Article Text

CSF spectrophotometry in the diagnosis of subarachnoid haemorrhage
Abstract
After subarachnoid haemorrhage (SAH), cerebral angiography is usually performed to establish a site of bleeding, which may then be treated surgically to prevent a potentially catastrophic re-bleed. The investigation of choice in the diagnosis of SAH is computerised tomography (CT). However, because CT can miss some patients with SAH, cerebrospinal fluid (CSF) spectrophotometry should be performed in those patients with negative or equivocal CT scans or those who have presented several days after the suspected bleed. Spectrophotometry should aim to detect the presence of both oxyhaemoglobin and bilirubin because either one or both of these pigments may contribute to xanthochromia following SAH. CSF supernatant is scanned using a double beam spectrophotometer at wavelengths between 350 nm and 650 nm. Oxyhaemoglobin alone produces an absorption peak at 413–415 nm, bilirubin alone produces a broad peak at 450–460 nm, and bilirubin together with oxyhaemoglobin produce a shoulder at 450–460 nm on the downslope of the oxyhaemoglobin peak. To minimise the frequency of false positive and false negative results, a protocol has been developed, which is described.
- subarachnoid haemorrhage
- computerised tomography
- cerebrospinal fluid
- spectrophotometry
- oxyhaemoglobin
- bilirubin
- xanthochromia
Statistics from Altmetric.com
CSF spectrophotometry in the diagnosis of subarachnoid haemorrhage
- subarachnoid haemorrhage
- computerised tomography
- cerebrospinal fluid
- spectrophotometry
- oxyhaemoglobin
- bilirubin
- xanthochromia
Subarachnoid haemorrhage (SAH) describes spontaneous arterial bleeding into the subarachnoid space, usually from a cerebral aneurysm. The most common presenting feature is severe occipital headache of sudden onset. This may be followed by vomiting and loss of consciousness. Up to half of affected patients have a further episode of bleeding. A population based study of SAH in New Zealand reported incidence rates of 10.5 and 18.3/100 000 for men and women, respectively. Sixty eight per cent of all cases had a confirmed intracranial aneurysm or arteriovenous malformation.1
After SAH, cerebral angiography should be performed in patients who are fit for surgery, to establish the site of bleeding, although about 5% of patients with a characteristic pattern of anuerysmal bleeding on computed tomography (CT) have no aneurysm demonstrated at angiography.2 When an aneurysm is identified, it may be treated surgically to prevent a potentially catastrophic re-bleed. Cerebral angiography is available only in neurosurgical centres and is an invasive procedure, with the risk of permanent neurological complications reported as ranging from 0.06% to 0.5%.3–5
Diagnosis of SAH
The investigation of choice in the diagnosis of SAH is CT, which usually demonstrates the presence of blood in the basal cisterns. CT may also provide valuable information about the origin and extent of haemorrhage and about the presence of early complications.2 However, CT can miss some patients with SAH. In 1983, a prospective study of CT in 1378 patients reported a diagnostic sensitivity for SAH of 95%.6 More recently, two studies using modern CT equipment reported false negative rates of 2% (CT performed within 12 hours of onset of headache)7 and 7% (CT performed within 24 hours of onset of headache).8 Timing of the CT is crucial because sensitivity declines with time, as shown in a series of 2940 patients with SAH. The diagnostic sensitivity of CT scanning decreased from 92.1% on the day of the bleed to 57.6% on day 5.9 Sensitivity may also be lower if scans are reported by inexperienced or non-specialist staff. Because CT scanning alone cannot reliably exclude SAH, it is recommended that patients with severe sudden headache but normal CT should have a lumbar puncture performed to rule out SAH.2,1011 This recommendation was endorsed in guidance issued by the Society of British Neurological Surgeons in 1997. Lumbar puncture is contraindicated in patients with papillo-oedema, focal neurological deficit, or reduced consciousness.
Pigments in CSF
After haemorrhage into the cerebrospinal fluid (CSF), lysis of red blood cells occurs within two to four hours, although the average survival of red blood cells in peripheral blood is 120 days. Haemolysis of the subarachnoid erythrocytes releases oxyhaemoglobin, which may be detected between two and 12 hours after a bleed. The liberated oxyhaemoglobin is gradually converted into bilirubin by macrophages and other cells of the leptomeninges.12–15 This conversion is reported to occur for about a week after the onset of aneurysmal bleeding.13 Spontaneous oxidation of the haem group may occur after about 10 days, resulting in approximately equal proportions of methaemoglobin and oxyhaemoglobin.15 This last process is often associated with the presence of intracranial haematoma.14,16 The presence of oxyhaemoglobin, bilirubin, or methaemoglobin gives rise to a yellowish or reddish-brown discolouration of CSF supernatant known as xanthochromia. It should be noted that xanthochromia is not specific to intracranial bleeding and can be seen in patients with jaundice and those with high CSF protein concentrations.14
Principles of CSF spectrophotometry
CSF spectrophotometry is indicated only in those patients with suspected SAH who have negative or equivocal CT scans.2,10,11 Occasionally, it may be useful in patients presenting a week or more after the onset of symptoms in whom CT has not been performed. Lumbar puncture should not be performed until 12 hours after the onset of symptoms because earlier sampling may produce false negative results.12 Although some workers have advocated visual inspection alone,17 spectrophotometry is less subjective and reportedly more sensitive,16 and is therefore the recommended technique.2,10 A study of 111 patients with blood in the basal cisterns on CT reported the sensitivity of spectrophotometry as 100%, decreasing to 90% by three weeks post bleed.18 However, the sensitivity of spectrophotometry in patients with negative CT remains unknown. Spectrophotometry should aim to detect the presence of both oxyhaemoglobin and bilirubin because either one or both of these pigments may contribute to xanthochromia after SAH.13,16 In practice, it is rare to detect bilirubin alone because oxyhaemoglobin is usually detected for at least three weeks after SAH,18 and it is unusual for patients to present later than this.
CSF supernatant should be scanned using a double beam spectrophotometer at wavelengths between 350 nm and 650 nm to detect oxyhaemoglobin alone (absorption peak 413–415 nm) (fig 1); oxyhaemoglobin and bilirubin (a bilirubin shoulder at 450–460 nm on the downslope of the oxyhaemoglobin curve) (fig 2A, B); or, more rarely, bilirubin alone (a broad peak at 450–460 nm) (fig 2C). It is the presence of a peak that should be sought rather than absolute absorbance at a specific wavelength. For example, a raised CSF protein concentration may cause a raised absorbance at 413 nm without the presence of an oxyhaemoglobin peak (fig 3).19

Spectrophotometric scan of oxyhaemoglobin alone; wavelength of absorption peak, 414 nm.
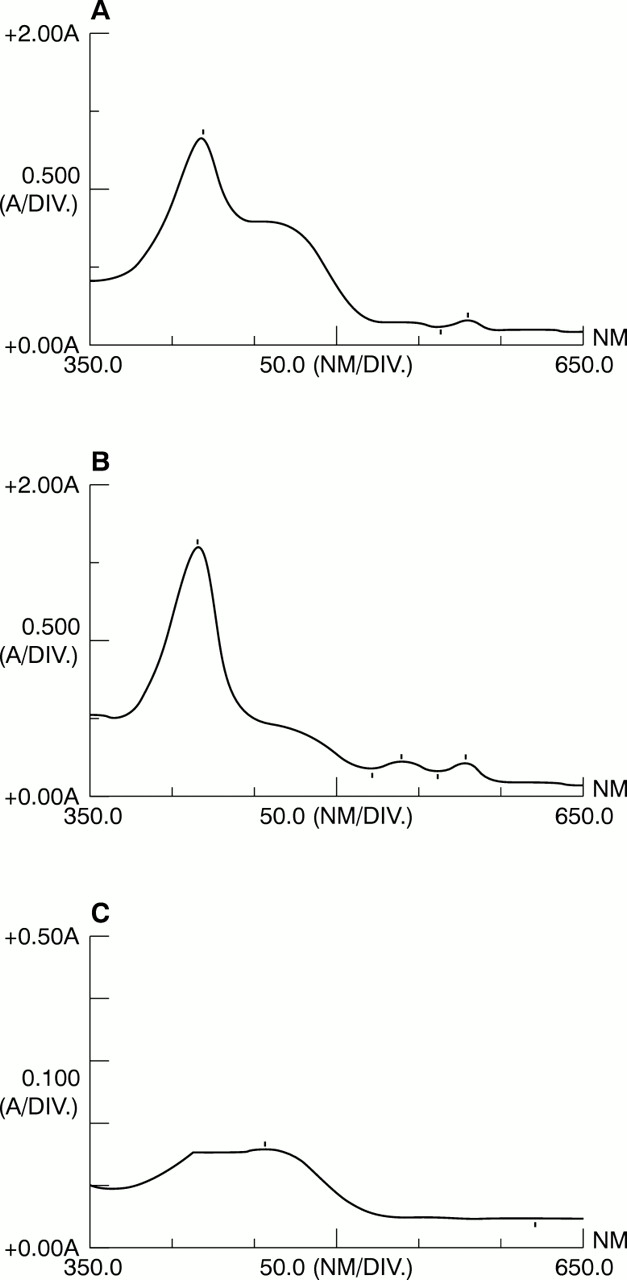
Spectrophotometric scans of oxyhaemoglobin peak with bilirubin shoulder on downslope at wavelength of 450–460 nm (A and B) and bilirubin alone (C), exhibiting a broad peak with maximum absorbance at wavelength of 453 nm.

Spectrophotometric scans where neither oxyhaemoglobin nor bilirubin is detected. (A) Clear cerebrospinal fluid (CSF) with normal protein concentration; (B) turbid CSF with raised protein concentration (2.53 g/litre).
Detection of bilirubin alone
If bilirubin alone is detected, quantitation is required with a correction to allow for non-haemorrhagic sources, such as influx of protein bound bilirubin across the blood–brain barrier (see below).20
Measured CSF bilirubin concentration (μmol/litre) = (A453 − A578) × 23, where 578 nm is the wavelength at which oxyhaemoglobin has identical absorbance to its absorbance at 453 nm, and 23 is the extinction coefficient for bilirubin (μmol/litre) at a wavelength of 453 nm.
Non-haemorrhagic component of bilirubin (μmol/litre) = serum bilirubin concentration (μmol/litre) multiplied by the ratio of CSF total protein concentration to serum total protein concentration.
Haemorrhagic CSF bilirubin concentration (μmol/litre) = measured CSF bilirubin (μmol/litre) − non-haemorrhagic CSF bilirubin (μmol/litre).
False positive results
Oxyhaemoglobin alone can be detected on spectrophotometry in the absence of SAH as a result of traumatic lumbar puncture and in vitro haemolysis. False positive results were reported in six of 27 patients without SAH undergoing spinal anaesthesia, where CSF samples demonstrated red blood cell counts of up to 705/mm.3,21 However we conducted a similar study and found no false positive results in 22 patients without SAH when CSF was centrifuged within 40 minutes. Red blood cell counts ranged from < 5 to 2215/mm.3,22 Traumatic taps are common because many lumbar punctures are performed by inexperienced junior staff. If a good flow of CSF is achieved, then serial samples are advisable in the hope that later samples will have less red blood cell contamination. The likelihood of false positive results is related to the degree of bloody contamination at lumbar puncture and to the delay between lumbar puncture and centrifugation of CSF. An in vitro study of CSF red blood cell contamination has suggested that CSF samples with cell counts of < 40 000/mm3 that are centrifuged within 15 minutes are unlikely to produce false positive results.22 CSF samples should be transported to the laboratory as quickly as possible. If sample volume permits, a small aliquot should be taken in case a red blood cell count is deemed helpful retrospectively, and the sample then centrifuged immediately. If a false positive result is suspected, a second lumbar puncture (preferably performed one vertebral interspace above the original puncture) may produce a negative result and obviate the need for cerebral angiography. However, the procedure of lumbar puncture may itself produce haemorrhage into the subarachnoid space, which will cause subsequent lumbar puncture samples to be positive.
Although the presence of both haemoglobin and bilirubin is usually diagnostic of SAH, severe bloody contamination may cause confusion. We have found that CSF spiked with blood to produce red blood cell counts of approximately 402 000/mm3 demonstrated an oxyhaemoglobin peak with a bilirubin shoulder on spectrophotometry (fig 4).23

Spectrophotometric scan of (A) plasma separated 15 minutes after collection of whole blood and (B) cerebrospinal fluid centrifuged 15 minutes after addition of whole blood to produce a red cell count of approximately 400 000/mm3.
False negative results
As discussed above, these can occur if lumbar puncture is performed earlier than 12 hours after SAH.12
Although the study described above of 111 patients with confirmed SAH reported no false negative results in samples taken from 12 hours to two weeks post bleed,18 these patients had classic CT appearances of SAH and so are not representative of those patients (that is, CT negative) who would normally have spectrophotometry performed. The false negative rate of CSF spectrophotometry in the diagnosis of SAH in CT negative patients is not known.
Protocol
See flow diagram (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram of the procedure to diagnose subarachnoid haemorrhage (SAH) using spectrophotometry of cerebrospinal fluid (CSF). CT, computed tomography; OxyHb, oxyhaemoglobin; RBC, red blood cells.
Acknowledgments
I wish to thank Mrs L Smith for her helpful comments during the production of this paper.