Article Text

Abstract
Aims—In recent years there has been increased use of core biopsy for the preoperative diagnosis of screen detected and symptomatic breast lesions. The aim of this study was to compare the quality assessment parameters for preoperative diagnosis by fine needle aspiration cytology (FNAC) before conversion to core biopsy with those for core biopsy after conversion in screening and symptomatic practice. Accuracy of typing and grading of tumours on core biopsy was assessed.
Methods—Correlation of FNAC (C1–5) and core biopsy (B1–5) results (total of 1768 cases) with subsequent available resection histology was performed for 473 FNAC samples in 1997/98, 349 core biopsies in 1998/99 performed in symptomatic practice, for 561 FNAC samples in 1997/98, and 385 core biopsies in 1998/99 performed in screening. Quality assessment parameters were calculated using the methodology detailed in the National Health Service Breast Screening Programme guidelines for cytology practice.
Results—Increased absolute and complete specificity, lower inadequate rates, and lower suspicious rates were found for core biopsy compared with FNAC in both symptomatic and screening practice. Typing of tumours was attempted in 86.7% of core biopsies in symptomatic practice and was accurate in 93.6% (132 of 141 where type was stated). Grading of tumours was attempted in 63.5% of invasive carcinomas, with the provisional grade on core biopsy being confirmed on later histology in 75% of grade 1 cases, in 70% of grade 2 cases, and in 86% of grade 3 cases. No case provisionally graded as 1 was subsequently found to be grade 3 and no provisionally grade 3 case was found to be grade 1.
Conclusion—Conversion to core biopsy for the preoperative diagnosis of breast lesions increases specificity and reduces inadequate and suspicious rates. Grading and typing of tumours and assessment of oestrogen receptor status by immunocytochemistry is also possible in core biopsy, thereby increasing diagnostic information available when considering treatment options.
- breast carcinoma
- fine needle aspiration cytology
- core biopsy
- quality assurance
Statistics from Altmetric.com
The introduction of the National Health Service Breast Screening Programme (NHSBSP) more than a decade ago promoted the importance of preoperative diagnosis in the assessment of breast lesions. This preoperative diagnosis was achieved using triple assessment involving multidisciplinary cooperation between radiologists, surgeons, and pathologists. Preoperative pathological diagnosis was largely achieved by the use of fine needle aspiration cytology (FNAC), and systems were developed to allow continuous monitoring of the performance of the clinical modalities involved in the screening process.1 As units have compared their performance with the national breast screening quality guidelines some have used core biopsy rather than FNAC as a complimentary investigation for screen detected lesions. The published data suggest that the use of core biopsy has increased the preoperative diagnosis rate in screen detected breast cancers,2, 3 and there is evidence for more widespread use of core biopsy in the screening programme.4 The application of the techniques used in the screening programme by multidisciplinary teams for the preoperative diagnosis of women presenting with symptomatic breast disease has occurred over the past decade. Increased use of core biopsy for preoperative diagnosis has resulted from the introduction of spring loaded biopsy guns, which make core biopsy less traumatic for patients than FNAC, and the perception that core biopsy is more likely to give a definitive diagnosis for management. The purpose of our study was to document the changes in attainment of quality assurance standards that are associated with the conversion to core biopsy in symptomatic and screening practice. Previous publications have concentrated exclusively on screen detected practice.3, 4
Materials and methods
Material for pathological examination was obtained from 1768 consecutive and unselected patients as part of triple assessment. Four groups were identified:
-
Patients (n = 561) who had screen detected lesions investigated by FNAC before the conversion to core biopsy took place (1 October 1996 to 30 September 1998).
-
Patients (n = 473) presenting to a clinic with symptomatic breast disease investigated by FNAC before the conversion to core biopsy took place (1 October 1996 to 30 September 1998).
-
Patients (n = 385) who had screen detected lesions investigated by core biopsy after the conversion to core biopsy took place (1 January 1998 to 1 November 1999).
-
Patients (n = 349) presenting to a clinic with symptomatic breast disease investigated by core biopsy after the conversion to core biopsy took place (1 January 1998 to 1 November 1999).
Patients were assessed by clinical examination, imaging techniques (mammography and/or ultrasound), and pathological examination of samples obtained by the method considered the most suitable to the case. FNAC was performed using a 21 or 22 gauge needle and core biopsies with a 14 or 16 gauge needle. All the FNAC diagnoses were categorised into C1–5 using the criteria laid out in the NHSBSP guidelines for cytological reporting (table 1). The FNAC results were correlated with subsequent biopsy or surgical excision (if performed) and a matrix of this data was constructed (table 2) from which external quality assessment performance criteria could be calculated as specified in the NHSBSP guidebook.1 The absolute specificity was number of C5 diagnoses expressed as a percentage of the total number of carcinomas aspirated. This calculation assumes that all C5 cases with no histology were in fact malignant. The suspicious rate was C3 and C4 cases expressed as a percentage of all cases aspirated. Similarly, the needle core biopsies were categorised as B1–5 (table 1) and correlated with the subsequent histology on resection (table 2) and the performance parameters were calculated as for the FNAC results.
National Health Service Breast Screening Programme guidelines for radiological, cytological and core biopsy reporting
Correlation between preoperative diagnosis and subsequent diagnosis at treatment
For screening patients a preoperative malignant diagnosis rate was calculated as the number of carcinomas diagnosed by FNAC or core biopsy (C5 or B5) expressed as a percentage of all cancers diagnosed.
All patients had been discussed at a multidisciplinary meeting in which the radiological findings, clinical findings, and FNAC or core biopsy results were reviewed. Radiological assessment was formalised using a convention similar to that for pathology findings (table 1). Patients with C5 cytology and concordant clinical and radiological malignant findings proceeded to definitive treatment, either local excision or mastectomy. C1 aspirates were repeated. In some cases where radiological and clinical features were benign and the aspirator was sure that the area had been sampled, C1 was accepted as evidence of absence of malignancy. Patients with C2 or C3 diagnoses in which other modalities indicated a benign lesion were reassured. Patients with C3 or C4 diagnosis in which other modalities indicated a malignancy proceeded to further investigations. All patients with a B1 or B2 diagnosis in which other modalities (palpation, mammography, or ultrasound) were suspicious (R3, R4, or R5) were repeated. Patients with a B3 diagnosis (that is, benign histology but possibly associated with malignancy nearby) proceeded to open biopsy for definitive diagnosis. Those with B4 diagnoses were investigated further. A B5 diagnosis led to definitive treatment unless incompatible with clinical and radiological findings (R2) in which repeat core biopsy or diagnostic open biopsy was performed. In symptomatic practice, grading of invasive carcinomas was performed using the Bloom and Richardson method modified by Elston and Ellis.5
Results
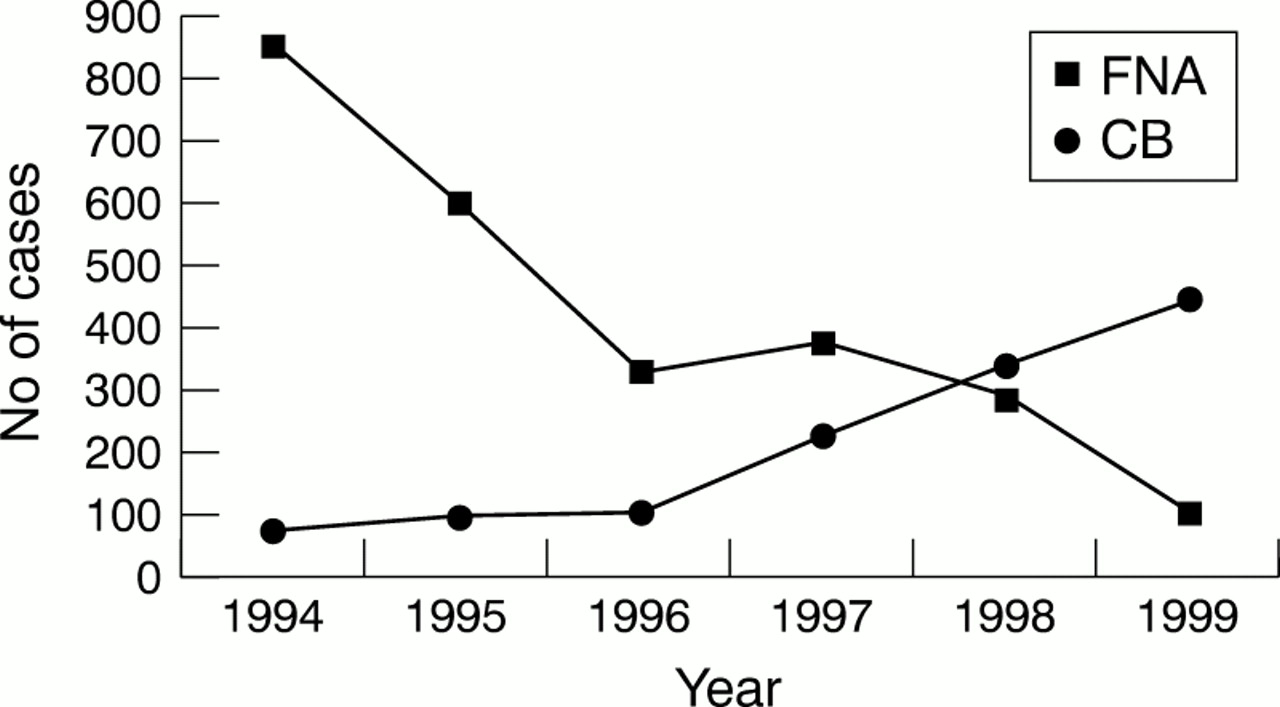
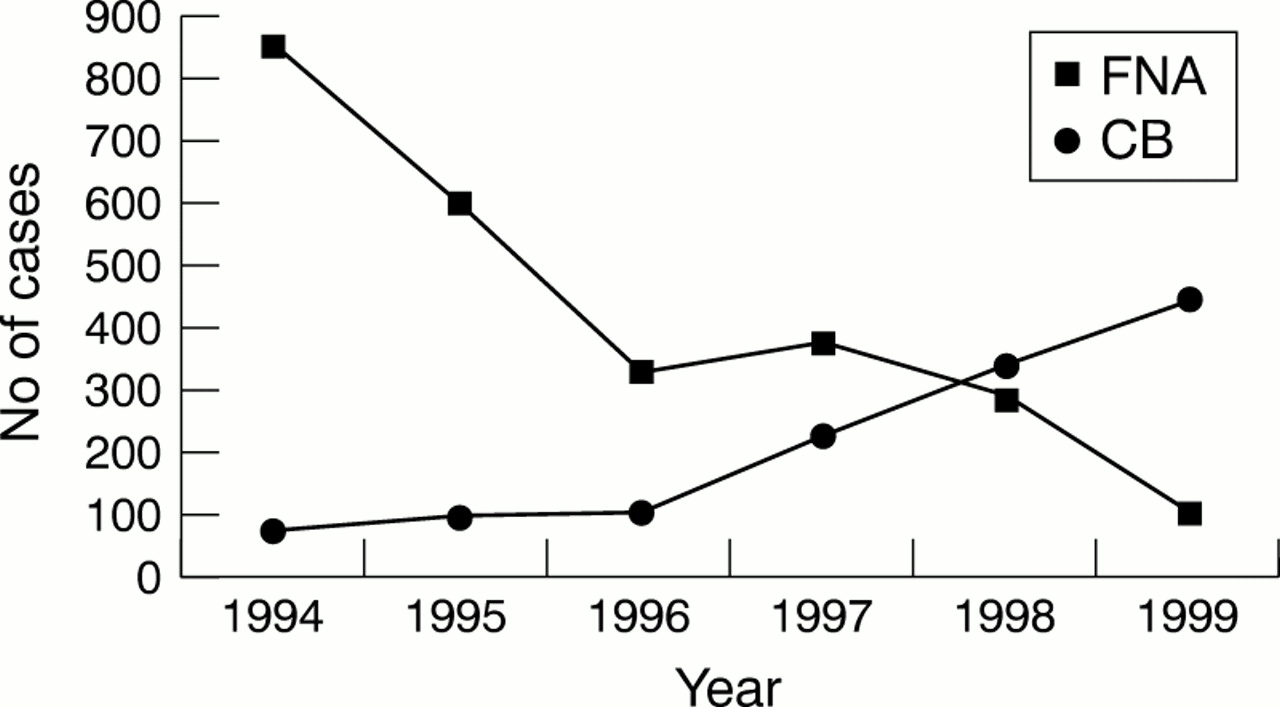
Figure 1 shows the numbers of FNAC and core investigations over time. Table 2 correlates investigation with subsequent histology. Table 3 shows the performance parameters calculated from these data in the four groups of patients identified. The main changes after the application of core biopsy to preoperative diagnosis are a pronounced increase in absolute sensitivity and complete sensitivity, with a reduction in inadequate rate and inadequate rate for cancer. There is also a reduced suspicious rate using core biopsy in both symptomatic and screen detected practice.
Performance parameters for the four groups of patients
{kind=link}
Graph showing numbers of fine needle aspiration cytology (FNA) and core biopsy (CB) investigations performed in screening practice by year.
In screening practice, the overall premalignant diagnosis rate (that is, C5 and B5) increased from 86% to 90% after the increased use of core biopsy.
In symptomatic practice, grading of invasive carcinomas was attempted in 63.5% of core samples and this provisional grade was confirmed on later histology in 75% of grade 1 cases, 70% of grade 2, and 86% of grade 3 cases (table 4). Typing of tumours was attempted in 86.7% of core biopsies and was accurate in 93.6% (132 of 141 where type was stated).
Comparison of provisional grades assigned to core biopsies with subsequent grades confirmed by histology
Discussion
Although FNAC and core biopsy have been promoted for rapid and accurate preoperative breast cancer diagnosis for many years, it is only relatively recently since the introduction of NHSBSP in the UK that the techniques have been widely applied, with monitoring of performance against national standards. Advocates of FNAC have highlighted the disadvantages of core biopsy. Histological processing is required, making it unsuitable for one stop clinics, which aim to give a diagnosis within one day, and core biopsy is a relatively expensive investigation because of the technical time involved in processing, cutting, and staining sections. The advantages of core biopsy are that histological sections are more readily interpreted by histopathologists leading to a “gold standard” result. Where malignancy is present, the presence or absence of invasion can be documented and the grade and type of tumour present can be assessed. Furthermore, it is possible to perform routine oestrogen receptor assays by immunocytochemistry on the tumour (although this is also possible with FNAC).6 This means that this important prognostic information is available to guide decisions regarding conservative management (wide local excision) or primary chemotherapy in selected patients.
In the past, preoperative diagnosis rates of less than 10% were reported in symptomatic patients and a questionnaire survey showed that clinicians (particularly surgeons) were reluctant to use the techniques.7 Analysis of figures available showed a lower suspicious rate for core biopsies (FNAC, 15%; core biopsies, 4%) but a higher inadequate rate for core biopsies (FNAC, 15%; core biopsies, 22%). Numbers in the study were small and imaging techniques were not used.7 Subsequent work has shown the potential of core biopsy in preoperative diagnosis of impalpable lesions and highlighted the cost savings compared with open biopsy.8–11 Preferential use of core biopsy in lesions difficult to diagnose by FNAC, such as lobular carcinoma, has been advocated.12 Review of preoperative diagnosis in screening practice has shown a continuing reliance on FNAC in most centres.4 Centres that have converted to the use of core biopsies in screening practice have reported a significant rise in preoperative diagnosis rates from 72% to 90%, which implies a worthwhile improvement in management of screen detected breast cancer.2 There are few comparative data on symptomatic breast practice.
The performance parameters presented here show better figures for symptomatic than screen detected practice. This would be expected because many screen detected lesions are small and impalpable and some types of lesion, rarely encountered in symptomatic practice, particularly microcalcifications and radial scars, may be difficult to sample by FNAC or core biopsies.13, 14 A recent overview of screening unit data showed a 16% increase in absolute sensitivity and a 14% fall in inadequate rate when core biopsies were used for preoperative diagnosis. 4 This overview shows a higher false negative rate for core biopsies, possibly as a result of patients being discharged after a benign core biopsy, which missed the adjacent carcinoma. This is not seen in our present study, perhaps as a result of ultrasound guidance and strict criteria for the acceptance of benign core biopsy results after correlation with other modalities at multidisciplinary meetings. Benign (B2) cores are repeated if there is clinical or radiological suspicion (R3, R4, or R5).
Our present study showed that conversion to core biopsy resulted in an increase in absolute sensitivity (from 59% to 89% in screening practice and from 70% to 99% in symptomatic practice), complete sensitivity (from 79% to 93% in screening practice and from 89% to 100% in symptomatic practice), and a fall in inadequate rate (from 32% to 21% in screening practice and from 35% to 5% in symptomatic practice). In screening, the overall malignant investigation rate (C5 and B5) or “preoperative diagnosis rate” for cancer increased from 86% to 90% with increased use of core biopsy. This is a modest improvement compared with that reported by others,2 but as can be seen in fig 1, both investigations were in use during the study period, and the switch to core biopsy was not sudden and complete. The other major change has been a reduction in the suspicious rate (C3 and C4 and B3 and B4 categories) from 14% to 5% in screening practice and from 13% to 3% in symptomatic practice. This implies that core biopsies are more likely to give a definitive biopsy result. This is an important advantage because “suspicious” pathology results at the multidisciplinary meeting often lead to an anxious wait for the patient, further investigations, and delay in treatment. In our study, there was one false positive core biopsy result, where a papillary lesion was interpreted as a papillary carcinoma, but on excision was a 2 mm intraductal papilloma, which reinforces the difficulty of interpretation and the usefulness of the B3 category. A second false positive core was interpreted as duct carcinoma in situ (DCIS), but on excision was found to be an adenomyoepithelioma with DCIS-like extensions at the periphery.
Previous reports indicate a lower inadequate rate for core biopsy and this finding is in accordance with the data presented here.2,3 The conversion to core biopsy as the investigation of choice in some centres for preoperative assessment of breast lesions means that the numbers of FNAC preparations will fall. This has two important consequences. First, the number of FNAC results that can be analysed for assessment against quality criteria may be too small to provide meaningful results, which can only be obtained if at least 200 aspirates are analysed. This means that analysis of data can only be performed perhaps on a two or three yearly basis, which will delay recognition of a problem with the unit's performance. It is also possible that FNAC will continue to be used at a much lower frequency for lesions that are anatomically placed such that needle core biopsy is considered risky or widespread sampling would be preferred. This selected use of cytology might result in non-representative figures in quality assessment. A further problem is loss of expertise in the assessment of cytology by pathologists because it is recognised that continuous exposure to cytological material is necessary to maintain expertise. These considerations raise the question as to whether FNAC should be abandoned altogether as a means of preoperative assessment if its occasional use in unusual situations may result in diagnostic error owing to loss of pathological expertise. One resolution to this dilemma is to perform both investigations on every patient, an approach that has been shown to yield better results than either modality alone. However, this means that patients have to undergo two invasive procedures and also increases pathology workload and costs.
Although the methodology for calculating the performance parameters for FNAC published in the NHSBSP cytology guidelines is robust, the quality standards set are probably inappropriate for core biopsy in screening practice and will require revision. The quality standards set for FNAC were derived from the results of surveys published in the literature and standards for core biopsy should be set in the same way. There are insufficient data available at present to allow a consensus on what are reasonable performance goals for core biopsy diagnosis. Results from other centres will help to define attainable standards, and modifications to the core biopsy diagnostic categories have already been proposed.15
Conclusion
Our study shows that conversion to core biopsy from FNAC in a single centre where that centre acts as its own historical control can result in increased absolute specificity, complete specificity, and reduced inadequate and suspicious rates in preoperative diagnosis in both screening and symptomatic practice.