Article Text

Abstract
Aims Any reference laboratory testing non-small cell lung cancer samples for predictive biomarkers needs to develop and validate a wide range of different molecular techniques, each with a specific time requirement and application. Updated international guidelines suggest that next generation sequencing (NGS) to be the initial procedure. However, in a non-negligible subset of cases, library generation may fail or amplicon coverage may be insufficient. In these NGS ‘invalid’ cases, the Idylla system may represent a viable option for rapid epidermal growth factor receptor (EGFR) genotyping.
Methods This retrospective study included 68 archival DNA samples previously processed by Ion Torrent NGS assay. Out of these, 43 cases, including 24 EGFR mutant samples, had a valid NGS result, whereas 25/68 (37%) were invalid. All samples were retested by directly pipetting the DNA inside the EGFR Idylla assay cartridge.
Results In all 43 cases with a valid NGS result, Idylla confirmed the EGFR mutational status. In particular, 24/24 (100%) of EGFR mutant samples as detected by NGS were confirmed by Idylla. Moreover, a large portion of cases (20/25; 80%) whose assessment by NGS was invalid were adequately processed by Idylla. Noteworthy, in 4/25 (16%) of cases, Idylla detected actionable EGFR mutations.
Conclusions Idylla assay could be very useful to quickly process cases for which NGS does not allow genotyping.
- lung cancer
- predictive biomarkers
- EGFR
- NGS
- Idylla
Statistics from Altmetric.com
Introduction
During the last years, treatment strategies in non-small cell lung cancer (NSCLC) have undergone considerable improvements due to the development of personalised therapies.1 In routine practice, testing tumour tissue for actionable genomic alterations requires a versatile approach, suitable for different types of samples and variable clinical contexts. Thus, ideally, any single molecular laboratory needs to develop and validate a wide range of different molecular techniques, each with a specific application. As an example, the ‘next generation sequencing’ (NGS) methodology is the best choice when testing is designed to detect a large number of different genomic alterations simultaneously2; the internal laboratory organisation may be optimised by adopting only one gene panel and single NGS workflow for all the different tumour types.2 However, NGS requires significant technical and bioinformatical skills, being cost-effective only in centres with a large volume of cases; in addition, NGS may have long turnaround times (TAT), both reflecting the need to batch samples before testing and to perform additional orthogonal techniques to confirm uncertain sequencing results. Conversely, in patients with NSCLC with acute clinical deterioration, the Idylla system (Biocartis NV, Mechelen, Belgium), based on fully automated real-time PCR, is very useful to provide rapid epidermal growth factor receptor (EGFR) genotyping.3 A single cartridge is required for any distinct case, which is ideal in low-volume testing laboratories. Moreover, the Idylla fully automated technology makes feasible to perform EGFR testing even in laboratories with little expertise in molecular biology. Remarkably, this technology can be reliably applied also to small tissue samples, including cytological samples.3 4 Recent investigation focusing on the relative performance of Idylla and NGS in lung cancer specimens showed that both approaches are accurate to detect actionable EGFR mutations.5 Thus, Idylla represents a viable alternative to NGS for rapid treatment choices in patients with ongoing acute deterioration, in particular when testing is performed on a less than optimal tissue specimen.5 Indeed, the success of NGS depends on multiple preanalytical factors, and it is well recognised that there is a positive correlation between the DNA yield and a successful NGS result.6 In particular, when NGS is carried out by the Ion Torrent semiconductor technology, the manufacturer’s recommended input amount is at least 10 ng. Although a subset of cases can be successfully sequenced even with a lower (<10 ng) DNA amount, literature data suggest that the percentage of cases failing in such cases is not negligible.6 7 Thus, laboratories may consider developing a complementary two-assay strategy: an initial NGS assay to detect all mutations of current and of potential clinical interest and, in case of NGS failure, when time to result is crucial, a very rapid assay for the actionable EGFR mutations, thus that a clinical report can be issued in a few hours. However, the performance of the Idylla in samples unsuitable for NGS evaluation has not been investigated yet. The aim of the present study is to define the role that Idylla can play in this setting.
Methods
Study samples
This retrospective study was designed to assess the relative performance of NGS and Idylla; to this end, we collected samples that had previously been processed by NGS. A sample prerequisite was the availability of a least 10 µL of archival extracted residual DNA. In order to collect a sizeable number of samples, cases were obtained from two institutions, the European Institute of Oncology (IEO), Milan, Italy and the University Federico II (FED II), Naples, Italy. These centres perform NGS as part of their diagnostic workup for the therapeutic management of patients with advanced stages of NSCLC. The NGS method is routinely carried out in both sites by an Ion Torrent personal genome machine platform (Thermo Fisher Scientific, Waltham, MA, USA). Although each Institution adopts a specific gene panel, a previous study showed that the assay performed at IEO (Oncomine Solid Tumour, Thermo Fisher Scientific) and that carried out at FED II (SiRe panel)8 detect EGFR mutations with a similar accuracy.9
On the overall, the study series included a total of 68 NSCLC archival DNA samples (IEO: number of cases=35; FED II: number of cases=33). Most of the DNA samples had been extracted from formalin-fixed paraffin embedded (FFPE) tissue sections (mostly 1 or 2) of 5–10 µm of thickness, whereas a minority (n=17) had been obtained from cytological samples. In any single case, DNA has been extracted by using a DNA Mini kit (Qiagen, Milan, Italy), following the manufacturer’s instructions, eluting in 30 µL final volume of nuclease-free water (not diethyl pyrocarbonate (DEPC) treated). In 24 archival DNA samples (IEO: number of cases=14; FED II: number of cases=10), NGS had shown EGFR mutations (table 1). Noteworthy, three cases, cases 2, 24 and 25, harboured a deletion of exon 19 associated with an exon 20 T790M mutation, whereas case 42 showed concurrent exon 18 E709K and exon 21 L858R mutations and case 47 displayed associated exon 18 G719A and exon 21 L861Q mutations. Conversely, in 19 cases NGS did not display any EGFR mutations. To meet the study aim, namely the performance of the Idylla in samples unsuitable for NGS, the sample set was enriched (n=25/68; 37%) in NGS unsuccessful cases (IEO: number of failed cases=10; FED II: number of failed cases=15). Reasons for failure of the NGS procedure included either absence of library generation or insufficient (<500 reads) EGFR amplicons coverage.
Study series including case number, patients’ gender and age, DNA concentration (ng/µL), testing site, NGS and Idylla results. MAF, as assessed by NGS, is also reported
Since EGFR mutational analysis is part of the routine diagnostic workup of patients with pulmonary lesions the need for ethic committee’s approval was not necessary for this study, in accordance with medical ethical guidelines of FED II and IEO. According to these guidelines, a comprehensive written informed consent was signed. All information regarding the human material was managed using anonymous numerical codes. All samples were handled in compliance with the Helsinki declaration (http://www.wma.net/en/30publications/10policies/b3/).
Idylla EGFR mutational test
Each Institution retested locally their subset of study samples by the EGFR Idylla assay. Although this procedure had been designed by the manufacturer to process 5–10 µm FFPE tissue sections, we have previously shown that archival extracted DNA can directly be pipetted inside an EGFR Idylla cartridge.4 Cases with valid NGS results were tested by pipetting 3 µL (corresponding to 1/10th of the original DNA preparation from the sample). Whenever possible, in NGS invalid cases the pipetted DNA volume was increased up to 10 µL of extracted DNA. Closing of the cartridge after inserting the DNA avoided cross-contamination. Via microfluidic channels in the cartridge, DNA was transported into five separate PCR chambers; these contained predeposited PCR reagents in dried form (ie, primers, probes, enzymes) designed for the qualitative detection of 18 types of genetic changes for which 51 different mutations have been validated. After 150 min run, final reports were directly available on the Idylla console and the results presented on screen as either ‘no mutation detected’ or ‘EGFR mutation detected’ were compared with those that had been generated by NGS.
Results
Overall, the study series included a total of 68 NSCLC archival DNA samples tested by NGS and retested by Idylla. Of these, 43 had a valid NGS result and were thus available for comparison with the result of the Idylla EGFR test. In 24/24 (100%) of EGFR mutant samples, Idylla confirmed the EGFR mutation as detected by NGS (figure 1). Mutation details are reported in table 1; in particular, concordance was also obtained in most (4/5; 80%) of the EGFR double mutant cases (cases 2, 24, 25 and 47); in case 42 Idylla only detected L858R and missed E709K (discordance by design). Similarly, in 19/19 (100%) of EGFR WT samples Idylla did not detect mutation, in full concordance with the NGS assessment.
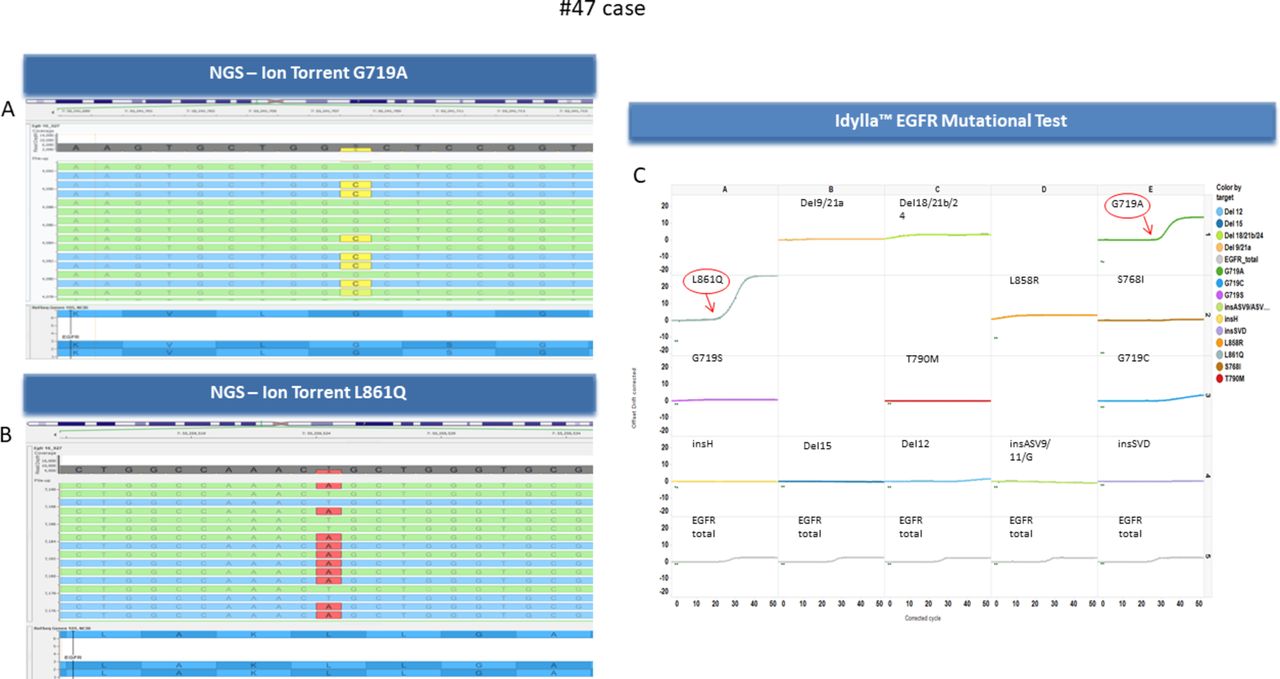
Case 47. Next generation sequencing (NGS) showed concomitant exon 18 G719A (A) and exon 21 L861Q (B) mutations. Idylla confirmed (C) the presence of both mutations (arrows). EGFR, epidermal growth factor receptor. EGFR, epidermal growth factor receptor; WT, wild type.
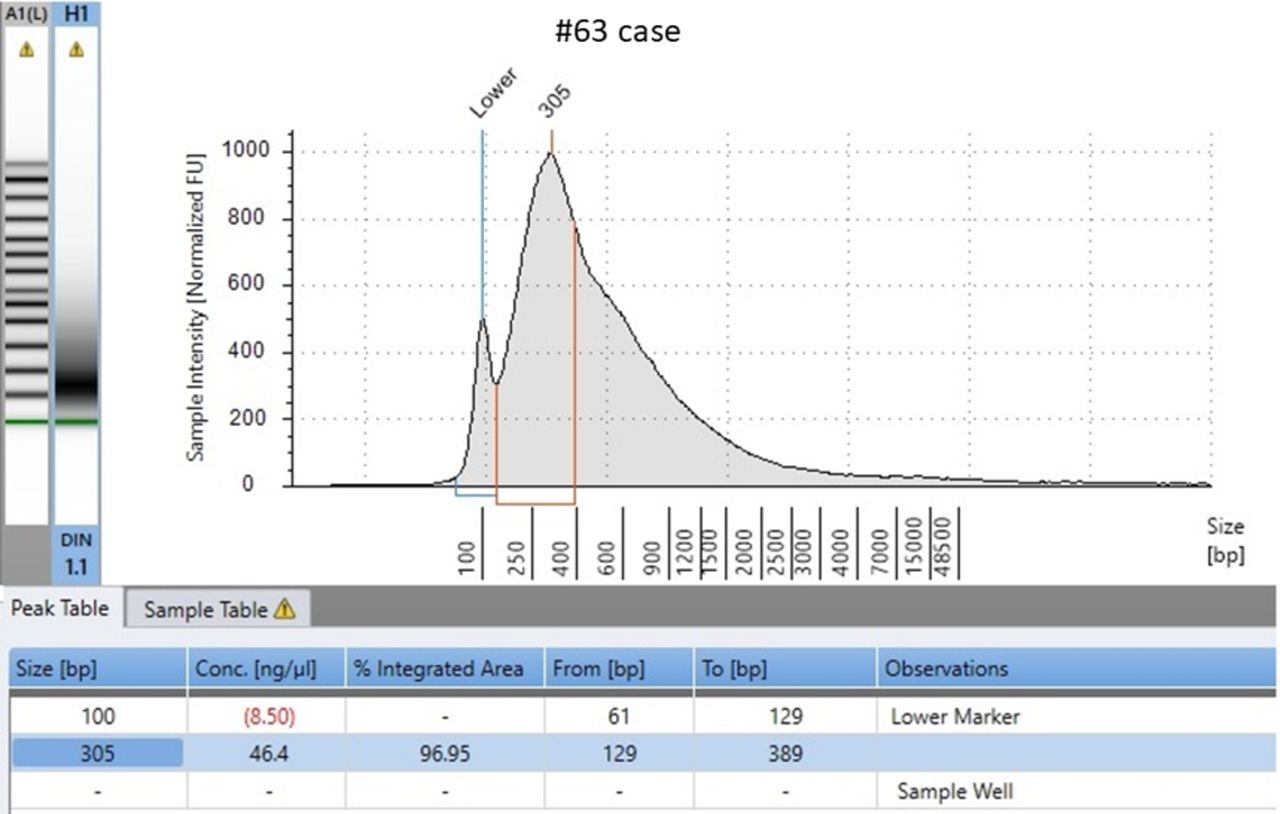
The Idylla performance was also evaluated in a relevant subset of cases (25/68; 37%), whose assessment by NGS was unsuccessful (table 1). On the overall, a large portion of these cases (20/25; 80%) were successfully processed by Idylla. This subset included 16 cases whose Idylla assessment was ‘EGFR no mutation detected’ (figure 2). Noteworthy, in a non-negligible portion (4/25; 16%) of cases whose evaluation by NGS was not contributive, Idylla detected actionable mutations. In particular, cases 27, 28 and 30 showed an exon 19 deletion, whereas case 33 showed an exon 21 L858R mutation. In five (5/25; 20%) instances (cases 59, 60, 61, 63 and 68) Idylla also gave an invalid result. Noteworthy, case 63 failed even if the DNA concentration was more than abundant (46.4 ng/µL), suggesting that there is no clear correlation between the amount of DNA extracted and the outcome of genotyping. This case was further investigated by a microfluidic platform based on electrophoretic system (4200 TapeStation, Agilent, Santa Clara, CA, USA) to assess the reason behind the failure. As it is shown in figure 3 the electrophoretic profile featured several peaks due to DNA fragmentation showing highly degraded DNA.

Case 66. In this case, next generation sequencing (NGS) (1) did not yield a contributive result, as amplicon coverage was insufficient (<500 reads). Conversely, Idylla (2) provided a valid result presented on screen as either ‘no mutation detected’. Real-time (RT) PCR curves for the successful amplification of the epidermal growth factor receptor (EGFR) total control DNA are shown (A–E). GC, Guanine/Citosine percentage.
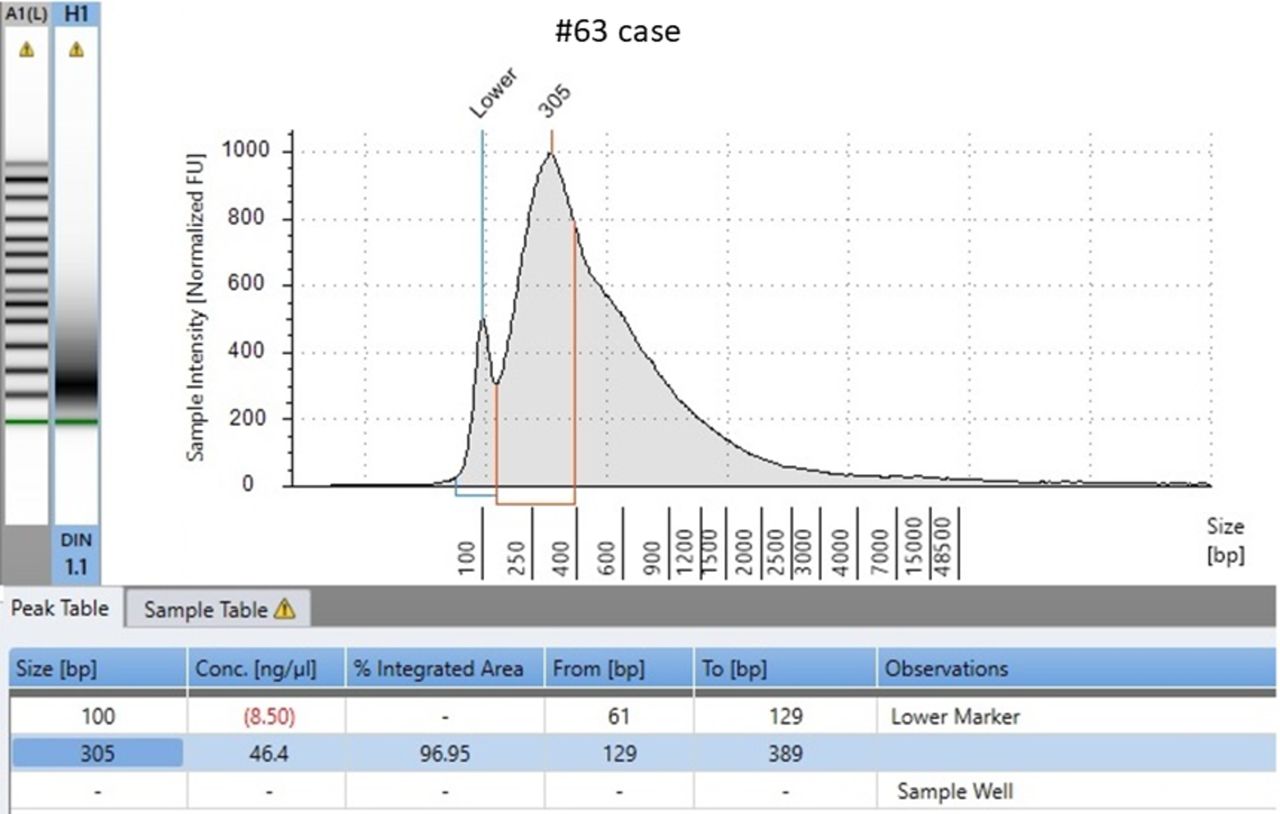
Case 63. Evaluation of DNA quality and quantity relative by a microfluidic platform based on electrophoretic system (4200 TapeStation, Agilent). The electrophoretic profile features highly fragmented DNA. The poor DNA integrity number (DIN value 1.1) explained how this case failed both when processed by next generation sequencing (NGS) and by Idylla. FU, fluorecence unit.
Discussion
This study data, besides confirming that NGS and Idylla are both accurate to detect EGFR activating mutations, show that the Idylla system is a viable option for rapid genotyping in NGS ‘invalid’ cases.
Although updated international guidelines represent the scientific backbone for lung cancer biomarker testing, they do not necessarily reflect real-world routine practice, as local issues require local solutions.10 Indeed, the standard of practice in large and comprehensive cancer treatment centres is far different from that of less specialised settings.10 The very recent revised guidelines from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology recommend that NGS panels should be preferred over single gene tests.11 Indeed, beyond EGFR also the BRAF, ERBB2 (HER2), KRAS and MET mutational status may be assessed by DNA-based NGS assays. Moreover, compared with sequential single gene testing NGS may be useful to spare clinical samples, whose abundance in neoplastic component is often limited, and, in clinical terms, to help patients find appropriate clinical trials.
However, while technology is advancing at a rapid pace and several DNA/RNA-based high-throughput technological solutions are emerging, currently NGS assays are often still limited to DNA alterations detection only, while most testing laboratories still strongly rely on immunohistochemical or fluorescent in situ hybridisation assays to detect ALK and ROS1 alterations.12 Thus, single gene testing methods are still acceptable to detect EGFR mutations provided that the recommended 10 working days’ TAT is met.11 In this setting, the timely communication between oncologists and molecular pathologists is crucial, in particular for acute deteriorating patient clinical management.5 Our data showed that, when clinical decisions should be taken quickly and when saving time is a crucial issue, since days have been spent for an ‘invalid’ NGS result, Idylla can provide a solution. As a general rule, regardless of the sample type, we directly pipetted in the cartridge from 3 up to 10 µL of extracted DNA preparation.4 Indeed, in this study, Idylla ‘rescued’ a large portion of cases (20/25; 80%) whose preliminary assessment by NGS was unfeasible (figure 4). Therefore, we propose an algorithm that could be used for clinical determination of EGFR mutational status Idylla, thanks to its capability of using only one FFPE slice as sample input, could be used in first line in settings, where due to low sample throughput, time to results would be an issue and sample batching could delay time to therapy initiation; alternatively, in settings where NGS analysis is performed to process a high volume of samples, NGS may be cost-effective in first instance for all samples. Even in these circumstances, the Idylla assay could be very useful to process cases with extensive DNA degradation for which NGS does not allow to make a conclusive diagnosis or when a short time to result is crucial for optimal patient management.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
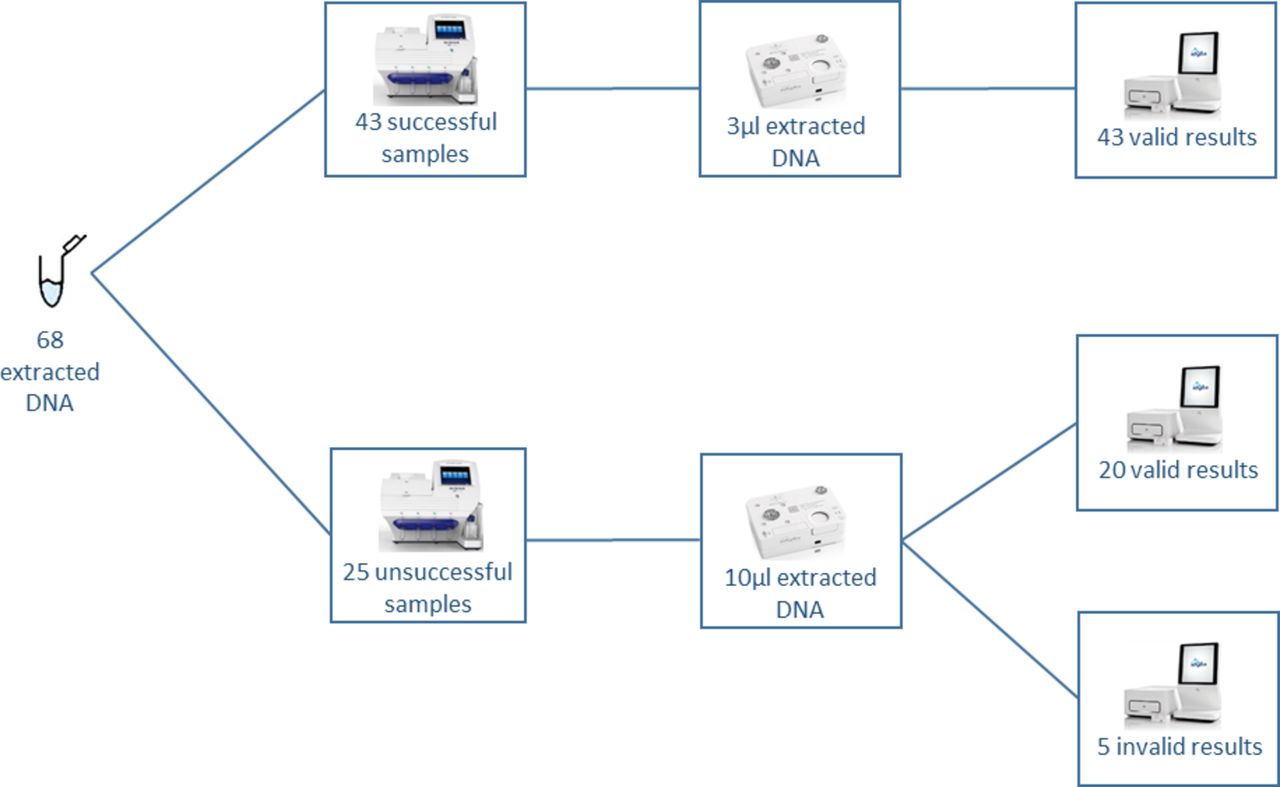
Study data summary. A total of 68 non-small cell lung cancer (NSCLC) archival DNA samples were retested by Idylla. Next generation sequencing (NGS) had been successful in 43 cases and unsuccessful in 25 instances. Depending on the NGS results, cases were retested by pipetting either 3 µL (NGS valid cases) or 10 µL (NGS invalid cases). In the 43 cases with a valid NGS result, Idylla confirmed the EGFR mutational status. Moreover, a large portion of cases (20/25; 80%) whose assessment by NGS was invalid were adequately processed by Idylla.
Take home messages
Although updated international guidelines suggest that next generation sequencing (NGS) to be the initial procedure, in a non-negligible subset of cases, library generation may fail or amplicon coverage may be insufficient.
A large portion of cases (20/25; 80%) whose assessment by NGS was invalid were adequately processed by Idylla for epidermal growth factor receptor (EGFR) genotyping.
In NGS ’invalid’ cases, the Idylla system is a viable option for rapid EGFR testing.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Footnotes
Handling editor Runjan Chetty.
Contributors CDL, GT and MB conceived the study and wrote the paper. GT and MB contributed as pathologists. CDL, AR, GG and UM performed the experiments.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.