Article Text

Abstract
Aims—To measure residual tumour in oesophageal adenocarcinoma treated with preoperative chemoradiotherapy, to correlate specific pathological variables with survival, and to describe morphological changes in tumour and non-neoplastic tissue resulting from preoperative treatment.
Methods—Resection specimens from 47 cases of oesophageal adenocarcinoma treated with preoperative 5-fluorouracil/cisplatin and radiotherapy were reviewed. Residual tumour was assessed in terms of tumour regression grade (TRG), pTNM stage, lymphovascular space invasion, and resection margin involvement. Survival analysis was performed using the Kaplan-Meier method and log rank test. Cox's proportional hazard model was used for multivariate analysis.
Results—A complete pathological response (TRG1) was present in eight cases. The absence of residual tumour was confirmed by negative immunohistochemical staining for MNF116. Tumour corresponding to TRG2 was present in five cases, to TRG3 in nine, to TRG4 in 22, and to TRG5 in three. By multivariate analysis, pN0 status (n = 35) had a positive effect on survival (p = 0.04) and TRG had no significant effect on survival (p = 0.06). Patients with pN0 tumours had a median survival of 48 months versus eight months for those with pN1 tumours (log rank test, p < 0.0001). We found that giant fibroblasts were discernible from single large residual tumour cells on haematoxylin and eosin alone.
Conclusion—Response to preoperative chemoradiotherapy in oesophageal adenocarcinoma is variable. Although there are as yet no reliable predictors of response to treatment, patients who are identified at diagnosis as having negative loco-regional lymph nodes should benefit considerably from this treatment approach.
- oesophageal adenocarcinoma
- preoperative chemoradiotherapy
- tumour regression
- prognosis
Statistics from Altmetric.com
The incidence of oesophageal adenocarcinoma has seen a dramatic increase in recent years.1–6 Similar to squamous cell carcinoma, the prognosis of adenocarcinoma is dismal, with a five year survival of approximately 20% after curative resection.7 Neoadjuvant chemoradiotherapy in addition to surgery for oesophageal carcinoma was shown to prolong survival in a prospective randomised trial from our unit8 and in some non-randomised trials.9–11 However, there remains considerable debate in the literature, and further randomised trials are needed before multimodal treatment can be established as the definitive approach. There is at present no accurate way of predicting which patients will benefit from this treatment approach and which will undergo potentially toxic treatment with little benefit.
Different grading systems for measuring residual tumour in oesophageal carcinoma after preoperative chemotherapy, with or without radiotherapy, have been described,12–15 but none has become universally accepted. It is still difficult to evaluate the true downstaging effect of neoadjuvant chemoradiotherapy in oesophageal carcinoma, even with the use of preoperative staging tools, such as endoscopic ultrasound.
We report a detailed histological review of oesophageal resection specimens from patients with oesophageal adenocarcinoma treated with preoperative chemoradiotherapy. We were interested in measuring residual tumour after treatment, and examining the effect of specific pathological variables on survival, in an attempt to derive prognostic information that might be relevant to pretreatment planning. We also detail the morphological effects of preoperative chemoradiotherapy on both tumour and non-neoplastic tissue.
Materials and methods
CLINICAL DETAILS
Forty seven consecutive resection specimens from patients with oesophageal adenocarcinoma treated with preoperative chemoradiotherapy were reviewed retrospectively. The surgical resections took place at St James's Hospital, Dublin between 1990 and 1996. The diagnosis of oesophageal adenocarcinoma was based on endoscopic biopsy material, the presence of greater than 75% of tumour above the gastro–oesophageal junction,16 and/or the presence of Barrett's mucosa. Preoperative investigations consisted of physical examination, chest x ray, abdominal ultrasound, barium swallow, and upper gastrointestinal endoscopy. Patients with detectable distant metastases were excluded. All multimodal patients received identical treatment consisting of 40 Gy radiotherapy in 15 fractions over three weeks. Either parallel opposed fields or oblique fields were used. Chemotherapy was administered in weeks 1 and 6 and consisted of 5-fluorouracil, 15 mg/kg body weight, for five days followed by cisplatin, 75 mg/m2, on day 7. Surgery was performed in week 8. Nine patients were women, 38 were men, with an average age of 64.5 years (range, 41–84; median, 68).
PATHOLOGY
Haematoxylin and eosin (H&E) slides were reviewed in all cases by two pathologists (BD and MG). Resected specimens were fixed in 10% buffered formalin. Where no obvious macroscopic tumour remained, the site of tumour seen at endoscopy was entirely submitted for histological examination. Full thickness transverse sections of the wall were taken. The mean number of block taken for each case was 10 (range, four to 17) and the mean number of tumour/ulcer blocks taken for each case was four (range, three to 10). Perioesophageal and greater and lesser curve lymph nodes were dissected where present and submitted separately for histology. The mean number of lymph nodes for each case was five (range, one to 17). Additional, separate, mediastinal lymph nodes were examined in four cases (mean, three; range, two to four). No lymph nodes were retrieved in three cases. Tumour regression was assessed using the tumour regression grading (TRG) system of Mandard et al as follows: TRG1, absence of residual cancer and extensive fibrosis; TRG2, rare residual cancer cells scattered through the fibrosis; TRG3, increased residual cancer cells but fibrosis still predominating; TRG4, residual cancer outgrowing fibrosis; TRG5, absence of regressive changes.14 Tumours were staged using the TNM staging system.15 The proximal, distal, and radial resection margins were assessed for the presence of microscopic involvement by cancer and positivity was denoted if tumour was present to within 1 mm of the margin. The presence of lymphovascular space invasion by tumour and histological subtype were also documented. Morphological changes in tumour cells and non-neoplastic tissue were described. Where no residual tumour cells remained (n = 8), we performed immunohistochemistry by the ABC method for MNF116 (Dako, Glostrup, Denmark; 1/50 dilution; pronase digestion) on the sections from the area where the tumour was located endoscopically.
STATISTICAL ANALYSIS
Survival was measured from the date of diagnosis to 1 December 1997. Survival analysis was performed using the Kaplan-Meier method and group comparisons were based on the log rank test. Multivariate analysis was performed using Cox's proportional hazards regression model.
Results
PATHOLOGICAL PARAMETERS
Thirty six tumours were adenocarcinomas, not otherwise specified, 10 tumours were mucinous carcinoma, and one was adenoid cystic carcinoma. Twenty six preoperatively treated tumours were classified as moderately differentiated, 20 were poorly differentiated, and one was well differentiated. These classifications were based on biopsy material pretreatment where little or no residual tumour remained in the resection specimen. A pathological complete response (TRG1) was seen in eight cases. Tumour corresponding to TRG2 was present in five cases, to TRG3 in nine, to TRG4 in 22, and to TRG5 in three. Tumour was staged as pT1 in seven cases, as pT2 in four, and as pT3 in 28. Thirty five cases were pN0 and 12 were pN1. Lymphovascular space invasion was present in seven cases, proximal and/or distal margin involvement was present in 13, and radial margin involvement was present in 12. Table 1 shows a comparison of the pathological parameters in patients with pN0 and pN1 tumours.
Comparison of pathological parameters in patients with pN0 and pN1 tumours
PATHOLOGICAL VARIABLES AND SURVIVAL
Median survival was 28 months in the overall group. By multivariate analysis many of the pathological parameters were interdependent. By this analysis, lymph node positivity was the most important pathological variable (p = 0.04) compared with tumour regression grade (p = 0.06) and pT stage (p = 0.07). When survival according to nodal status was examined, patients with pN0 status had a median survival of 48 months versus a median survival of eight months in the pN1 group (log rank test, p < 0.0001).
MORPHOLOGICAL CHANGES ASSOCIATED WITH TREATMENT
Changes in the tumour
The tumours showed extensive surface ulceration. Where little residual tumour remained, tumour cells were often dissociated and arranged singly, in short lines or tubules in a densely fibrotic stroma (table 2). The cells had very large nuclei often bizarrely shaped and multilobated. Nuclear chromatin in tumour cells was vesicular with large eosinophilic single or multiple nucleoli. The cytoplasm in the tumour cells was expanded and had a dense amphophilic quality with disappearance of cell borders and sometimes vacuolation (table 2; figs 1 and 2). All of the mucinous tumours showed residual intramural pools of mucin with admixed tumour cells arranged singly or in groups. When tumour cells were metastatic to loco-regional lymph nodes they did not show appreciable nuclear or cytoplasmic changes.
Treatment induced morphological changes in tumour cells

Tumour cells with large vesicular nuclei, some multilobated with multiple nucleoli and expanded and finely vacuolated cytoplasm (haematoxylin and eosin).

Tumour cells with large vesicular nuclei, some multilobated with multiple nucleoli and expanded and finely vacuolated cytoplasm (haematoxylin and eosin).
Stromal and vascular changes
Bizarre stromal fibroblasts were seen in 12 patients. These were documented when there were large elongated or angulated single nuclei with tapering basophilic cytoplasmic processes. Nuclear chromatin tended to be granular, nuclear membranes smooth, and the cells usually had single nucleoli (fig 3). There were large, atypical endothelial cells in granulation tissue underlying ulcerated tumour. Telangiectasia of submucosal vessels was common (n = 34; table 3). Thirty seven patients showed myxohyaline intimal proliferation of vessels, but no foamy plaques were seen within vessel walls (fig 4).
Treatment induced morphological changes in non-neoplastic tissue

Bizarre fibroblasts showing angulated nuclei, granular nuclear chromatin and tapering cytoplasmic processes (haematoxylin and eosin).
Vessels showing myxohyaline intimal proliferation (haematoxylin and eosin).
Non-neoplastic epithelial changes
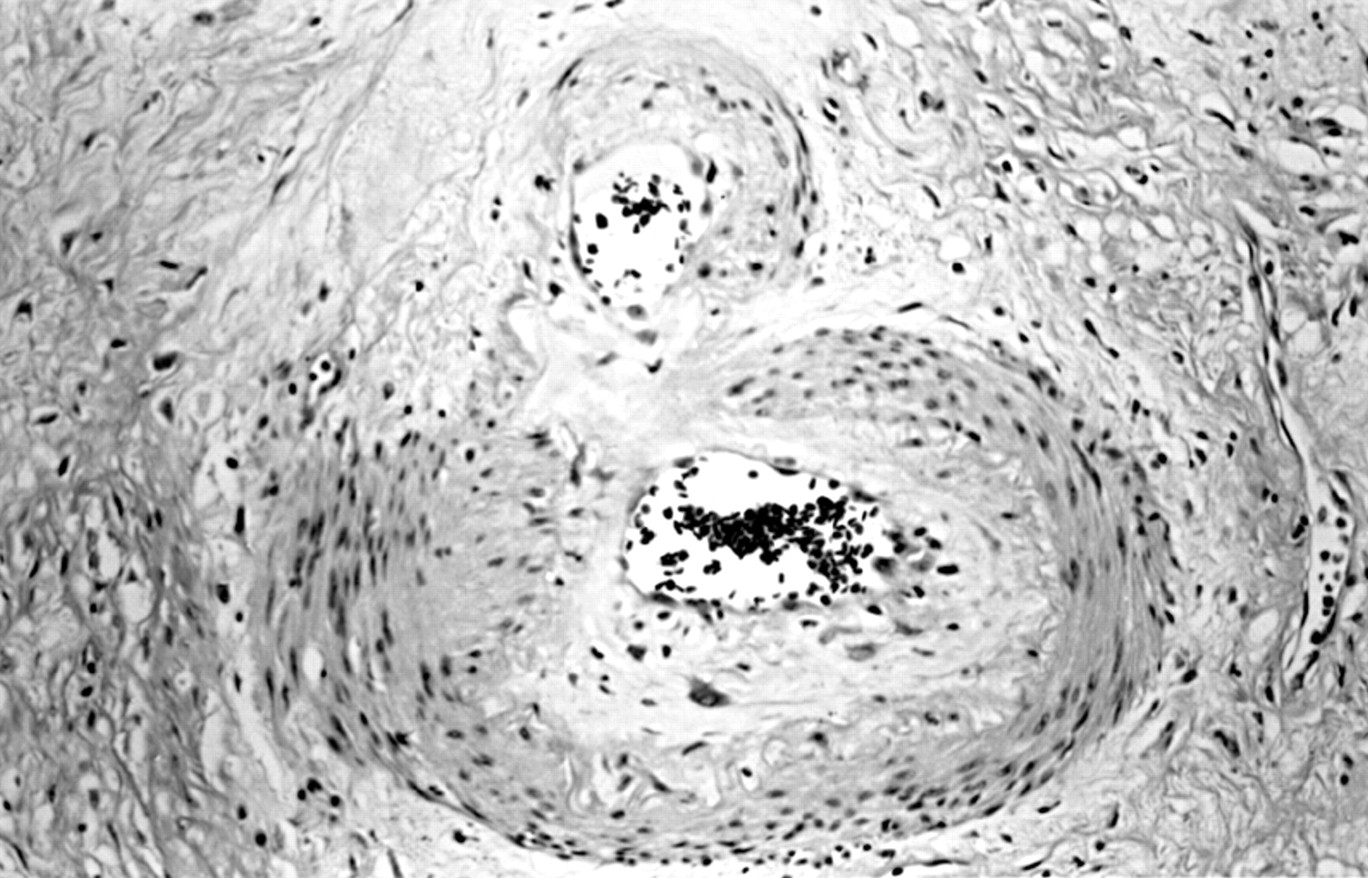
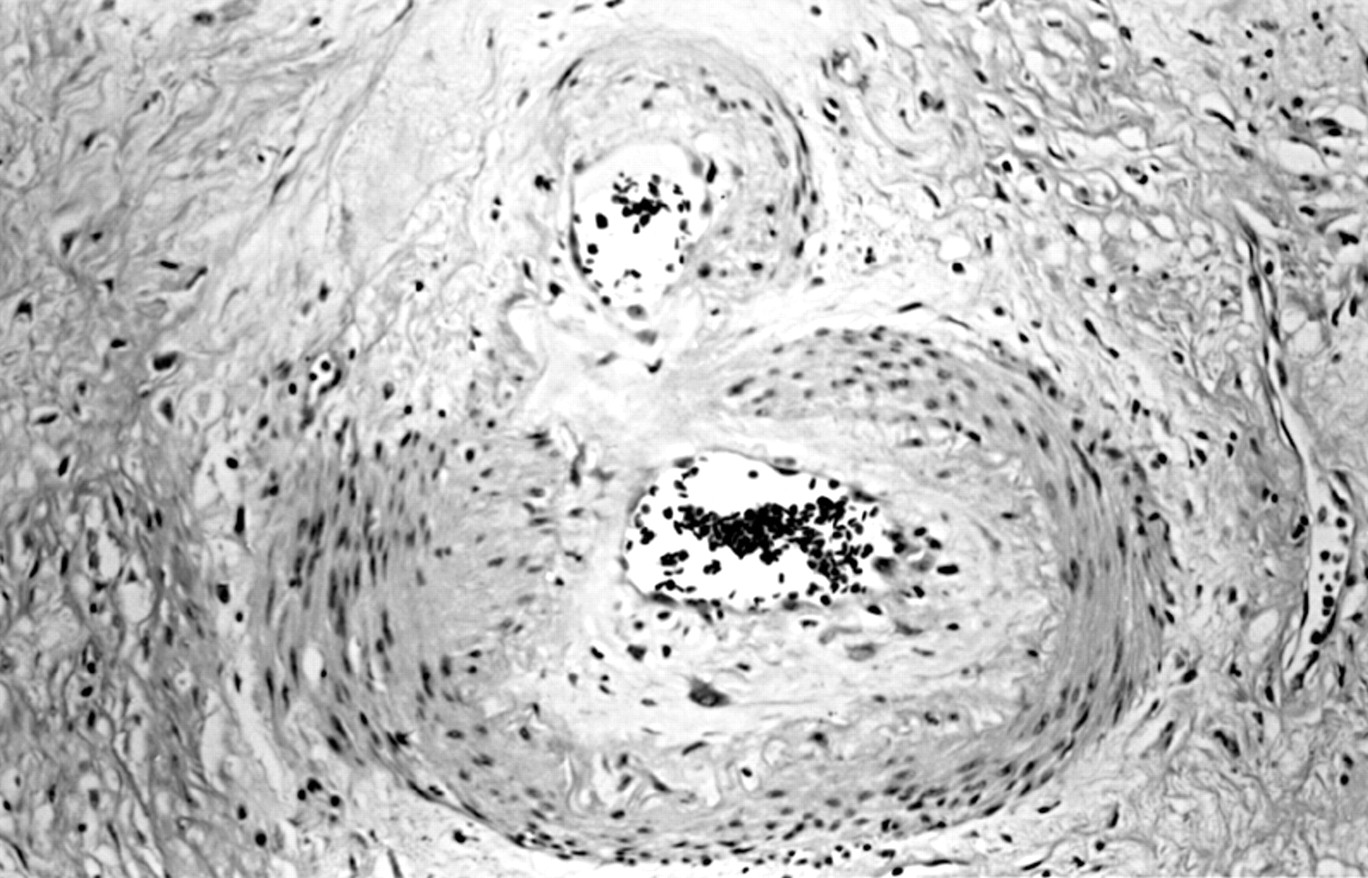
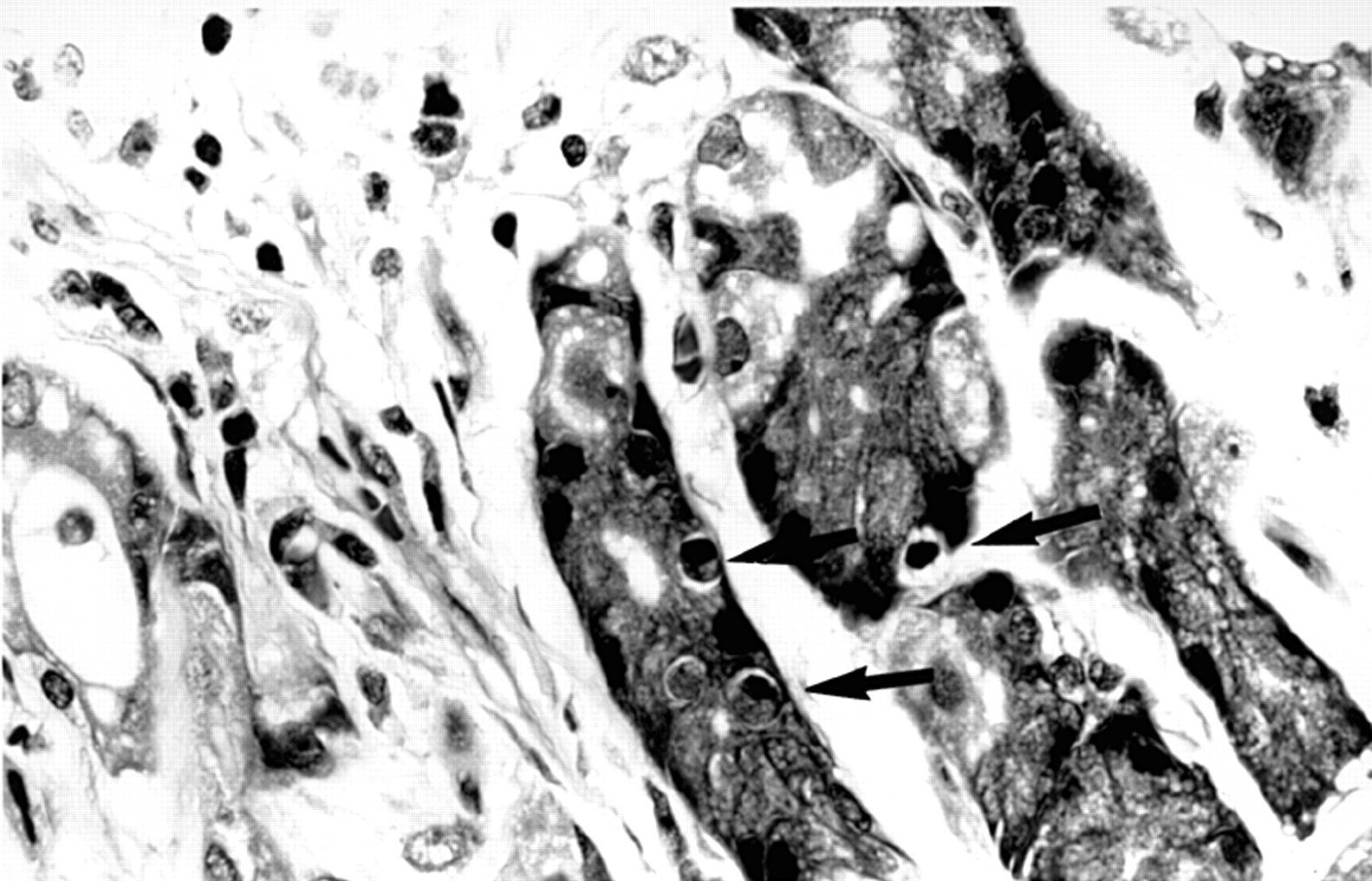
Specialised gastric mucosa (usually assessed at the distal margin) showed focal gland atrophy with angulation of glands, flattening of epithelium, and nuclear atypia. Gland lumina often contained neutrophils and cell debris. Apoptotic bodies were present in the parietal and chief cells of the lower third of the gastric epithelium (n = 14; table 3; fig 5). There was often a pronounced plasma cell infiltrate in the gastric mucosa and lymphocytes were commonly seen in squamous mucosa. Acanthosis of squamous epithelium away from tumour with exaggeration of surface folds giving a serrated appearance was noted (n = 22; table 3). Oesophageal submucosal mucous glands showed acinar atrophy and squamous metaplasia (n = 11) (fig 6). Squamous epithelium adjacent to tumour showed spongiosis, focal acantholysis, ballooning, and cystic degeneration of keratinocytes. These changes were felt to be ischaemic in nature. Glandular epithelium adjacent to tumour showed atypia which was interpreted as regenerative.

Apoptotic bodies (arrows) in specialised gastric glands (haematoxylin and eosin).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Squamous metaplasia and atrophy of oesophageal submucosal glands (haematoxylin and eosin).
Discussion
Although the role of neoadjuvant treatment for oesophageal carcinoma remains controversial, a randomised trial based at this centre demonstrated a significant survival benefit in patients who received multimodal treatment in resectable oesophageal adenocarcinoma over those treated by surgery alone. Other randomised clinical trials have not confirmed this survival advantage17,18 but many non-randomised trials, some of which include both adenocarcinomas and squamous cell carcinomas, have shown promising results. This is particularly true for patients who achieve a complete pathological response after treatment, who have repeatedly been shown to have a significantly longer overall survival.9,19–22 The response to neoadjuvant treatment is unpredictable, however, and there are no known pretreatment parameters that identify those patients who are sensitive or resistant to the neoadjuvant component.
In our series, in which we describe tumour regression in 47 adenocarcinomas of the oesophagus, we demonstrated a 17% complete response rate after multimodal treatment, which is comparable with other reports.10,23–25 By multivariate analysis, the only pathological variable that had a significant independent influence on survival was lymph node status. There was a sixfold and highly significant increase in median survival in node negative patients over those with positive nodes at the time of surgery. This concurs with the series of Vogel et al,10 where multimodal node negative patients had a significant survival advantage over all other patients. Unlike other reports,9,19–22 regression grade did not have a significant independent effect on survival (p = 0.06). T stage, lymphovascular invasion, and resection margin involvement were also interdependent with respect to survival.
Thus, in our series, patients with negative lymph nodes at surgery after preoperative chemoradiotherapy lived longer than those with positive lymph nodes, irrespective of other pathological variables. Endoscopic ultrasound was not performed on all patients so the number of patients who were node negative to start with and the number who were downstaged to a node negative status can only be speculated. We did not identify specific features of regression in regional lymph nodes that would identify this last subset of patients. We can, however, suggest that patients who are identified at the time of diagnosis as being node negative by endoscopic ultrasound will benefit greatly from preoperative chemoradiotherapy.
We used the regression grading system of Mandard et al for oesophageal carcinoma14 because it assesses residual tumour in relation to background fibrosis, which was very applicable to our series given the prominent fibrotic response that we noted in many of our cases. The system was reproducible and was predictive of disease free survival in their report. The Japanese Society for Esophageal Diseases was the first to describe a regression grading system for oesophageal carcinoma treated with preoperative radiotherapy or chemotherapy.12 Their system was based on whether viable tumour cells occupied more than one third of the entire tumour, less than one third, or were absent altogether. Other authors have used systems also based on the ratio of viable to necrotic tumour for assessing residual tumour after neoadjuvant treatment in head and neck carcinoma.26 In our series, we did not identify necrotic tumour cells, possibly because of a longer time between chemotherapy (weeks 1 and 6) and radiotherapy (up to week 3) and surgery at week 8. The residual tumour classification (R) following treatment was published first in 1987 by the UICC,15 where R0 represented no residual tumour, R1 microscopic residual tumour, and R2 macroscopic residual tumour. The advantages of this system are that it is simple and reproducible and has been validated in terms of predicting outcome. Similar to Mandard et al,14 we found that the gross diagnosis was not sufficiently reliable for us to use this system. Darnton et al used morphometric methods to measure the proportion of tumour to stroma in preoperatively treated oesophageal carcinoma.13 They based their analysis on one arbitrarily chosen microscopic field. However, we feel that microscopy of the entire tumour site is necessary for the accurate measurement of residual tumour.
We also report a qualitative description of the effects of preoperative chemoradiotherapy on tumour cells and non-tumoral tissue in oesophageal adenocarcinoma. Diagnostic difficulties can arise from overinterpretation of treatment related changes, such as in the case of single bizarre radiation fibroblasts mimicking carcinoma cells. We had no difficulty distinguishing single malignant cells surrounded by fibrosis from radiation fibroblasts on H&E because the former were larger with very irregular, vesicular, sometimes multilobated nuclei. The nuclear chromatin of the fibroblasts was more granular, the nuclear contour was angulated, and the cytoplasm fibrillary and tapering. Immunohistochemistry using the broad spectrum anticytokeratin antibody MNF116 was negative in eight cases where there were bizarre fibroblasts but no residual tumour detectable on H&E.
The changes in tumour cell morphology in the report of Mandard et al largely mirrored our own findings, apart from their descriptions of ghost keratinocytes and giant cell and granulomatous reactions to keratinous material,14 which we would not have expected given that our series only included cases of adenocarcinoma. They documented regression in metastatic loco-regional lymph nodes when they saw keratinous material or squamous ghost cells in dense fibrosis within lymph nodes. Sulfaro et al also described changes in tumour cells and stroma in lymph nodes as being indicative of regression in a series of squamous cancers of head and neck treated with preoperative chemotherapy.27 In our series, in contrast to descriptions of squamous cancers, we did not identify specific features in lymph nodes that we could attribute to regression. We found fibrosis and degrees of hyalinisation both in metastatic and non-metastatic lymph nodes, and tumour cells (when present) did not show nucleomegaly or alterations in cytoplasm.
In conclusion, there is a wide variation in the degree of tumour regression in patients with oesophageal adenocarcinoma treated with preoperative chemoradiotherapy. We demonstrated a 17% complete response rate in our series. Pathologically detected negative regional lymph nodes are associated with a significantly longer survival by multivariate analysis. We found no independent association between tumour regression grade and survival. We suggest that patients staged as node negative at diagnosis by endoscopic ultrasound have the prospect of an excellent result after preoperative chemoradiotherapy. Hopefully, in the future, the discovery of molecular markers that will predict response to treatment and outcome will help to tailor treatment to individual patients with this disease.