Article Text

Abstract
Aims—Angiogenesis, an important prognostic factor in several tumours, is a complex event mediated by angiogenic factors released from cancer cells and host immune cells. Among the host immune cells, a role has been implicated for mast cells in tumour progression via promoting angiogenesis. Data have been recorded that indicate a correlation between intratumoral neovascularisation, as assessed by microvessel density (MVD), and prognosis in squamous cell carcinoma (SCC) of the oesophagus. However, a correlation between mast cell density (MCD) and either prognosis or angiogenesis has not been delineated yet in this disease. The aim of this study was to investigate the prognostic value of MVD and MCD in SCC of the oesophagus. The correlation between MVD and MCD was also evaluated.
Methods—MVD and MCD were investigated in tumour specimens from 53 patients diagnosed with SCC of the oesophagus. Intratumoral microvessels were stained with anti-CD34 antibody and mast cells with toluidine blue before being measured by light microscopy.
Results—Both MVD and MCD were associated with the depth of wall invasion, lymph node metastasis, and tumour progression (stage). A significant correlation was noted between MVD and MCD values (r = 0.72). The prognosis was significantly worse in patients with high MVD (≥ 92) and high MCD (≥ 18) values. Multivariate analysis indicated that MVD and stage were independent predictors of survival.
Conclusions—These findings support the suggestion that MVD is a reliable prognostic marker in SCC of the oesophagus. Moreover, MCD may have a role in the angiogenesis of these tumours and might be responsible for their aggressive behaviour.
- microvessel density
- mast cell
- prognosis
- oesophagus
- squamous cell carcinoma
- angiogenesis
Statistics from Altmetric.com
Angiogenesis plays an important role in tumour growth and the formation of metastases.1,2 Numerous quantitative studies have shown that intratumoral neovascularisation is a significant predictor of metastasis and clinical outcome in many tumours, including gastrointestinal carcinomas.3–5 In squamous cell carcinoma (SCC) of the oesophagus, some studies have investigated the association between microvessel density (MVD) and clinicopathological parameters and prognosis.6–13 Data indicating a correlation between MVD and tumour behaviour and survival have been reported.8–13
Recently, apart from their roles in the maintenance of homeostasis and in inflammation, the association of mast cells with various tumours has been described.14–17 In several malignancies, mast cell density (MCD) has been found to correlate with increased risk of metastasis and prognosis.14,15 Currently, the exact functional relevance of mast cells surrounding various tumours is unclear. However, accumulated evidence indicates that mast cells might induce tumour progression by providing mitogenic stimulation or angiogenesis. In addition, data from experimental studies support the induction of neovascularisation by mast cell derived angiogenic mediators or growth factors.18–23 Although a correlation between MCD and prognosis has been described in the gastrointestinal system,15 in SCC of the oesophagus the correlation between MCD and either clinical progression and clinicopathological parameters or angiogenesis has not been investigated.
Therefore, our study was undertaken to investigate the prognostic value of MCD and MVD in the context of clinicopathological parameters and survival in SCC of the oesophagus. The correlation of MCD and MVD was also evaluated.
Methods
Fifty three patients treated and followed in the department of thorax surgery at Akdeniz University between 1992 and 1999 who were diagnosed as having SCC of the oesophagus at the pathology department were enrolled in our study. The mean ages of the 30 male and 23 female patients at the time of the surgery were 45 years (range, 29–62) and 42 years (range, 32–55), respectively. Table 1 summarises the other clinicopathologic characteristics of the cases (published as supplemental data in JCP online: www.jclinpath.com).
Neither chemotherapy nor radiotherapy was applied before surgery. Survival data were available on all patients. The mean follow up time for all patients was 24 months (range, 6–60). Haematogenous metastases were detected in 20 patients (11 liver and nine lung).
Haematoxylin and eosin stained tissue sections (4 μm thick) from the surgical specimens fixed in 10% formalin and embedded in paraffin wax were reviewed and representative tissue blocks (two to five blocks from each case) were selected. For microvessel staining, sections from each tumour were dewaxed and heated in a microwave oven for 10 minutes to retrieve antigens. Endogenous peroxidase was blocked by using 3% hydrogen peroxide in methanol for 10 minutes. Each step of incubation was followed by thorough washing of the slides in distilled water and phosphate buffered saline (PBS). After incubation with primary antibody against CD34 (QBEnd 10, mouse monoclonal; 1/50 dilution; Dako, Glostrup, Denmark) for 30 minutes, sections were reacted with secondary biotinylated antibody for 15 minutes and streptavidin for 15 minutes. Finally, all slides were treated with DAB reagent to develop colour and counterstained with Mayer's haematoxylin.
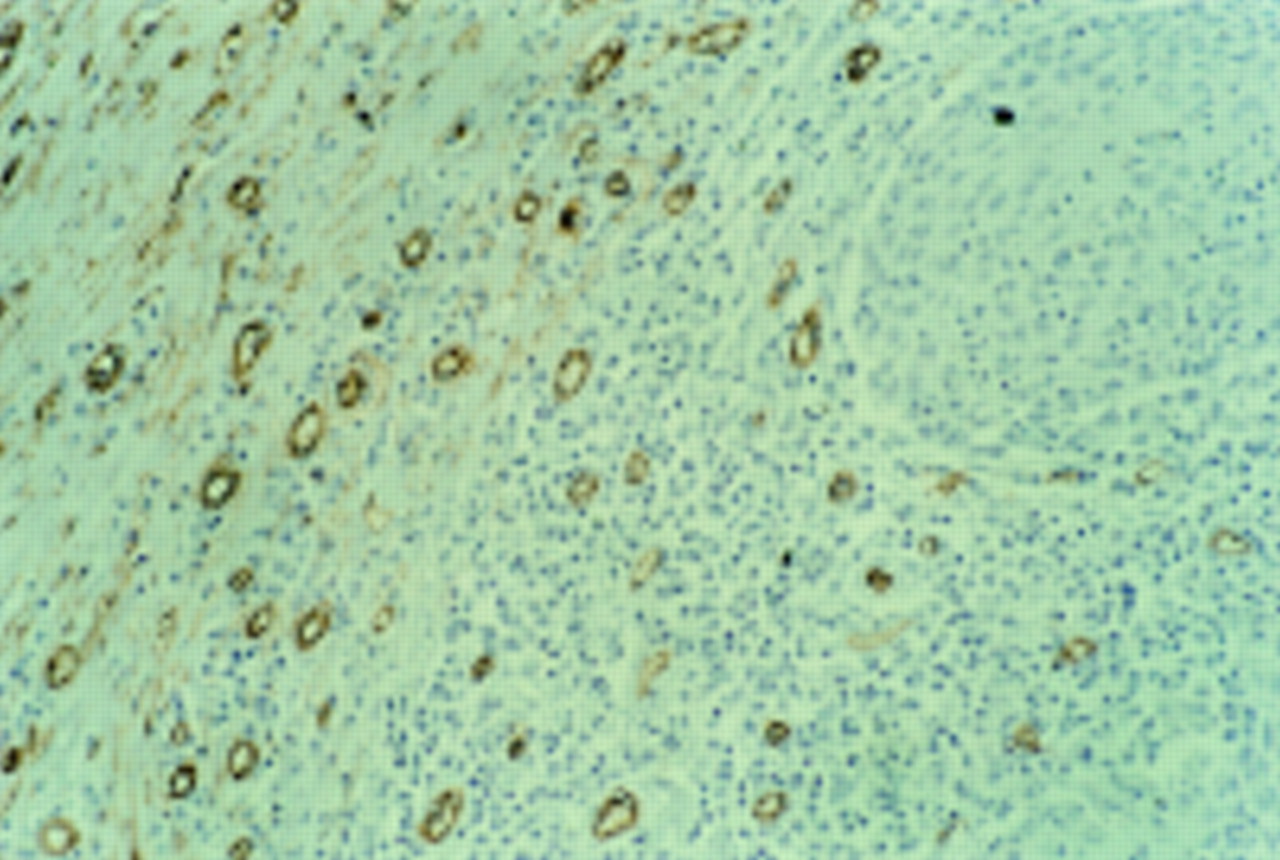
For determination of MVD, the stained sections were screened at low power (×100) to identify the areas of highest vascularisation within the tumour (hot spots). Microvessel counts were performed at ×400 magnification (fig 1) with the use of an ocular grid subdivided into 100 areas in four fields of vision, and for each case the hot spot MVD was noted.24 In addition, microvessels were counted throughout each of the tissue sections in 10 systematically selected fields of vision, to obtain systematic MVD values.24
Immunohistochemical staining of endothelial cells with antibody against CD34. Microvessels are represented by darkly stained capillaries and small clusters, which stand out sharply from other tissues (counterstained with Mayer's haematoxylin; original magnification, ×400).
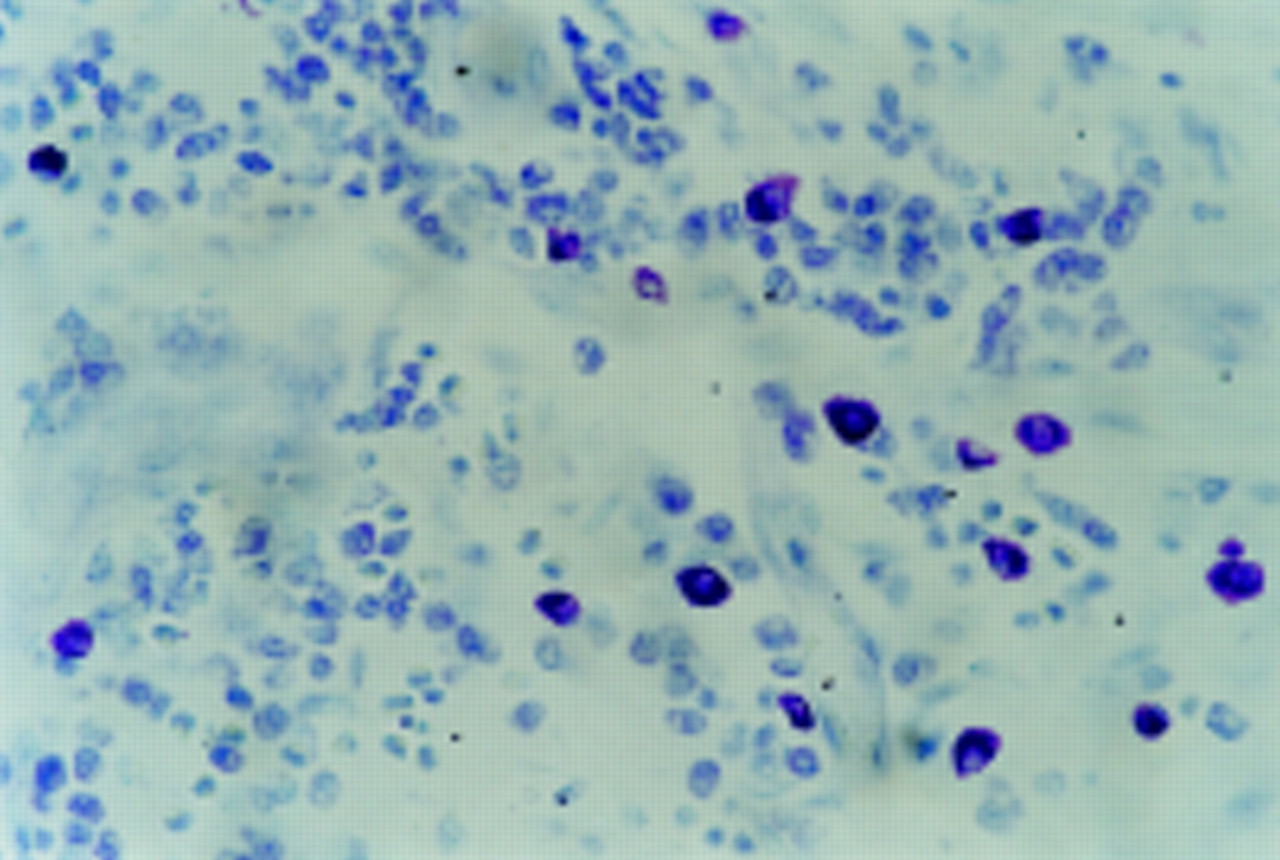
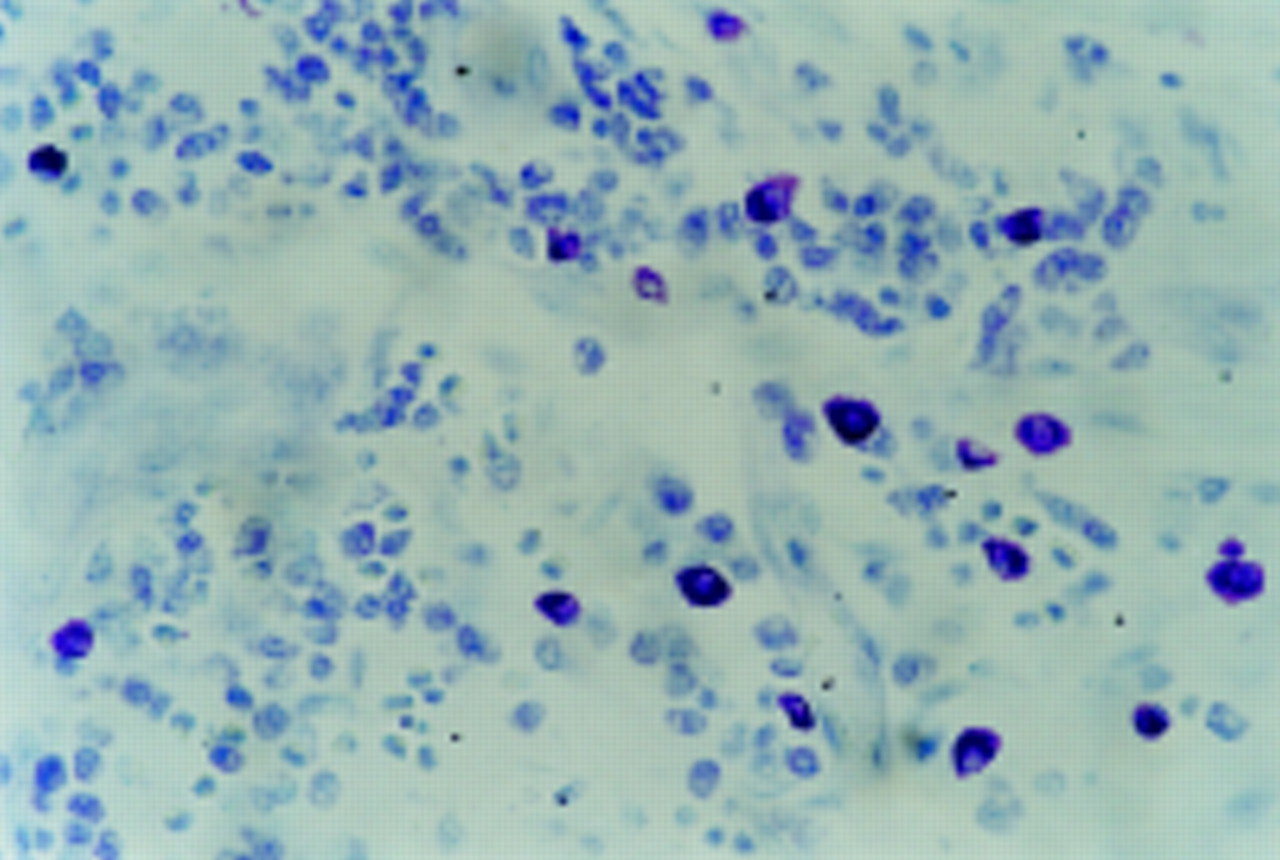
In each of the 53 cases, additional sections from the tissue blocks that were used to evaluate MVD were stained with 0.1% aqueous toluidine blue and tissue mast cells were identified by their characteristic metachromasia (fig 2). By using the same counting methods as for MVD evaluation, mast cells were counted in hot spots and also in each tissue section to determinate hot spot and systematic MCD values.

Mast cells in tumour stroma stained with toluidine blue. They are readily identified by their metachromatic granules and larger sizes (original magnification, ×200).
For statistical analysis, samples were divided into four groups according to the median values of the hot spot and systematic MVD and MCD results. Each of the hot spot and systematic MVD and MCD values was compared with clinicopathological parameters and checked by the Mann-Whitney U and χ2 tests. The correlation between MVD and MCD was tested by means of the Spearman's rank correlation coefficient. The Wilcoxon signed rank test was used to compare the ratios between microvessels and mast cells in hot spots and the systematic counts.
Survival was calculated from the day resection was performed to the day of death or the day of last follow up. Univariate and multivariate survival analyses were performed by means of the Kaplan-Meier method and Cox regression analysis, respectively. Confidence intervals were 95%. Significance was set at ≤ 0.05.
Results
Hypervascular areas were located, particularly on the invasive edges of the tumours. In each case, hot spot MVD and MCD values were significantly higher than systematic MVD and MCD values. The mean (SD) hot spot MVD among the samples was 115.01 (55.82), with a median of 92 and a range from 43 to 251. The systematic MVD varied from 13 to 98, with a mean (SD) of 48.05 (21.60). The mean (SD) hot spot and systematic MCD values were 21.29 (10.18), with a median of 18 and a range of 3 to 49, and 3.98 (2.230), with a median of 4 and range of 0.56 to 11, respectively.
There were significant correlations between hot spot and systematic MVD values (Spearman's rank correlation: r = 0.70; p < 0.01) and between hot spot and systematic MCD values (Spearman's r = 80; p < 0.01).
The ratios of the hot spot to systematic MCD and MVD values were 5.71 and 2.44, respectively (Wilcoxon rank test: p < 0.001). The ratio of the hot spot MCD to MVD values was significantly higher (1.8) than the ratio of systematic MCD to MVD values (0.08) (Wilcoxon rank test: p < 0.001). Moreover, Spearman's correlation test revealed a significant correlation between hot spot MVD and MCD (r = 0.72; p < 0.01).
No correlation was found between the systematic MVD and MCD values and the clinicopathological factors. However, hot spot MVD and MCD values were significantly higher in tumours with deeper penetration and lymph node metastases (p < 0.05). Higher hot spot MVD and MCD values were associated with tumour progression (stage III and IV v stage I and II; p < 0.01; tables 1 and 2; published as supplemental data in JCP online: www.jclinpath.com). Hot spot MVD values also correlated with lymphatic vessel invasion (p < 0.05; table 1; published as supplemental data in JCP online: www.jclinpath.com).
At the end of the follow up, 27 patients survived, with a mean survival period of 27 months. Twenty six patients died with a mean survival period of 18 months. The mean (SD) hot spot vessel counts were 90.82 (4.34) for the 27 survivors and 140.13 (67.65) for the 26 patients who died after surgery (p < 0.05). The hot spot MCD values of the survivor group were significantly lower (mean, 17.13; SD, 7.85) than those of the non-survivors (mean, 25.62; SD, 12.55; p < 0.05). However, the systematic MVD and MCD values were similar in both groups (p > 0.05).
When samples were divided into hypervascular and hypovascular groups, according to the median values of the hot spot MVD, the two groups consisted of 30 and 23 cases, respectively. Within these groups, there were 27 and 26 cases with high and low hot spot MCD values, respectively. Deeper tumour penetration, lymph node metastasis, and advanced stage tumours were observed more frequently in hypervascular tumours and in tumours with high MCD (tables 1 and 2; published as supplemental data in JCP online: www.jclinpath.com). Samples were also divided according to the median values of systematic MVD and MCD but no associations were seen between systematic MVD and MCD values and clinicopathological parameters.
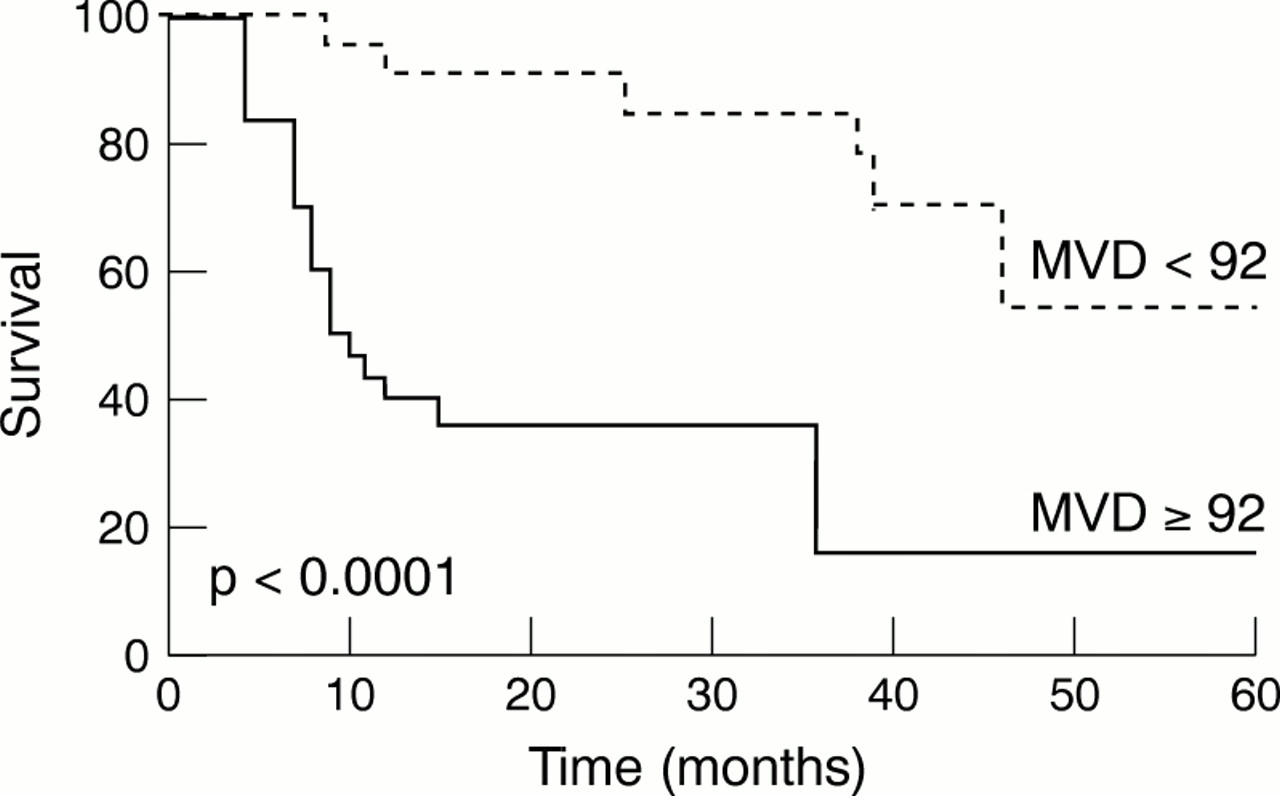
Kaplan Meier univariate survival analysis based on the log rank test revealed that survival correlated with tumour depth, stage, hot spot MVD, and hot spot MCD. Five year survival in the hypervascular and hypovascular groups, and groups with high and low hot spot MCD were 18%, 58%, 24%, and 52%, respectively (figs 3, 4).
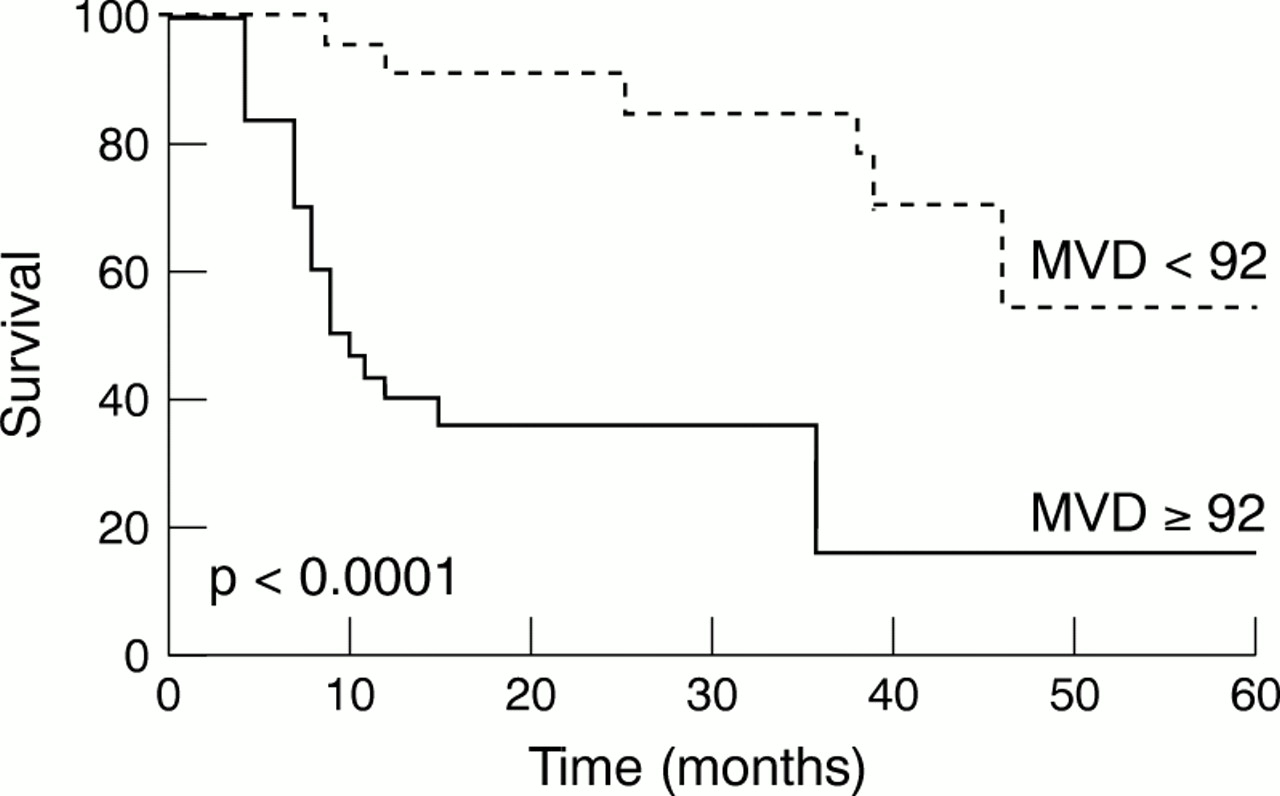
Survival curves according to microvessel density (MVD) status. Patients were stratified by the median microvessel count of the series.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves according to mast cell density (MCD) status. Patients were stratified by the median mast cell count of the series.
In multivariate analysis, MVD was found to be an independent prognostic factor (p = 0.009; risk ratio (RR) = 2.55), together with the stage of the disease (p = 0.041; RR = 2.16). However, in the same analysis, MCD did not reach significance (p = 0.865; RR = 2.16 ).
Discussion
Angiogenesis in SCC of the oesophagus has been investigated in several recent studies. In some reports vascular volume, vascular area, and vascular length were found not to correlate with the clinicopathological parameters of the disease.6,7 Previous studies that investigated angiogenesis in these tumours by means of the microvessel counting method demonstrated a relation between MVD and advanced disease parameters.8–13 Our present study revealed that higher MVD values were associated with the presence of lymph node metastasis, tumours with deeper penetration, and advanced stage. Similar to our findings, a linear relation between MVD and lymph node involvement, depth of wall invasion, and stage was seen in some studies.8,10,13 However, we did not detect an association of MVD with tumour size or an inverse correlation between MVD and advanced disease parameters, as described previously.9,11 Recently, it has been proposed that the use of different antibodies to define endothelium, different methodologies in the assessment of MVD, and interobserver variation could contribute to these discordant results.8 Although these factors pose potential limitations for comparison between studies, our results suggest that MVD is useful for detecting aggressive behaviour in tumour cells in SCC of the oesophagus.
In SCC of the oesophagus, an association of MVD with recurrence and survival has been demonstrated.8,10,13 Moreover, MVD was described as an independent prognostic factor in these tumours. In 41 patients with SCC of the oesophagus, Tanigawa et al found that MVD, assessed with either CD34 or von Willebrandt factor staining, was an independent prognostic variable.10 In our series, the prognosis of the patients with hypervascular tumours was found to be worse than those with hypovascular tumours, and multivariate analysis revealed that MVD was an independent prognostic factor (p < 0.05). Our findings are in agreement with those reported by Tanigawa et al,10 and support the view that in patients with SCC of the oesophagus, the assessment of tumour vascularisation is valuable for the prediction of tumour progression and clinical outcome.
Tumour angiogenesis is a complex event mediated by angiogenic factors released from cancer cells and/or host immune cells.25,26 Among these host immune cells, several observations have indicated a role for mast cells in tumour progression by promoting angiogenesis. Mast cells surround many tumours.18,27 In some malignancies, large numbers of mast cells were detected before the occurrence of neovascularisation.18,28 Basic fibroblast growth factor, interleukin 4 (IL-4), IL-8, tumour necrosis factor α (TNF-α), and TNF-β are among the mediators present in mast cell granules, and are strong inducers of angiogenesis.29–32 Mast cell deficient mice exhibit less tumour angiogenesis and tumour growth compared with mice with normal mast cell numbers.33 Moreover, mast cells were shown to induce neovascularisation through the carcinogenesis of squamous cells.34 Although mast cell mediated angiogenesis is a complex event that is not completely understood, these findings support the view that mast cells might induce tumour progression and potentiate metastasis by stimulating angiogenesis. In our study, the ratio of hot spot MCD to MVD values was higher than the ratio of systematic MCD to MVD values. Moreover, a significant linear correlation was detected between hot spot MVD and MCD values. This association indicates that, in SCC of the oesophagus, mast cells might have a role in tumour associated angiogenesis. In a recent study, Belien et al investigated the topographical relations between tumour angiogenesis and mitosis in breast carcinoma with the use of image processing, and demonstrated that microvessel and mitosis hot spots were close or overlapping, evidence of the association between vascularisation and tumour cell proliferation.35 In SCC of the oesophagus, further studies on the topographical distribution of microvessel and mast cell hot spots might help elucidate the possible role of mast cells in tumour angiogenesis.
The stromal mast cell reaction has been analysed in certain types of tumours to detect the correlation, if any, between mast cell density and disease outcome, but discordant results have been reported.14,36,37 In the gastrointestinal system, an increase in mast cell count correlated with a worse prognosis in patients with rectal carcinoma.15 Although in colon carcinoma no relation between mast cell density and survival was detected,17 more recently it was demonstrated that the mast cell count might be a useful marker of colorectal neoplasia.38 Finally, in our study, higher MCD values correlated with advanced disease parameters and worse prognosis in SCC of the oesophagus. However, in Cox regression analysis, MCD was not found to be an independent prognostic parameter. Although only a limited number of cases was included in our study, this is the first attempt to compare angiogenesis and mast cell density in SCC of the oesophagus. Therefore, our findings need to be investigated further with large scale studies.
It is difficult to explain the discordant results with MCD in different tumours. Reed and colleagues36 found a significant increase in the mast cell population surrounding melanocytic lesions expressing IL-3 (which is chemotactic to mast cells) compared with lesions that did not express IL-3. In addition, mast cells around these lesions were found to possess IL-3α receptors. They concluded that the simultaneous expression of several substances providing mast cell chemotaxis in tumour cells could influence the degree of mast cell response and could define the presence of different types of mast cell containing specific receptors against these chemoattractants. Although further studies are needed to establish the effect of chemotactic factors released from cancer cells on the stromal mast cell reaction, these findings suggest that differences in these factors depending on tumour type could partly explain dissimilar findings between mast cell density and tumour progression in different tumours.
In our study on the assessment of angiogenesis and mast cell density, the microvessels and mast cells were counted in each mm2 of tissue, without considering the proportion of stroma. It has been stated that the growth of a solid tumour is dependent upon an adequate blood supply, which is achieved by the generation of stroma, where the formation of new capillaries is a central event, and also that this component is an entry site for immune inflammatory cells.20,39–42 In other words, in a particular tumour, the number of microvessels and mast cells could be related to the amount of stromal component and consequently tumours having more stroma might have more microvessels and mast cells. For this reason, variations in the amount of stroma and tumour cells in different counting fields might influence the objectivity of the traditional microvessel counting procedure. If counting was performed for each mm2 of tissue, vascularity and mast cell density might not be accurate, because the proportion of tissue occupied by tumour cells might be much greater than that occupied by stroma. Therefore, we suggest that in SCC of the oesophagus, correcting the microvessel and mast cell counts for stromal fraction when assessing the relation between angiogenesis and mast cells would be superior and more objective than traditional counting methods. A similar method has been described previously for the correction of the percentage of the epithelial fraction when counting mitosis.37,43,44
In conclusion, the results of our study demonstrate that MVD could be a useful indicator of tumour progression and survival in SCC of the oesophagus. The significant association between MVD and MCD values indicates that mast cells could comprise an important cell population responsible for the neovascularisation of these tumours. Further investigations into mast cell derived angiogenic mediator release induced by tumour cells in SCC of the oesophagus might provide not only a better understanding of the interaction of mast cells and tumour cells during angiogenesis, but might also help to predict responses to angiogenesis inhibiting agents.