Article Text

Abstract
Aims—Prolactin plays an important role in the proliferation and differentiation of normal breast epithelium, and possibly in the development of breast carcinoma. The effects of prolactin are mediated by its receptor; thus, alteration in the expression of this receptor could be important in studying the biology of breast cancer. This investigation was aimed at comparing the expression of prolactin receptors in normal, benign, and malignant breast tissue.
Material/Methods—The expression of prolactin receptors was studied in paraffin wax embedded sections of 102 breast biopsies (93 female and nine male), using the monoclonal antibody B6.2, and the avidin–biotin immunoperoxidase technique. Six biopsies were normal, 34 had benign lesions, and 62 were malignant.
Results—In normal cases, prolactin receptor positivity was seen only on the luminal borders of the epithelial cells lining ducts and acini. In most benign lesions, variable degrees of luminal and cytoplasmic staining were seen. Cells showing apocrine metaplasia and florid regular ductal epithelial hyperplasia were mostly negative. In malignant cases, the staining pattern was mostly cytoplasmic and heterogeneous. Forty one of the 59 carcinomas in women showed a degree of positivity involving 10–100% of the tumour cells. A significant direct correlation was found between prolactin receptor and oestrogen receptor staining when only cases that scored more than 100/300 for the latter receptor, using the H scoring system, were considered (p = 0.0207). No correlation was found between prolactin receptors and progesterone receptors, patient's age, tumour size, tumour grade, or axillary lymph node status.
Conclusions—Prolactin receptors seem to be expressed at different cellular sites in normal, benign, and malignant breast epithelial cells. The receptor is expressed in more than two thirds of female breast carcinomas, suggesting that it may play a role in the pathogenesis of the disease. The positivity is correlated with moderate and strong staining for oestrogen receptors in tissue sections, but not with other prognostic factors.
- breast
- breast carcinoma
- male breast
- prolactin receptors
- oestrogen receptors
Statistics from Altmetric.com
Prolactin plays an important role in the proliferation and differentiation of normal breast epithelium and in stimulating postpartum lactation.1 Prolactin may also play a role in the development of breast carcinoma,2 in addition to a variety of benign breast lesions, including duct ectasia,3,4 fibrocystic change,5 and granulomatous mastitis.6 The effects of prolactin are mediated by its receptor; thus, alteration in the expression of this receptor could be important in studying the biology of breast diseases, including carcinoma.
The prolactin receptor (PrlR) is a transmembrane protein that belongs to the cytokine receptor superfamily, and is expressed in a wide variety of tissues in addition to the breast.1 It is closely related to the growth hormone receptor,7 and is encoded by a single gene located on chromosome 5.8 The receptor consists of three parts or domains: extracellular, transmembrane, and intracellular domains. In experimental animals, several isoforms of the receptor have been identified. These differ in the length and composition of their intracellular tail and are known as short, intermediate, and long PrlR. In all these isoforms the extracellular, ligand-binding domain is identical.7 In humans, there is also evidence to suggest the presence of more than one PrlR form, but until recently only the long form has been cloned.8
Studies of the distribution of PrlR in human breast tissue are limited. In the 1970s, evidence for the presence of PrlR in human breast carcinoma was presented using biochemical binding assays.9 Susequently, similar assays were used to study the prognostic relevance of these receptors in breast carcinoma.10,11 The prolactin receptor was cloned in 1988 by Boutin et al.12 In 1993, Banerjee et al characterised the antibody B6.2,13 a monoclonal antibody directed against the extracellular domain of the human PrlR. This was raised against a membrane enriched fraction from metastatic human breast cancer cells. Prolactin induced growth of T47D human breast cancer cells was blocked by the addition of B6.2 to the medium, and specific binding of B6.2 to the cells was completely inhibited by prolactin.13 This antibody has been used successfully for the demonstration of PrlR in gastrointestinal14 and breast15 tissue, and non-Hodgkin's lymphoma cell lines.16 In our study, we have used B6.2 to investigate the expression of PrlR in a wide variety of normal, benign, and malignant breast tissue sections, to explore the possible presence of alterations that could be useful in studying the biology of breast cancer.
Material and methods
Our study comprised 102 breast biopsies derived from 93 female and nine male patients. All were seen and operated upon during 1996/1997 at Charing Cross Hospital, London. Six biopsies were normal, from reduction mammoplasties, 34 had benign lesions (eight fibrocystic change, nine fibroadenomas, six intraduct papillomas, three duct ectasias, two lactating adenomas, and six cases of gynaecomastia) and 62 were malignant (from 59 women and three men). Benign cases were selected to reflect a spectrum of common benign lesions. Malignant cases were all consecutive primary invasive breast carcinomas. All haematoxylin and eosin stained sections were reviewed and a representative section was selected from each case for our study. New 5 μm sections were cut from the corresponding paraffin wax blocks and immunostained as described below. Clinical and pathological information were obtained from pathology reports. For carcinomas, this also included oestrogen (ER) and progesterone (PgR) receptor status in all cases, as assessed by immunohistochemistry,16 and axillary lymph node status in most cases. In all malignant cases, the original sections were reviewed to confirm the histological type and grade of the tumours.
For the immunohistochemical demonstration of PrlR, the avidin–biotin complex (ABC) immunoperoxidase technique was used. Sections were dewaxed and 2% hydrogen peroxide in methanol was applied for 10 minutes to block endogenous peroxidase. Antigen retrieval was then carried out by placing the slides for five minutes in 100 ml Tris buffered saline (TBS) that had been prewarmed to a temperature of 37°C. Just before the slides were placed in the bath, 0.01 g of protease XXIV enzyme (Sigma, Poole, Dorset, UK) was added. Sections were then washed and 200 μl of normal horse serum (Serotec, Oxford, UK) in TBS were applied. After draining and washing, the primary antibody, B6.2,13 diluted 1/2000 in TBS, was applied. This was followed by washing and applying the secondary antibody biotinylated horse antimouse immunoglobulin (Vector Laboratories, Peterborough, UK) diluted 1/400 for 45 minutes. After rinsing, freshly prepared avidin–biotin peroxidase complex (Vector Laboratories) was added to the slides for 45 minutes. This was followed by applying diaminobenzedine (Vector) for five minutes, washing, and counterstaining with Harris's haematoxylin (BDH Ltd, Poole, Dorset, UK). For carcinomas, a tumour was considered PrlR positive when more than 10% of the tumour cells were positively stained.
Unstained sections from normal and benign biopsies were also assessed for ER using the ABC technique and the monoclonal antibody 1D5 (Dako, Cambridge, UK) at a dilution of 1/100 after a pressure cooker retrieval step.17
Statistical analysis was carried out using the χ2 and Fisher's exact tests.
Results
NORMAL BREAST
PrlR positivity was seen in all cases examined, in the form of dark brown staining of the luminal borders of the epithelial cells lining the ducts and acini (fig 1). Staining was heterogenous and varied in intensity from one case to another and sometimes from one area to another in the same section. Myoepithelial cells were negative, in addition to fibrous tissue and blood vessels.
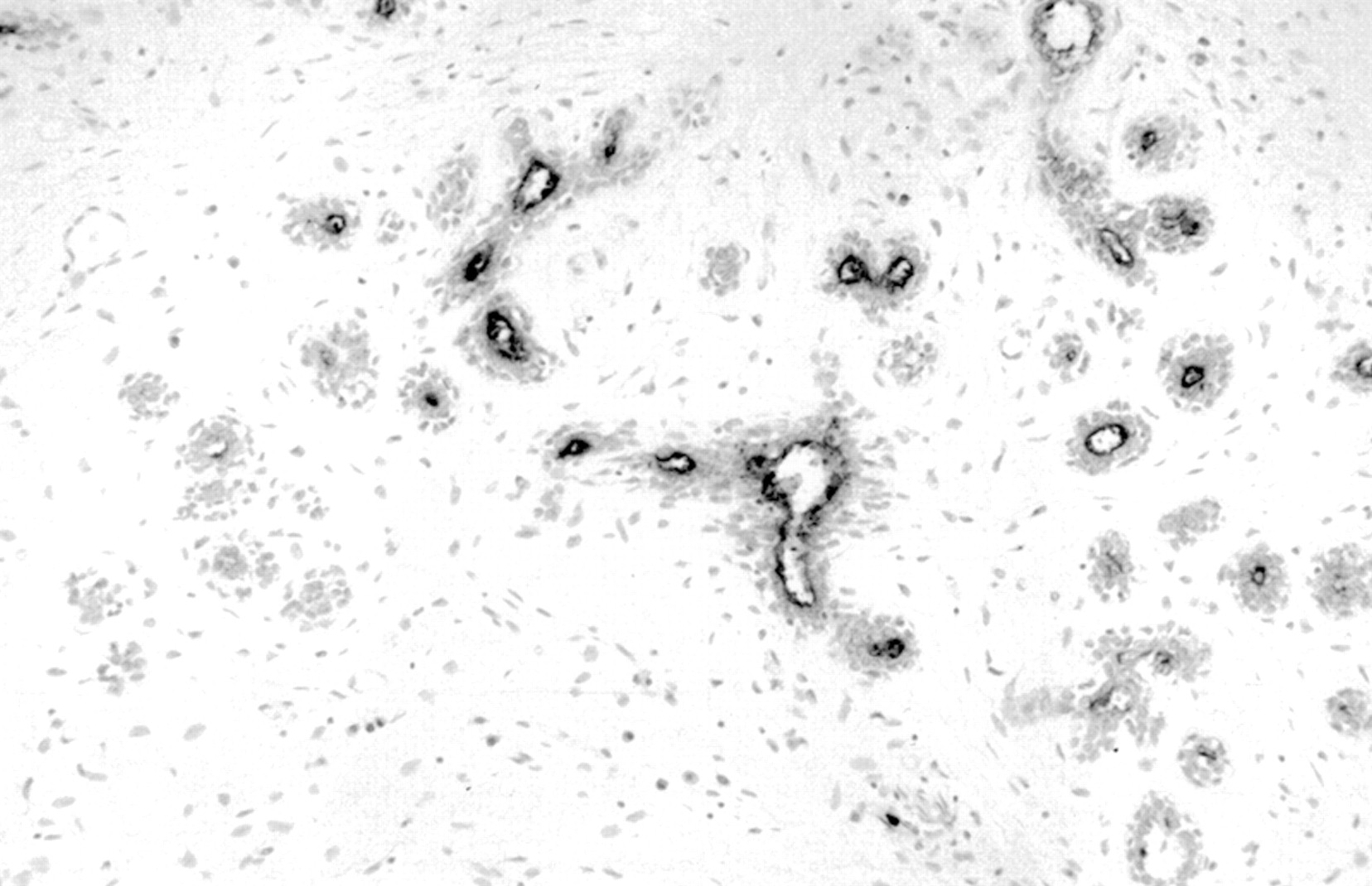
Normal mammary ducts and acini showing prolactin receptor luminal staining.
BENIGN LESIONS
Most benign lesions showed more intense positive staining than that seen in normal ducts and acini. Thus, in addition to the luminal staining, intense cytoplasmic staining was also noted in many cases. The staining pattern was heterogenous and some cases were totally negative.
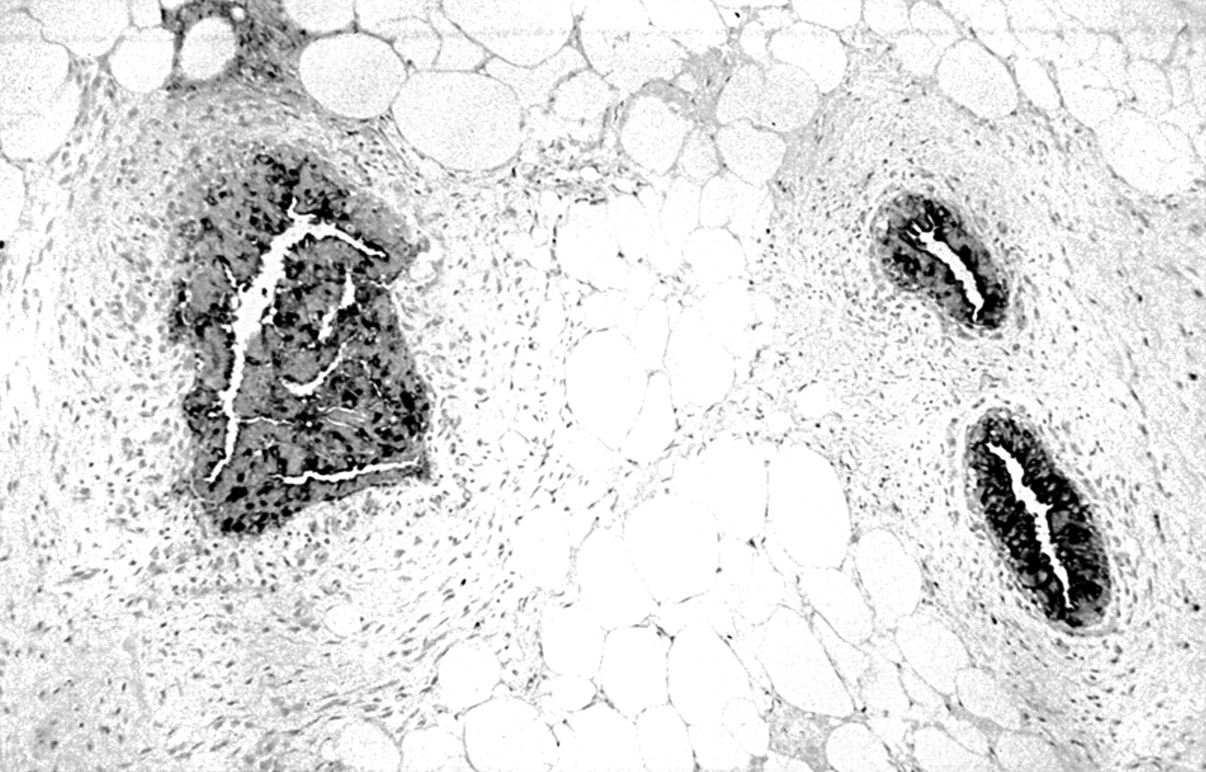
All nine fibroadenomas were PrlR positive, although in some cases staining was focal. Luminal and cytoplasmic staining were present (fig 2). Four of eight cases of fibrocystic change showed focal positive staining of ducts and cysts. Apocrine metaplasia, seen in five cases, was always negative. The proliferating epithelial cells in three foci of florid regular ductal hyperplasia were also negative (fig 3). All six intraductal papillomas showed patchy positive staining, which was mostly localised to the luminal borders. In general, the larger the papilloma the more extensive the staining was. Two of the three biopsies with duct ectasia showed strong positive staining of cells and luminal contents. Of the two lactating adenomas examined, one showed patchy luminal positivity and the other showed patchy strong cytoplamic positivity (fig 4). Five of the six gynaecomastia cases showed heterogeneous luminal and cytoplasmic staining. Staining was particularly strong in a biopsy from a 71 year old patient (fig 5), compared with that seen in cases from young patients.

Fibroadenoma, prolactin receptor positive zonal cytoplasmic staining. Scattered positively stained lymphocytes are also seen.

Florid ductal epithelial hyperplasia, mostly prolactin receptor negative, except for focal luminal staining.

Lactational adenoma, positive prolactin receptor cytoplasmic staining.

Gynaecomastia, strong positive prolactin receptor luminal and cytoplasmic staining.
FEMALE INVASIVE BREAST CARCINOMA
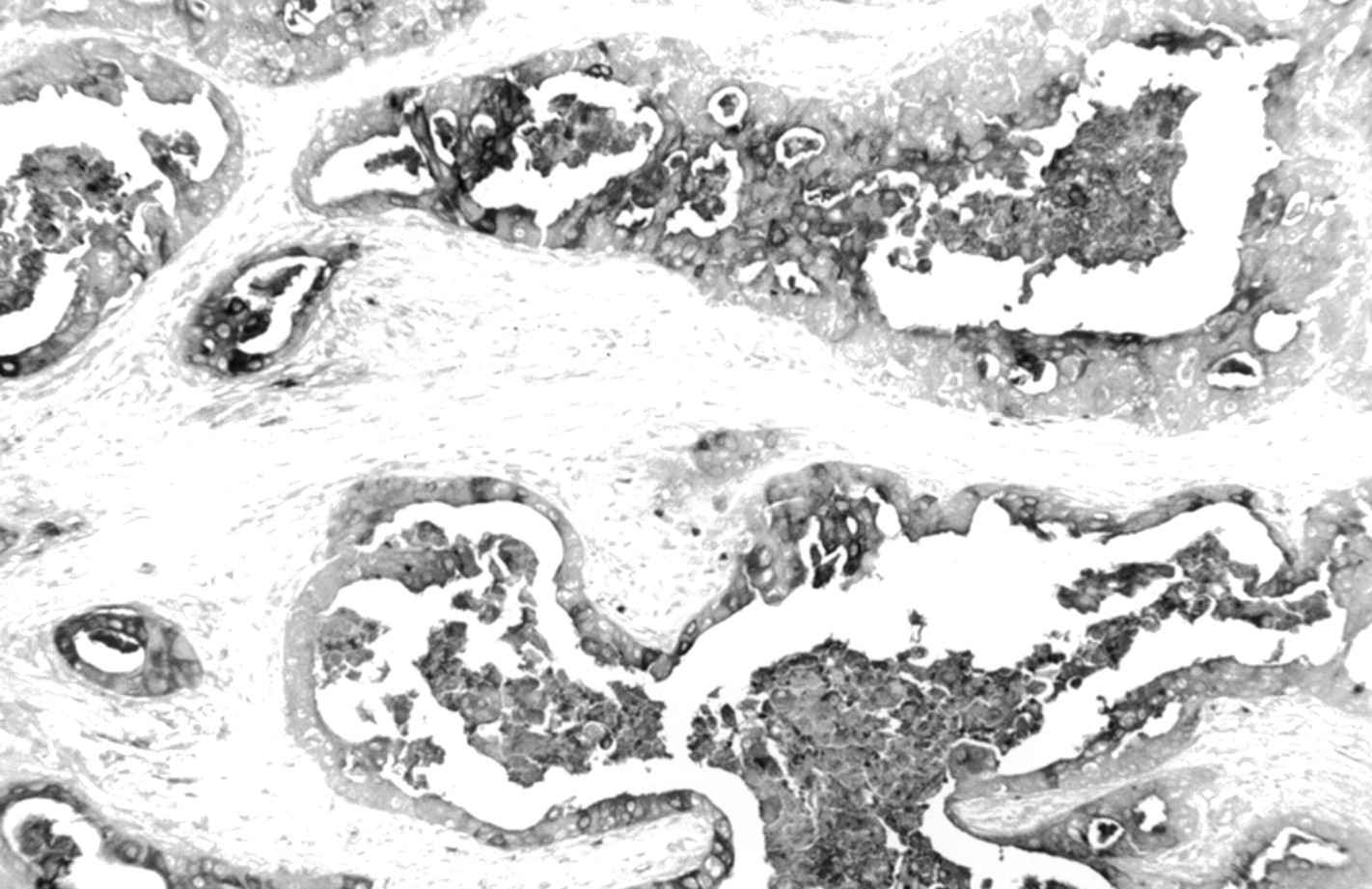
The 59 cases examined included 52 ductal, four lobular, one tubular, one mucinous, and one squamous carcinoma (table 1). Seven cases were grade I, 28 grade II, and 24 grade III (table 1). Information about axillary lymph node status was available in 35 cases. Of these, 17 had node metastases and 18 did not (table 1). Forty one of the 59 showed a degree of PrlR positivity, which involved between 10% and 100% of the tumour cells in the sections examined. The staining pattern was mostly cytoplasmic and heterogeneous (fig 6). Sometimes, staining appeared to be zonal, with strongly stained areas seen alongside negative areas.
Relation between histological type, tumour grade, nodal status, and oestrogen (ER) and progesterone (PR) receptor status, and staining for prolactin (PrlR) receptors in female invasive breast carcinoma

Invasive ductal carcinoma, showing strongly positive cytoplasmic and membrane staining for the prolactin receptor. Note unstained stroma between tumour cells.
Of the 52 invasive ductal tumours, 36 were PrlR positive. Three of the four lobular tumours were positive. Both the tubular and mucinous cases examined were positive, whereas the invasive squamous case was negative (table 1). Because of the negative staining noted in benign apocrine metaplasia, we stained a section of an invasive apocrine carcinoma from our archives for PrlR. Focal cytoplasmic and luminal positive staining was present (fig 7). This case is not included in the statistical analysis, because it was not part of the consecutive series.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Invasive apocrine carcinoma showing focal positive cytoplasmic and luminal staining for the prolactin receptor.
There was no significant relation between PrlR staining and patient's age or tumour size. Patients with positive tumours varied in age between 32 and 80 years, with a mean (SD) of 60.3 (13.3) years. Patients with negative tumours had an age range of 39–89, with a mean (SD) of 54.7 (13.1) years. Although patients with positive tumours had an older mean age than those with negative tumours, the difference was not significant (p = 0.1396). Tumours positive for PrlR varied in size between 5 and 80 mm and had a mean (SD) of 23.6 (15.6) mm. Negative tumours varied between 9 and 57 mm, with a mean (SD) of 25.4 (14.9) mm (p = 0.6756, not significant).
In addition, there was no correlation between PrlR staining and tumour grade or axillary lymph node status. The percentage of positively stained tumours was similar in each grade (five of seven for grade I, 20 of 28 for grade II, and 16 of 24 for grade III; table 1), in addition to node positive and negative tumours (12 of 17 and 12 of 18, respectively; table 1).
A significant direct correlation was found between PrlR and ER staining when only cases that scored more than 100/300, using the H scoring system,16 were considered (p = 0.0207; table 1). No correlation was found between PrlR and PgR (p < 0.5; table 1).
MALE INVASIVE BREAST CARCINOMA
Only one of the three cases examined, which were all of the invasive ductal type, showed PrlR positivity in more than 10% of the tumour cells. All three cases were strongly positive for ER.
Discussion
Our study shows that PrlR, as demonstrated by the B6.2 antibody, seem to be expressed heterogeneously at different sites within normal, benign, and malignant breast epithelial cells. Expression is mainly along the luminal border in normal cells and is mostly cytoplasmic in malignant cells. In benign lesions, expression (when present) seems to vary between luminal, cytoplasmic, or a combination of the two. In that respect, we noted complete absence of PrlR expression in the main mass of proliferating epithelial cells in the three cases of florid ductal hyperplasia examined, although there was positive staining of the residual lumina (fig 3). Apocrine metaplasia was consistently negative for both PrlR and ER, but focal staining was seen in a case of invasive apocrine carcinoma. In contrast, some cases of lactational adenoma showed diffuse cytoplasmic staining, which was not unlike that seen in some carcinomas (fig 4). More cases need to be examined to assess the importance of these findings.
Around two thirds of female breast carcinomas showed positive staining for PrlR. This is similar to that reported previously in a study using a different antibody and a different technique (immunoblot analysis),18 but is less than the 95% positivity reported by the same group in another study using immunohistochemistry.19 These two studies also showed discrepancies with regard to the relation between PrlR and ER expression, with the first study, but not the second, reporting a direct relation between the two. In our study, we found a direct correlation between PrlR and moderate/strong, but not weak, expression of ER; that is, cases that had an ER H score of more than 100. Thus, it is clear that different techniques and different antibodies may yield different results. What seems to be consistent in our study, in addition to the above reported studies, is the site of the expressed receptor, which appears always to be luminal in normal cells and cytoplasmic in malignant cells. However, it must be emphasised that these results are obtained when the appropriate dilution is used. For B6.2, the dilution used in our study was 1/2000. When the same antibody was used at a stronger dilution (1/250) by another group of investigators, cytoplasmic and nuclear staining of normal and malignant epithelial and myoepithelial cells, in addition to stromal cells, was obtained.15
Even though a correlation between PrlR and strong expression of ER in female breast carcinoma was seen in our study, there were cases that were positive for one receptor and negative for the other (including 17 female malignant cases). In addition, two of the three male cancers examined were PrlR negative, whereas all tumours were strongly positive for ER. As for benign cases, a striking discrepancy in the expression of the two receptors was noted in the three florid ductal hyperplasias examined, which were all PrlR negative but strongly ER positive. In contrast, five of the six gynaecomastia cases examined, all showing a degree of epithelial hyperplasia, were PrlR positive, and all six cases were strongly positive for ER. All these findings suggest that although the expression of the two receptors is commonly linked, with evidence suggesting the presence of crossregulation between them,20 dissociation can occur in certain pathological states. This is supported by two recent studies carried out at our laboratory where PrlR expression was found in 15 of 16 cases of ER negative ductal carcinoma in situ,21 and in 80% of invasive breast carcinomas presenting during or shortly after pregnancy and lactation, in which the expression of ER was absent in half of the cases.22 In contrast, the absence of PrlR expression in apocrine metaplasia is consistent with the reported lack of crossregulation between androgen receptors and PrlR,20 because there is a possible link between androgen receptors and apocrine metaplasia.23
A few carcinomas in our study showed a zonal distribution, with negative areas seen alongside positive areas. This difference in reactivity was sometimes associated with clear differences in tumour morphology. This phenomenon has been seen before. In 1954, Foulds noted that mouse mammary tumours often exhibited zones of different morphologies, suggesting that these tumours were zonal, with different areas being biologically different from each other.24 Thus, the difference in PrlR expression in these “zonally reactive tumours” may reflect important biological differences between different parts of a given tumour. This heterogeneity may have therapeutic implications if tumour cells of different zones happen to respond differently to certain therapeutic agents.
Most of the studied cases were of the invasive ductal type, with only five invasive lobular cases, but even so the percentages of PrlR positive cases were similar in both types (69% and 75%, respectively; table 1). The absence of PrlR staining in the single case of squamous cell carcinoma examined is not surprising, and is consistent with the derivation of these squamous cells from non-luminal, possibly myoepithelial, cells.25 Conversely, the positive staining noted in the two mucinous and tubular cases is consistent with an origin from a luminal cell type.
There was no correlation between PrlR expression and tumour grade, size, or axillary lymph node status, suggesting that the assessment of PrlR would not be useful as a prognostic factor. Perhaps, the recent characterisation of an intermediate isoform of the human prolactin receptor,26 in addition to the previously characterised long form, would help in providing more refined tools for the study of PrlR in breast cancer. In particular, it would be interesting to know whether the distribution of these isoforms in normal and abnormal breast tissue is different, and whether specific isoforms have a site specific distribution within cells.
Because prolactin plays an important role in the proliferation and differentiation of normal breast epithelium,1 it is suggested that the higher expression of PrlR noted in the cells of most benign and malignant breast lesions, compared with normal cells, could be an important factor in the pathogenesis of these diseases, rather than a reflection of the high proliferative activity of the abnormal cells.
Acknowledgments
An abstract of this study was presented at the Winter Meeting of the Pathological Society of Great Britain and Ireland, Cambridge, January 1999. This work was submitted in part fulfilment of BSc degree requirements (SG).