Article Text

Abstract
Aim—Despite the fact that gastric carcinoma continues to be one of the most common cancers world wide, only dysplasia in flat mucosa and adenomas have been shown to evolve into invasive carcinoma. The aim of this paper is to report a novel histological phenotype of gastric adenoma with early invasive growth.
Material and results—The patient presented with gastric complaints. A barium examination revealed an ulcerated tumour in the corpus, apparently infiltrating the gastric wall. The endoscopic examination showed a pediculated protruding tumour in the greater curvature. Punch biopsies were reported as invasive adenocarcinoma. Because of the poor condition of the patient, a partial gastrectomy was performed. The histological examination revealed elongated fronds with lateral crenated, saw tooth-like notches as a result of scalloped epithelial indentations. Areas with high grade dysplasia, with carcinoma in situ, and invasive carcinoma at the tip of the adenoma were demonstrated. The pedicle of the protruding neoplasia “emerged” from a non-protruding serrated adenoma.
Conclusions—The protruding serrated neoplasia had apparently evolved from a non-protruding serrated gastric adenoma. This appears to be the first case of gastric serrated neoplasia in the literature.
- gastric serrated neoplasia
- gastric carcinoma
- dysplasia
- gastric adenoma
Statistics from Altmetric.com
Early in 1923, Konjetzny1 reported the presence of polypoid changes in the gastric mucosa, and five years later Borrmann2 described different types of gastric polyps. In 1929, Stewart3 found 47 gastric polypoid lesions with mucosal aberrations—which he called adenomas—among 11 000 necropsies.
Since then, much attention has been centred in the literature around gastric adenomas,4–14 and several classifications have been proposed by different authors.15–19
The accepted microscopic structures described for those neoplastic gastric polyps have been either tubular, tubulovillous, or villous.4–19 Recently, however, while reporting surgical gastric specimens, we found a protruding neoplastic lesion with the phenotypic characteristic of a serrated adenoma, similar to those reported in the colon.20 Because a similar case of gastric serrated adenoma has been reported previously in the literature, it was considered of interest to describe its microscopic characteristics in this report.
The patient
The patient was a 78 year old woman. Thirty two years previously, she was treated with pelvic irradiation for a squamous cell carcinoma of the uterine cervix. For the past 10 years she had been treated for diabetes mellitus and hypertony. Two years ago the patient developed a gastric peptic ulcer, which was treated with medication. For the past week she had complained of profuse vomiting, weakness, tiredness, and dizziness. No haematemesis or melena were recorded. The laboratory reported moderate anaemia. A barium x ray examination of the stomach revealed an ulcerated tumour in the corpus, apparently infiltrating the gastric wall. The subsequent endoscopic examination showed a pediculated polypoid tumour in the greater curvature. Punch biopsies taken from the tumour were reported as invasive adenocarcinoma.
Owing to the poor condition of the patient, the surgeon considered a total gastrectomy too hazardous and, because the tumour was pedunculated (according to the endoscopist), he decided to perform a local excision. The patient had an uneventful postoperative period.
Pathology
The surgical specimen comprised a 10 cm in diameter gastric wall centred by a protruding pediculated polyp, measuring 4 cm in diameter. Part of its luminal border was eroded and covered with fibrin. The preparation was fixed in 4% neutral formalin.
After fixation, a 1 cm thick cross section of the entire preparation (through the largest tumour diameter, including part of the adjacent gastric mucosa) was imbedded in paraffin wax and processed for histology. The remainder of the tumour and the adjacent gastric mucosa in all four lateral directions were sampled in blocks.
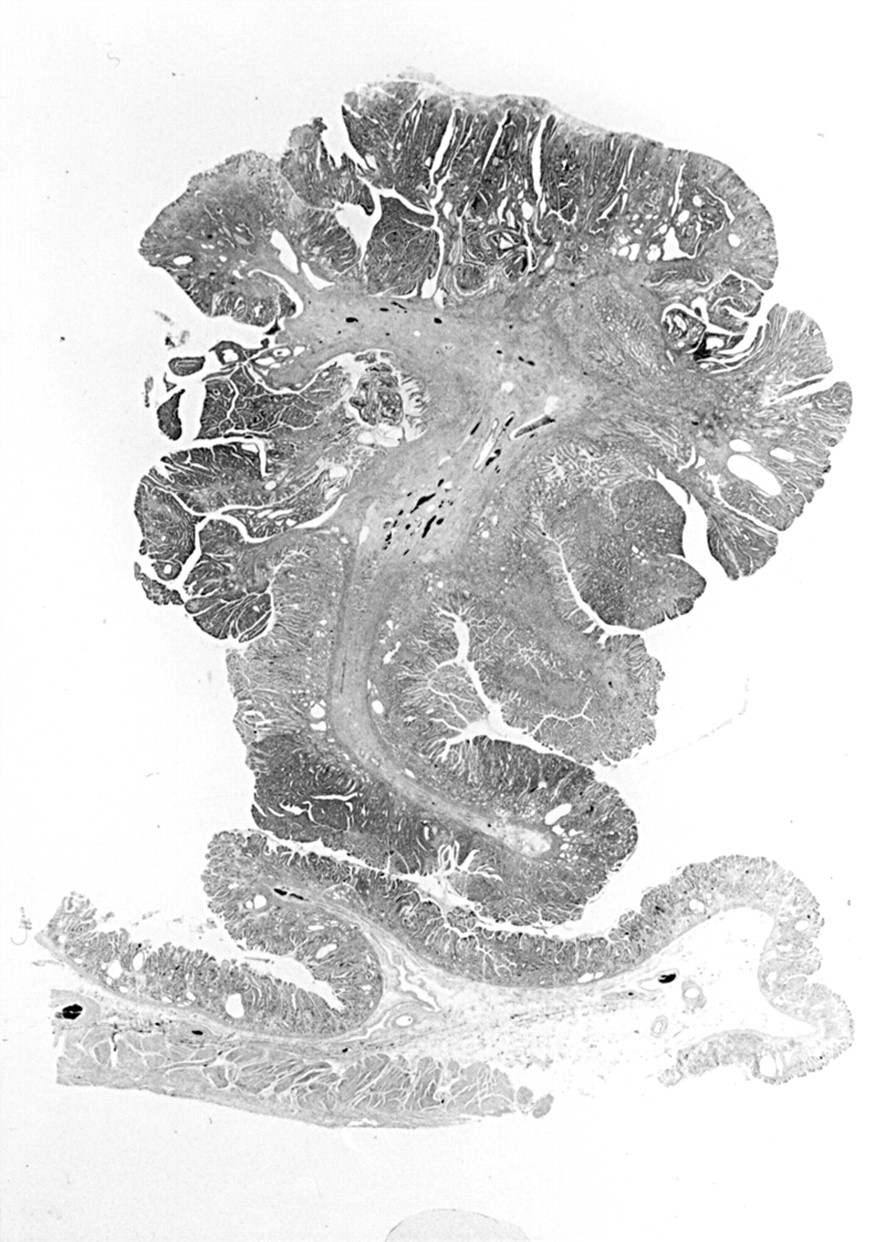
Macrosections (6 μm thick) from the large block were cut and stained with haematoxylin and eosin (fig 1) and for Ki67 (MIB1; Dako, Glostrup, Denmark), and p53 (DO-1, sc-126, L148; Santa Cruz, Santa Cruz, California, USA).

Macrosection showing protruding, pedunculated gastric neoplastic lesion (haematoxylin and eosin).
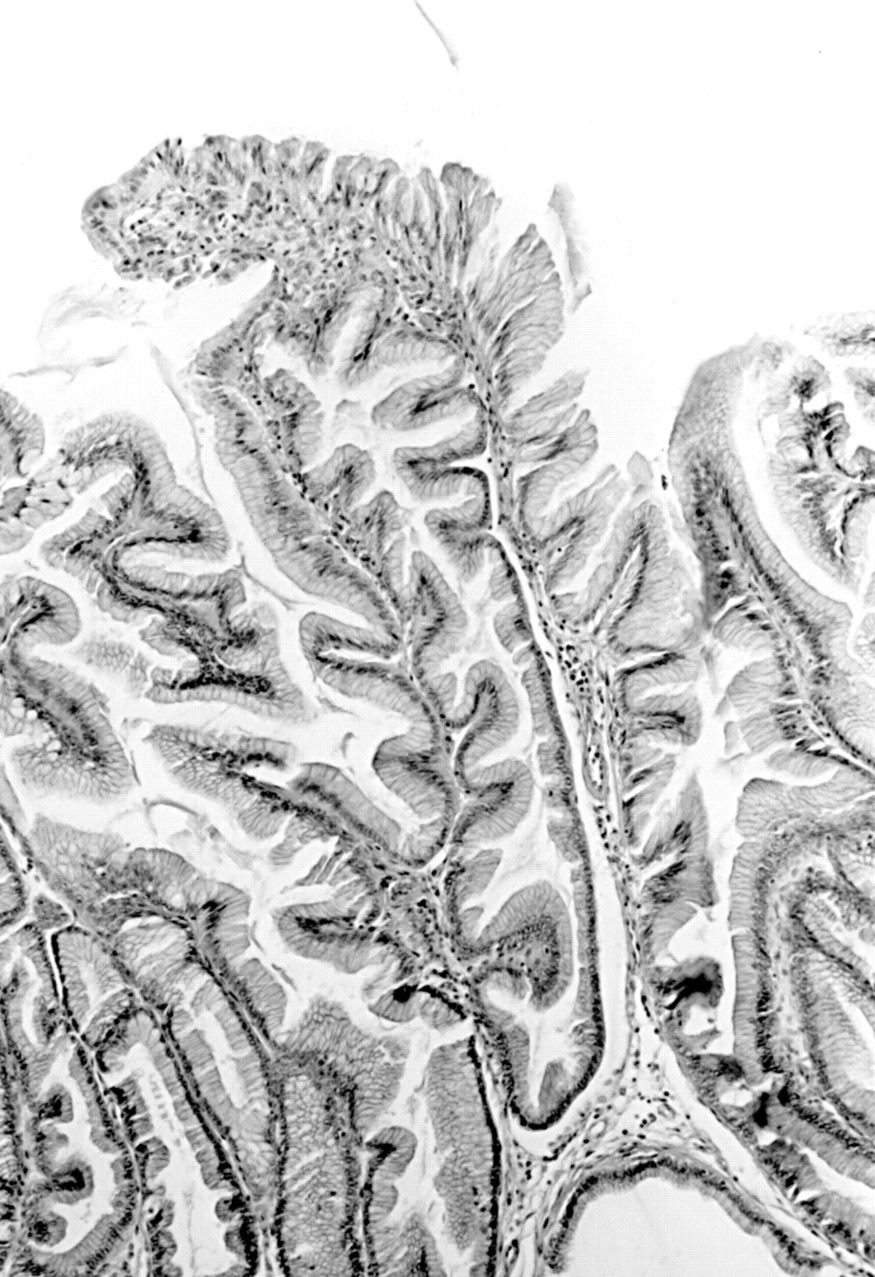
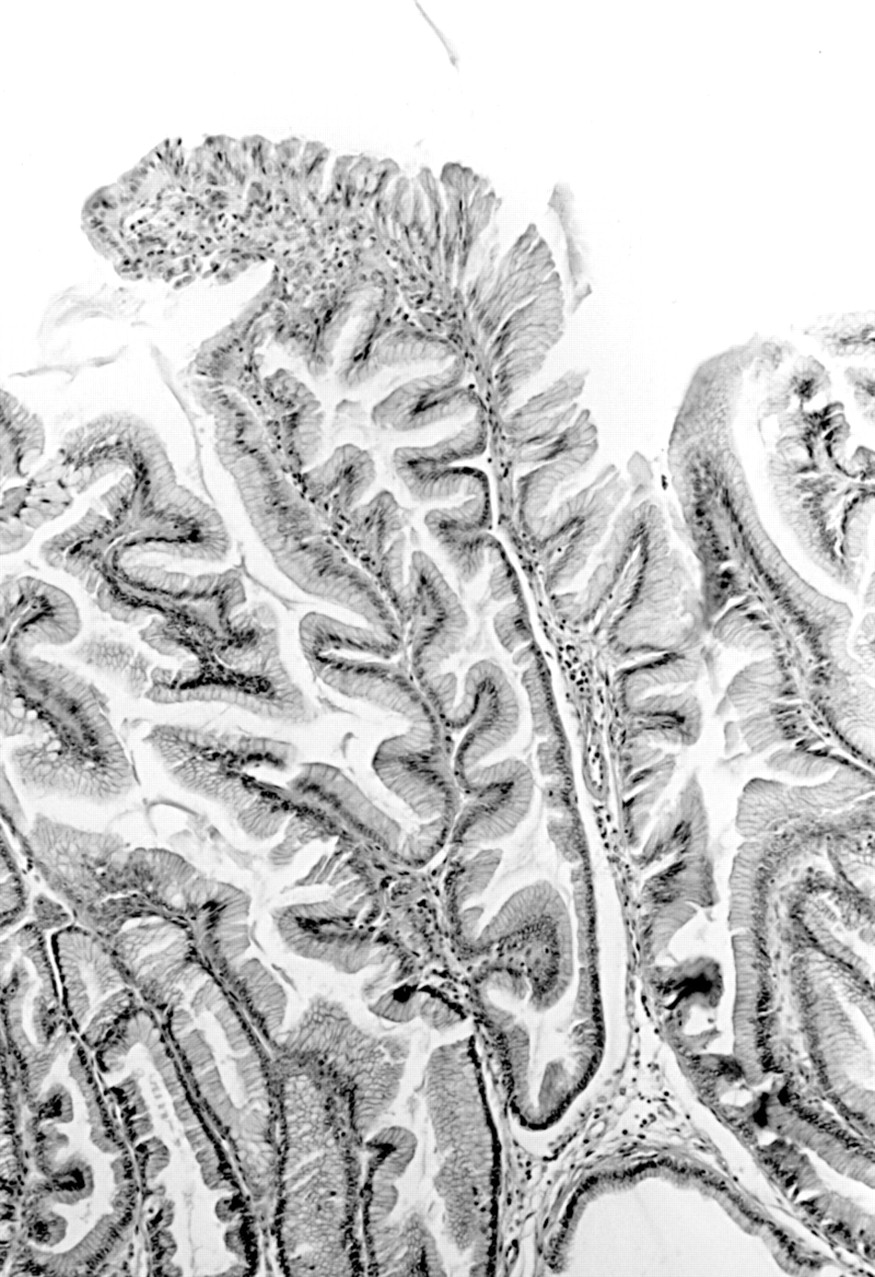
The histological examination revealed a protruding neoplastic lesion composed of elongated fronds with lateral crenate, saw tooth-like notches caused by scalloped epithelial indentations (fig 2). The nuclei covering the serrated glands were stratified, either cigar shaped with irregular chromatin deposits, or vesicular shaped carrying a large nucleolus (fig 3A). In other cells, the nucleoli were dark and irregular as a result of nucleolus associated chromatin. Connecting thin chromatin bridges were seen between two or more individual chromocentres and between the irregular chromatin clumps along the nuclear membrane and the chromocentres. Mitotic figures were increased. Some glands showed a back to back arrangement, others a gland within glands arrangement, and in one area invasive carcinoma was seen in the luminal aspect of the neoplasm (fig 3B). Other areas showed elongated fronds without indentations. The pedunculated base of the serrated neoplasm showed no invasive growth.

Low power view of the protruding neoplasm showing elongated fronds with lateral crenate, saw tooth-like notches resulting from scalloped epithelial indentations (haematoxylin and eosin; original magnification, ×5).

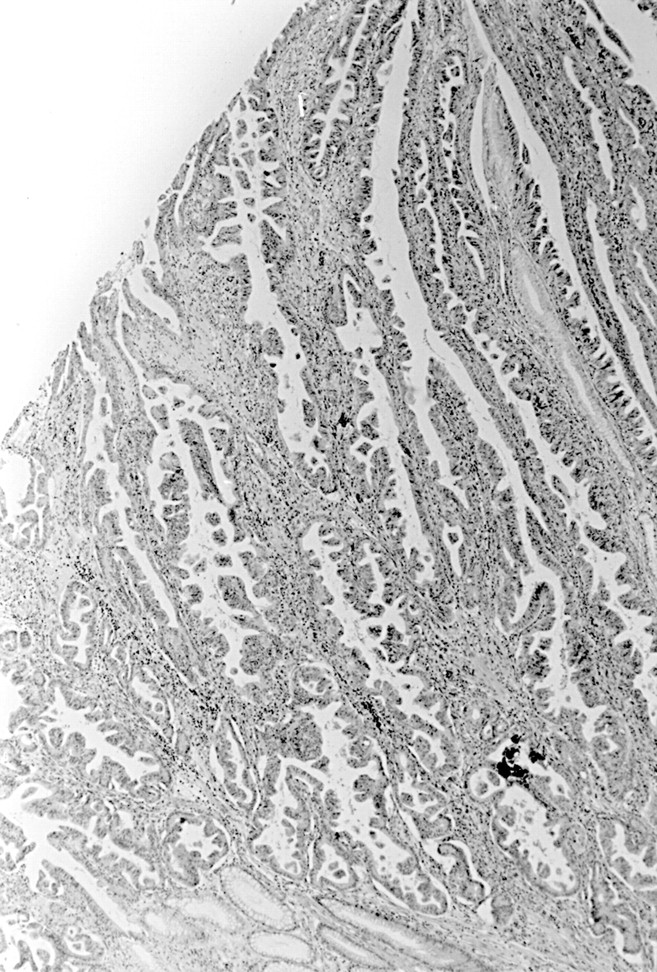
(A) Area demonstrating architectural variations in the serrated neoplasm (haematoxylin and eosin; original magnification, ×10). (B) Area with invasive carcinoma found in the luminal aspect of the neoplastic lesion (MIB1 antibody; original magnification, ×5).
Immunohistochemical staining revealed pronounced Ki63 (MIB1) expression in the serrated protruding adenoma, in addition to the area of invasion. p53 was not expressed. It should be noted that the preparation had been fixed in formalin for two days. The possibility that the relatively long period of fixation led to spurious p53 results cannot be rejected.
The pedicle of the serrated neoplasia “emerged” from a non-protruding serrated adenoma measuring 2 cm in diameter. The non-protruding lesion showed serrated foveoli with indentations (fig 4) lined by dysplastic cells (fig 5), which exhibited pronounced Ki63 (MIB1) expression (fig 6). The non-protruding serrated adenoma was partly surrounded by gastric mucosa with hyperplastic foveolar epithelium showing serrated indentations. No dysplasia could be demonstrated (fig 7). The hyperplastic foveolar epithelium mimicked hyperplastic colorectal polyps.20
Gastric mucosa (of corpus type) surrounding the protruding neoplasm with hyperplastic, tall foveoli with serrated indentations (haematoxylin and eosin; original magnification, ×10).

Gastric mucosa surrounding the protruding neoplastic lesion showing hyperplastic, tall foveoli with serrated indentations lined with dysplastic cells (haematoxylin and eosin; original magnification, ×10).

Immunohistochemical study showing pronounced cell proliferation in the serrated indented epithelium of the neck of non-dysplastic glands (MIB1 antibody; original magnification, ×10).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
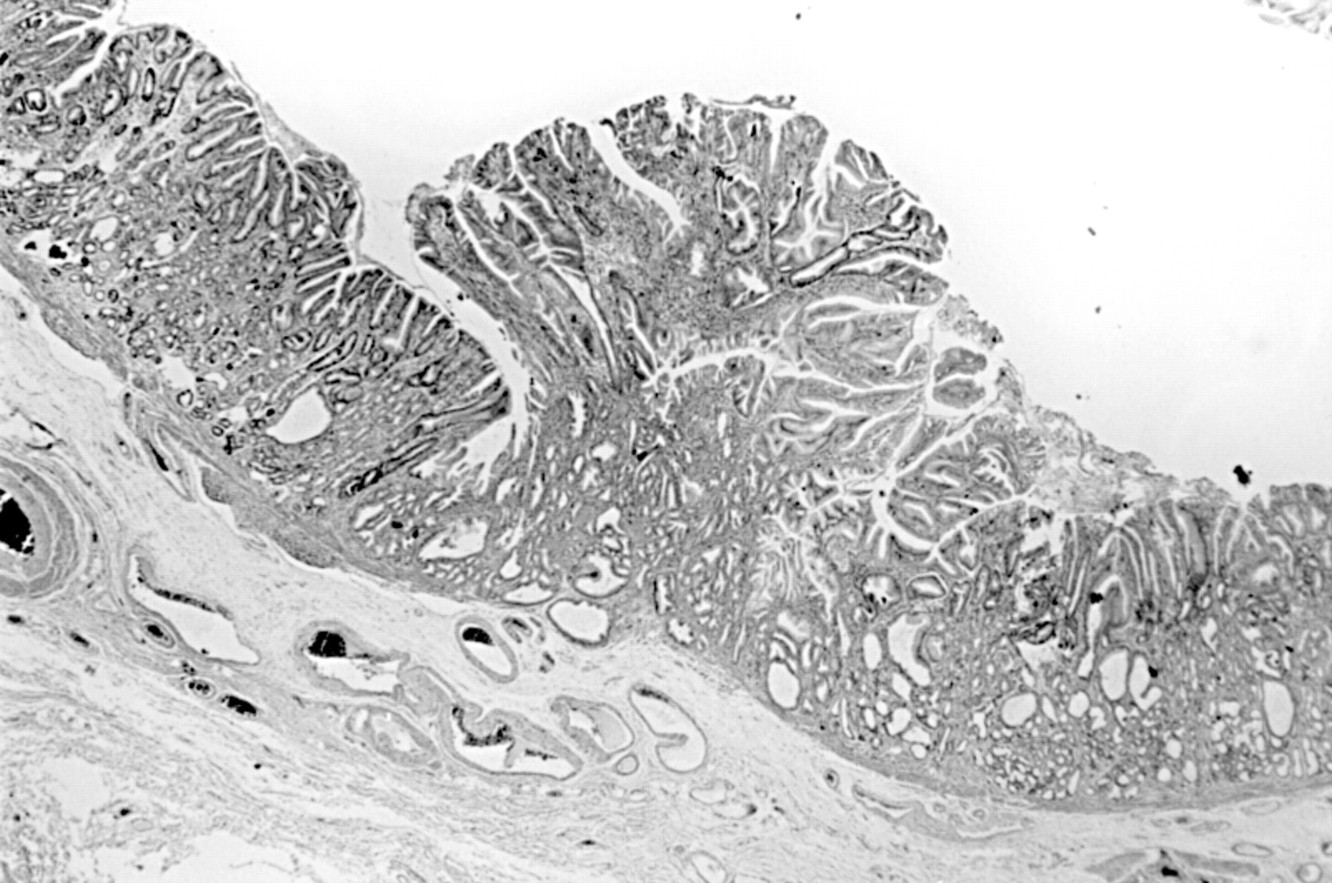
Abrupt border between the normal gastric mucosa and the non-protruding mixed polyp (composed of hyperplastic, tall foveolar mucosa with serrated indentations), which surrounded the protruding neoplasm (haematoxylin and eosin; original magnification, ×5).
The fundic mucosa surrounding the hyperplastic foveolar epithelium showed occasional intestinal metaplastic cells and dilated gastric glands. The foveoli were normal. No inflammation, atrophy, or dysplastic changes were found.
Discussion
On the grounds of gross appearance, Goldstein and Lewin21 classified gastric adenomas into flat topped, villiform, and pedunculated, and Ming and Goldman18 classified them into flat and papillary. In a recent study,22 we found that 40 of 67 gastric adenomas were non-protruding (not thicker than twice the thickness of the normal gastric mucosa), with the remaining 27 being protruding (having more than twice the thickness of the normal gastric mucosa).
Based on their histological appearance, Elster23 classified gastric polyps into focal foveolar hyperplasia, hyperplasiogenic polyps, and tubular and villous adenomas, and Appelman4 classified them into non-neoplastic (focal foveolar hyperplasia and hyperplastic polyps), non-neoplastic possibly hamartomatous (Peutz-Jehgers-type polyps), and neoplastic adenomas (with or without invasive carcinoma). Nakamura11 grouped gastric polyps into types I and II (hyperplastic polyps), and types III and IV (adenomas), and Kozuka24 grouped them into common type (hyperplastic, adenomatous, and carcinomatous polyps), special-type hamartoma (Peutz-Jehgers polyps, juvenile polyps, polyps in Cronkhite-Canada syndrome, and fundic gland cyst polyps), polypoid lesions (inflammatory polyps and polypoid carcinoma), and polyps resulting from a submucosal mass. A special histological phenotype of gastric tubular adenomas built of dysplastic Paneth cells has been also described.25
Surprisingly, serrated adenomas have not been found in the aforementioned classifications of gastric adenomas.26 One possibility is that gastric serrated adenomas have been classified together with gastric villous adenomas. Another possibility is that this type of lesion is very rare in the stomach. In this respect, it should be mentioned that we found no case of serrated adenoma among 224 gastric adenomas (154 in Japanese and Icelandic patients,22,27 and 70 in Swedish patients; CA Rubio, 2001, unpublished).
Gastric adenomas resides often evolve into invasive carcinomas.4–12,15–24,27 Invasive carcinomas in adenomas have been reported in 6–21% of non-protruding (flat) adenomas and in 20–76% of protruding (papillary) adenomas.26 The frequency of carcinoma correlates with the size of the adenoma and with the severity of the dysplasia.26
The protruding serrated adenoma presented here showed elongated fronds with lateral crenated, saw tooth-like notches resulting from scalloped epithelial indentations. The cells lining the epithelium covering those notched fronds were pleomorphic.
Areas with cigar shaped dysplastic nuclei reaching the superficial aspect of the epithelium were regarded as high grade dysplasia, whereas areas with vesicular shaped nuclei carrying a large nucleolus reaching the upper border of the epithelium were regarded as carcinoma in situ (intraepithelial carcinoma). There were glandular structural changes such as “back to back” glands and “gland within glands” arrangements, consistent with suspicious intramucosal carcinoma. Moreover, unequivocal adenocarcinoma invading the submucosal tissue was present at the tip of the neoplastic lesion; no carcinoma was present at the base of the protruding serrated neoplasm.
The protruding serrated neoplasia “emerged” from a non-protruding serrated adenoma. Cellular proliferation (Ki67) was intense in the dysplastic cells covering serrated indentations in the neck and superficial foveolar epithelium (fig 5). The underlying fundic glands were Ki67 negative.
The protruding serrated neoplasm mimics serrated adenomas of the colon, which are by far more common.28,29 In serrated adenomas of the colon, dysplastic cells are initially found at the base of the crypts, which is also the site of increased cellular proliferation.29 Colorectal carcinomas have also been found to originate in non-protruding serrated adenomas.29
This gastric serrated adenoma differs from the most commonly occurring histological phenotypes of gastric adenomas (tubular, tubulovillous, or villous) reported in the literature.4,19 The differential diagnosis with other lesions in the gastric mucosa includes hyperplastic polyps,30 Menetriér's disease,31 and hyperplastic lymphocytic gastritis.32 With regard to Menetriér's disease, in 1997 Stamm33 reported 11 cases of localised hyperplastic gastropathy of the mucous cell and mixed cell type, which was consistent with localised Ménétrier's disease. The foveoli had a corkscrew profile, of the type described in Menetrier's disease.31 Serrated structures were neither described nor shown in the illustrations.33
The protruding serrated neoplastic lesion presented here “emerged” from a non-protruding serrated adenomatous lesion, which had at its periphery abutting areas of hyperplastic foveolar epithelium (with serrated indentations) without dysplasia. A similar histological constellation in the colon has been named mixed hyperplastic polyp serrated adenoma by Longacre and Fenoglio-Preiser.28 Recently, Jass et al reported the occurrence of neoplastic changes in hyperplastic colorectal polyps.34 Colorectal hyperplasic polyps are characterised by foveolar hyperplasia with serrated indentations without dysplasia.20 In the light of these observations, it appears that not only colonic hyperplastic polyps but also gastric serrated hyperplastic polyps may evolve into a neoplastic lesion. Interestingly, Zea-Iriarte et al reported rare cases of invasive carcinoma in gastric hyperplastic polyps.30 Gastric hyperplastic polyps differ from hyperplastic colonic polyps because they are devoid of serrated indentations.30
Despite its decreasing incidence, gastric carcinoma continues to be one of the most common cancers world wide.26 Histological mucosal changes, such as atrophic gastritis and intestinal metaplasia, are believed to predispose to gastric cancer development, and dysplasias of flat mucosa, adenomas, and ectopic gastric glands11,13,35–37 appear to be genuine precursors of gastric carcinomas of the intestinal type. However, dysplasia in flat mucosa, adenomas, and ectopic gastric glands are rather uncommon lesions. Therefore, any possible alternative pathway to investigate gastric carcinogenesis should deserve careful attention.
Increased awareness of the existence of serrated neoplasia in the stomach may result in similar cases being reported in the future.
This is the first case of serrated neoplasia of the stomach reported in the literature.
Acknowledgments
This study was supported by the Cancer Society, Stockholm, and the Karolinska Institute.