotranscobalamin was assigned in October 2015 for the WHO International Standard 03/178.31
Physiological variation in holotranscobalamin concentration
There is more to learn about the determinants of holotranscobalamin concentration in the circulation, in particular a better understanding of the relative influences of B12 metabolism and absorption is required.32 Clarity around which conditions, unrelated to B12, influence holotranscobalamin also merits further investigation.
Analytical challenges associated with holotranscobalamin assays based on competitive binding luminescence technologies
Some patients carry a rare variant in the transcobalamin gene (TCN2) that interferes with the ‘active B12’ assay.33 The minor allele rs35838082 (p.R215W) is rare in Caucasians with a minor allele frequency (MAF) of <0.01 but more common in South Asians (MAF ∼0.02) and those of African origin (MAF ∼0.25). Holotranscobalamin results for these patients are erroneously low (∼5 pmol/L) despite all other laboratory markers reported as normal, and an absence of clinical deficiency.33
Direct comparison of the holotranscobalamin and serum B12 assays
Direct comparison of the holotranscobalamin and serum B12 assays is not straightforward because no single gold standard laboratory marker of vitamin B12 status has been identified. However, receiver operator characteristic curves generated from a study in which subjects were defined as B12 deficient if they had a serum MMA >750 nmol/L showed holotranscobalamin to be a moderately more reliable marker of B12 status than serum B12 based on a greater area under the curve, 0.85 vs 0.76 (B12), and superior sensitivity and specificity.6
Second-line screening of vitamin B12 status
The inexorable link between assay sensitivity and specificity for both the serum B12 and holotranscobalamin assays, and the variable clinical sequelae of B12-deficient states leads to a wide indeterminate range. A serum B12 concentration between 125 and 250 pmol/L and a holotranscobalamin concentration between 25 and 70 pmol/L merits investigation using functional laboratory markers that provide an indication of cellular B12 utilisation.34 ,35
Total homocysteine: an indicator of methylcobalamin-dependent methionine synthase function
In man, two different forms of B12 (methylcobalamin and adenosylcobalamin) act as coenzymes for two different reactions.35 In one, methionine synthase requires methylcobalamin for the remethylation of methionine from homocysteine. In the laboratory, tHcy is readily determined by a variety of automated analytical techniques. In countries where the addition of folic acid to all enriched cereal grain foods is mandated, an elevation in tHcy >20 µmol/L, with normal renal function, may indicate methionine synthase dysfunction in response to suboptimal B12 (methylcobalamin form) availability.36 Since cobalamin methylation, that is, optimal formation of methylcobalamin, is dependent on the supply of 5′-methyltetrahydrofolate, in countries without mandatory folic acid fortification the diagnostic utility of tHcy is limited unless it can be established that the patient is folate replete. 5′-Methyltetrahydrofolate is a more powerful nutritional determinant of homocysteine (∼3.5 times) than methylcobalamin, and it is not until folate status has been optimised that B12 becomes the major determinant of homocysteine.37 Other, more modest, nutritional determinants of homocysteine include vitamin B6 and vitamin B2. 38 When interpreting tHcy results, it is recommended that age-specific and sex-specific reference ranges are applied. Examples from the author's laboratory include ≤13 and ≤15 μmol/L for females aged <60 years and males aged <64 years, respectively.39
Methylmalonic acid: an indicator of adenosylcobalamin-dependent methylmalonyl-CoA mutase function
In the second of the two B12-dependent reactions, methylmalonyl-CoA mutase uses adenosylcobalamin to convert methylmalonyl-CoA to succinyl-CoA. In B12 deficiency, excess methylmalonyl-CoA is hydrolysed to MMA. MMA is a useful marker of B12 utilisation, with some laboratories citing a serum concentration >280 nmol/L indicative of suboptimal status in patients <65 years with normal renal function.24 Interpretation is more challenging in the elderly and those with impaired renal function.40 An MMA concentration >750 nmol/L is generally accepted as indicative of ‘definite’ B12 deficiency.35 An automated LC-MS/MS assay for MMA analysis is available and capable of processing several hundred samples daily.41
Multiassay approaches to the laboratory diagnosis of vitamin B12 status
Mathematical models that combine multiple markers of B12 status into a single diagnostic indicator have been developed.42 The most sophisticated model uses all four most commonly available blood markers (a ‘four-variable’ analysis) to calculate a combined indicator of B12 status (cB12); where cB12 is expressed as cB12=log10[(holotranscobalamin×serum B12)/(methylmalonic acid×homocysteine)] (age factor). The formula transforms the four individual markers into a single variable dependent on age and is known as the ‘Fedosov's wellness score’. cB12 is interpreted as high–normal, normal, low–normal, deficient and severely deficient. ‘Fedosov's wellness score’ has recently been used to evaluate B12 status in non-anaemic healthy Swiss senior citizens.43
Recommended approaches for the laboratory assessment of B12 status
Although the application of a ‘four-variable’ analysis consisting of serum B12, holotranscobalamin, tHcy and MMA to generate Fedosov's wellness score provides a rigorous approach for the laboratory evaluation of B12 status, cost precludes its routine application. ‘Three-variable’ or ‘two-variable’ analysis approaches have also been evaluated and shown to estimate B12 status within acceptable margins of error compared with the ‘four-variable’ analysis.45
Recommended ‘three-variable’ analysis: serum B12, holotranscobalamin and MMA
Using models developed that calculate the Fedosov's wellness score based on the application of three assays being used in combination with a correction for folate on the model through its modulation of homocysteine,45 the best simulation of the ‘four-variable’ analysis is achieved through the combination of assays for serum B12, holotranscobalamin and MMA. tHcy should be omitted.
The next best ‘three-variable’ analysis is achieved by omitting either serum B12 or holotranscobalamin from the ‘four-variable’ analysis and combining the chosen assay with MMA and tHcy.45
Recommended ‘two-variable’ analysis: holotranscobalamin and MMA
The smallest ‘two-variable’ analysis error (compared with the ‘four-variable’ analysis) is observed when holotranscobalamin is combined with MMA.45 It is this approach that the author recommends for laboratory diagnosis of B12 status since an acceptable deviation from the ‘four-variable’ analysis is achieved without the expense of performing additional tests.
Example laboratory assessment algorithm
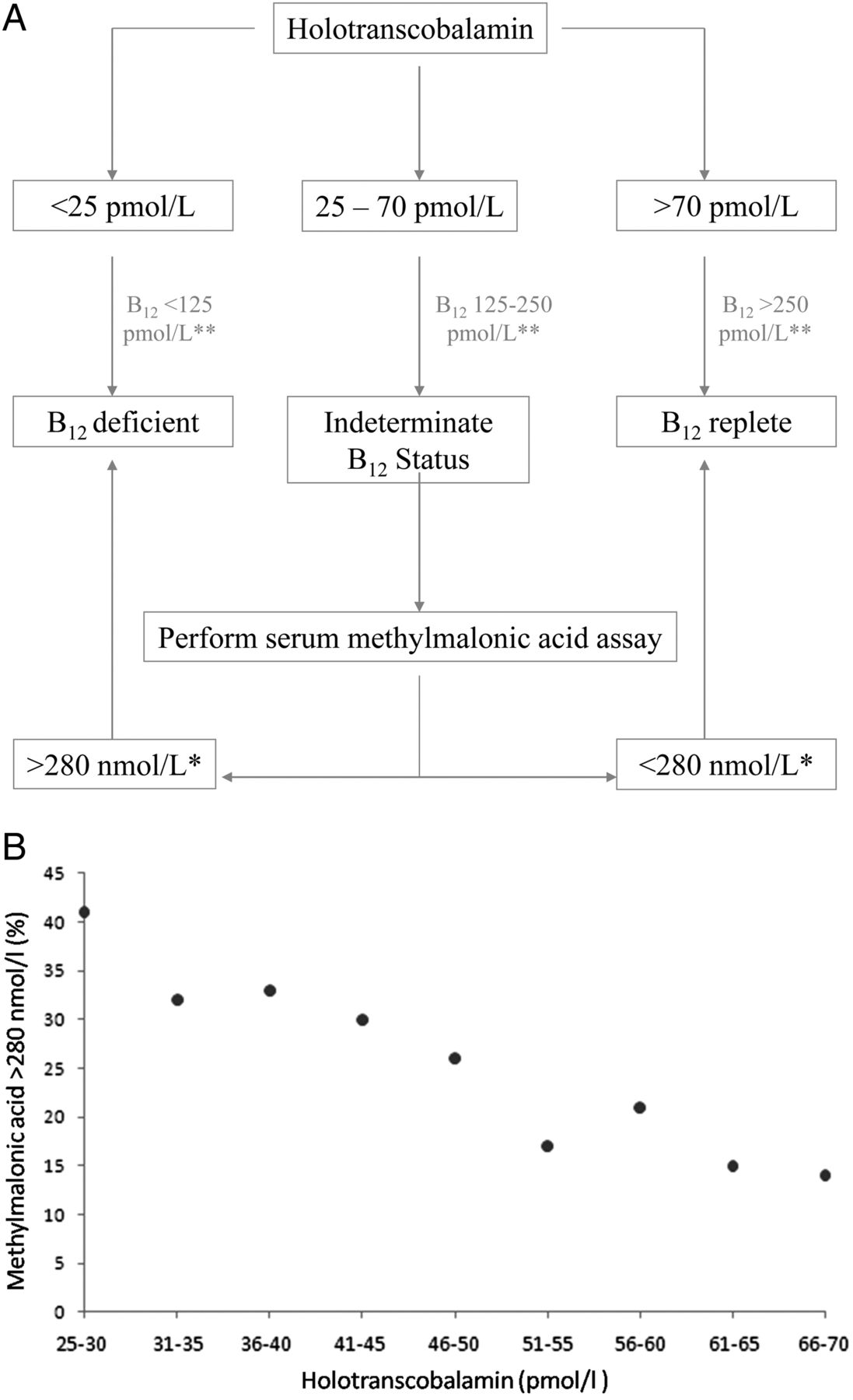
An example laboratory assessment algorithm that has been used extensively in the author's laboratory since 2012 that uses holotranscobalamin (first-line assay) with MMA (second-line assay) is shown in figure 2A. In laboratories where holotranscobalamin is not available, the recommended approach is serum B12 combined with MMA (figure 2A). Note that in the interest of economy in this example a sequential selection algorithm is followed, that is, whether a second-line assay is performed is dependent on the outcome of the first-line assay rather than both tests being performed on all samples. In the author's laboratory, ∼5% of samples from a mixed patient population have a holotranscobalamin <25 pmol/L and are classified as deficient; an indeterminate concentration of 25–70 pmol/L is measured in ∼25% of samples leading to second-line MMA analysis. All other samples are classified as replete. Figure 2B shows the percentage of samples from the indeterminate range subsequently defined as B12 deficient. Total prevalence of B12 deficiency in the mixed patient population is 10.8%.24

{kind=link}
{kind=link}
(A) An example laboratory assessment algorithm for vitamin B12 status assessment that uses holotranscobalamin and methylmalonic acid. *Cut-off applied to patients <65 years old with good renal function (a cut-off of >360 nmol/L applied to patients >65 years). **Previously suggested cut-offs for serum B12 from Hvas and Nexo.34 (B) Percentage of patients with a methylmalonic acid concentration >280 nmol/L as a function of holotranscobalamin concentration in a mixed patient population (n=3122).24 ,46 *A cut-off of >360 nmol/L applied to patients >65 years.
Identifying the aetiology of vitamin B12 deficiency
Schilling test
The withdrawal of radiolabelled cyanocobalamin and bovine intrinsic factor reagents for the Schilling test hampers the investigation of patients with B12 deficiency. The test consisted of up to four parts (part I, basic test; part II, with intrinsic factor; part III, following course of antibiotics; part IV, pancreatic enzymes taken for 3 days) in which the urinary excretion of radiolabelled B12 with and without intrinsic factor was established.47 ,48 Result interpretation was as follows: part I <5% labelled B12 excreted and part II excretion normal or near normal confirmed malabsorption as a result of lack of intrinsic factor (eg, pernicious anaemia); parts I and II abnormal, suggested malabsorption not resulting from intrinsic factor deficiency, for example, Crohn's disease; part III abnormal indicated abnormal bacterial grown. Part IV abnormal indicated pancreatic insufficiency.
As a sensitive marker of B12 malabsorption, holotranscobalamin levels that correct with small oral doses of vitamin B12 and the use of recombinant intrinsic factor could provide the basis for a non-isotopic B12 absorption test to replace the unavailable Schilling test. A sensitive B12 absorption test described by Nexo et al that relies on the holotranscobalamin assays (CobaSorb) to identify which patients may benefit from oral courses of B12 rather than the more commonly used replacement by intramuscular injection is available.49 The CobaSorb test involves measuring holotranscobalamin before and two days after daily intake of three times 9 μg B12 (cyanocobalamin form). The authors assigned a cut-off of >22% and >10 pmol/L to demonstrate active absorption with the caveat that it should not be used if the baseline B12 level is >65 pmol/L—in this situation, the C-CobaSorb test is suggested.50
Other laboratory assays that can be used to establish the cause of B12 deficiency include those for plasma-intrinsic factor antibodies; plasma-gastrin and pepsinogen; and plasma-parietal cell antibodies.
Two types of plasma-intrinsic factor antibodies have been detected in the plasma of >60% of patients with pernicious anaemia44 ,51 with type I blocking the binding of B12 to intrinsic factor and type II stopping the attachment of intrinsic factor or intrinsic factor-B12 complex to ileal receptors. Achlorhydria may be suspected by the presence of raised gastrin levels.52
Ninety per cent of patients with pernicious anaemia have gastric parietal cell antibodies, but specificity of this test is poor since they are also found in 15% of elderly subjects.
Summary
No single laboratory marker is suitable for the assessment of B12 status in all patients. The application of multiple markers, whether using a sequential selection algorithm or through the calculation of a single diagnostic indicator such as cB12, leads to a reduction in the number of B12-deficient patients who are overlooked. In the presence of discordance between laboratory test result and strong clinical features of B12 deficiency, it remains important to proceed with treatment to avoid neurological impairment.5
Acknowledgments
The author thanks Finlay MacKenzie and Aimee McGrory from UK NEQAS Haematinics for providing figure 1. The UK NEQAS Haematinics service is provided by Birmingham Quality, which is part of the University Hospitals Birmingham NHS Foundation Trust. The author is particularly indebted to Dr Malcolm Hamilton, Anne Lee and Sheena Blackmore for sharing their expertise. Thanks to Dr Agata Sobczyńska-Malefora for her work in establishing age-dependent and sex-dependent reference range for tHcy, Renata Gorska for assistance with the preparation of this manuscript, and to the wider team from the Nutristasis Unit at Guy's and St. Thomas' Hospital NHS Foundation Trust for the ongoing development and application of assays to establish vitamin status.
References
Footnotes
Handling editor Tahir Pillay
Twitter Follow Dominic Harrington at @DrDJHarrington
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.