Article Text

Abstract
Aims: One of the limitations of fine needle aspiration biopsy (FNAB) of the breast is in distinguishing invasive carcinoma (IDC) from ductal carcinoma in situ (DCIS). It has been proposed that the presence of myoepithelial cells overlying epithelial malignant cell clusters suggests DCIS. However, the recognition of myoepithelial cells in aspirates may be difficult. The aim of this study was to investigate a new nuclear myoepithelial cell marker, p63, a p53 homologue nuclear transcription factor, in a series of breast FNABs in an attempt to distinguish IDC from DCIS.
Methods: Papanicolaou stained smears from eight cases of pure DCIS and 15 cases of pure IDC with a histologically confirmed diagnosis were submitted to immunocytochemical analysis using the antibody 4A4 against p63. Two pathologists evaluated the presence of p63 positive cells overlying malignant cell clusters and admixed with malignant cells. The frequency of p63 positive cells in DCIS and IDC was compared using Fisher's exact test.
Results: p63 consistently stained the nuclei of myoepithelial cells, either overlying malignant cell clusters and/or admixed with malignant cells. p63 positive myoepithelial cells were seen in all DCIS cases and in nine of the 15 cases of IDC (p = 0.0375). In eight cases (three DCIS and five IDC), scattered p63+ epithelial malignant cells were seen.
Conclusions: Although p63 positive myoepithelial cells are found more frequently in DCIS cases, their presence cannot be used as a criterion to rule out invasion in breast FNABs because they are present in up to 60% of invasive cases.
- breast
- ductal carcinoma
- immunocytochemistry
- myoepithelial cells
- p63
- DCIS, ductal carcinoma in situ
- FN, false negative
- FNAB, fine needle aspiration biopsy
- FP, false positive
- IDC, invasive ductal carcinoma
- TN, true negative
- TP, true positive
Statistics from Altmetric.com
- DCIS, ductal carcinoma in situ
- FN, false negative
- FNAB, fine needle aspiration biopsy
- FP, false positive
- IDC, invasive ductal carcinoma
- TN, true negative
- TP, true positive
During the past few years, cytologists and pathologists have faced new challenges in diagnostic cytopathology practice. The “more information with less material” paradigm is progressively increasing the minimal diagnostic and prognostic information that must be included in every cytopathology report.1,2 Most of these requirements are the result of new treatment strategies and surgical approaches that avoid axillary lymph node dissection.1–3 In the 1960–80s, most patients were clinically diagnosed with large palpable breast lesions and treated with mastectomy when diagnosed with either an in situ (DCIS) or an invasive (IDC) ductal carcinoma of the breast in fine needle aspiration biopsies (FNABs).2,3 Thus, for cytopathologists, it was not necessary to decide whether a ductal carcinoma was invasive or not, based on cytopathological findings.3 However, since the early 1990s, conservative surgical approaches without axillary dissection have been advocated for patients with DCIS so that a distinction between IDC and DCIS on cytological samples has frequently been required by clinicians.2,3 In addition, stereotaxic core needle biopsy of the breast has gained popularity in clinical practice, because it has similar negative predictive values when compared with FNAB,4 and in many cases may also allow the distinction between invasive and in situ tumours.5
Several cytomorphological criteria have been tested with regard to their accuracy in distinguishing between DCIS and IDC, although only modest results have been achieved.2,3,6–10 It has been proposed that malignant cell clusters forming tubular structures, with cytoplasmic lumen formation, and the presence of stromal and/or fat fragments infiltrated by neoplastic cells favours a diagnosis of IDC.2,3 In contrast, the presence of foamy macrophages, calcifications, and, most importantly, myoepithelial cells overlying tumour cell clusters points toward a diagnosis of DCIS.2,7 Most authors stress that a cautionary approach should be taken in this situation, because invasion cannot be ruled out with certainty. In the study published by McKee et al,2 most of the above mentioned criteria were not sufficiently specific and sensitive to be applied independently to individual cases. In that study, they found that the presence of myoepithelial cells overlying malignant cell clusters was significantly associated with DCIS.2 However, on cytological examination, the correct identification of myoepithelial cells is sometimes difficult, because they might be confused with apoptotic cells, stromal cells, or even epithelioid histiocytes.2,7,11
“Preliminary studies indicated that p63 might be better than other conventional myoepithelial cell markers because it decorates the nuclei of myoepithelial cells, thereby overcoming the cytoplasmic fragility of myoepithelial cells in fine needle aspirates”
Recently, p63, a p53 homologue nuclear transcription factor that is consistently expressed in the basal cells of stratified epithelia and myoepithelial cells, was characterised.12–14 Barbareschi and colleagues12 and our group13 have shown that p63 is a reliable myoepithelial cell marker in histological sections. Moreover, some preliminary studies indicated that p63 might be better than other conventional myoepithelial cell markers12,13,15 because it decorates the nuclei of myoepithelial cells, thereby overcoming the cytoplasmic fragility of myoepithelial cells in FNAB.
While evaluating a series of benign and malignant FNABs, we noticed the presence of p63 positive myoepithelial cells overlying malignant cell clusters in some cases of DCIS. This finding prompted us to investigate the usefulness of p63 positive myoepithelial cells overlying malignant cell clusters and admixed with malignant cells in differentiating between DCIS and IDC in FNAB.
MATERIAL AND METHODS
Eight cases with a histologically confirmed diagnosis of pure DCIS and 15 with a histologically confirmed diagnosis of pure IDC of the breast were retrieved retrospectively from the pathology files of the Hospital São João, University of Porto, Porto, Portugal. The histological sections were reviewed by two of the authors and the diagnoses of pure DCIS and pure IDC were reconfirmed. In each case, smears obtained by previous FNABs were available. Only those cases with a Papanicolaou stained slide with cytological features consistent with a diagnosis of ductal carcinoma were included in our present study.
The histological and cytological samples were reviewed by two of the authors, and the most representative Papanicolaou stained cytology slide was chosen for the immunocytochemical analysis, as described previously.16 Briefly, the coverslips of Papanicolaou stained slides were removed. Heat induced antigen retrieval in a wet bath, using the Dako antigen retrieval solution was performed for 20 minutes in all samples. Immunocytochemistry was performed according to the streptavidin–biotin–peroxidase technique using the antibody 4A4 raised against p63 (1/200 dilution; Neomarkers, Freemont, California, USA), as described elsewhere.17 Only cells showing strong and distinctive nuclear immunoreactivity for p63 were considered positive. Cytoplasmic and membranous staining were considered non-specific. Positive (histological sections of a sclerosing papilloma with myoepithelial hyperplasia) and negative (omission of primary and secondary antibodies) controls were included in each slide run. All controls gave appropriate results.
In our present study, we specifically searched for p63 positive cells overlying malignant cell clusters and for p63 positive myoepithelial cells admixed with malignant cells. We compared their frequency in histologically confirmed DCIS and IDC. Statistical analysis was performed with Statview 5.0 software. Statistical differences between p63 expression in myoepithelial cells overlying malignant cell clusters and admixed with malignant cells, and the final histological diagnosis were calculated using Fisher's exact test. A test was considered significant only if the two sided p value was less than 0.05. We also calculated the sensitivity and specificity of the presence of p63 positive myoepithelial cells as a marker for DCIS. Sensitivity was defined as the ratio between: the number of DCIS cases with p63 positive myoepithelial cells (true positive; TP)/TP + the number of DCIS cases without p63 positive myoepithelial cells (false negative; FN). Specificity was defined as the ratio between: the number of IDC cases without p63 positive myoepithelial cells (true negative; TN)/TN + the number of IDC cases with p63 positive myoepithelial cells (false negative; FN). Both sensitivity and specificity were expressed in percentages.
RESULTS
Table 1 summarises the cytological and histopathological data of all cases. The review of the pure DCIS and IDC cases revealed that there was no invasive component in the DCIS cases and no in situ component in the IDC cases.
Summary of clinical pathological features of the 23 cases of breast cancer studied and p63 expression in myoepithelial cells
Cytological analysis of p63 stained slides showed a distinctive nuclear staining pattern in myoepithelial cells; a faint background was seen in three cases, although this did not impair the evaluation of the slides.
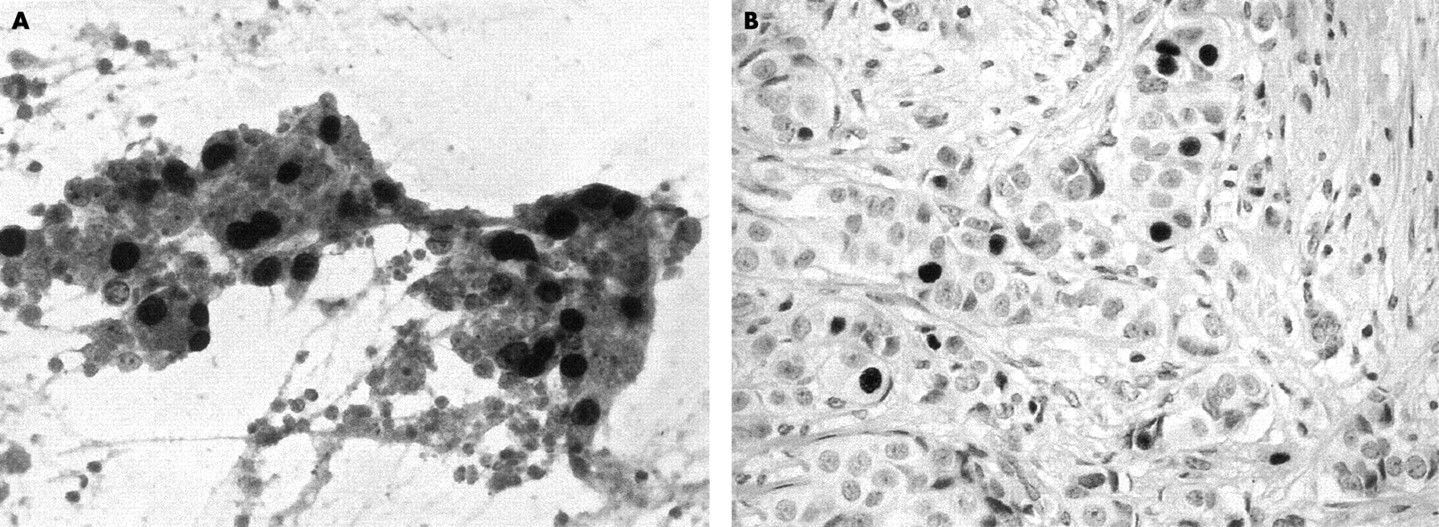
p63 positive myoepithelial cells overlying malignant cell clusters were seen in all DCIS cases (fig 1A) and in 60% (nine cases) of IDCs (fig 1B). Most importantly, the presence of myoepithelial cells was significantly more frequent in DCIS than in IDC cases (p = 0.0375). The sensitivity of p63 positive myoepithelial cells for the diagnosis of DCIS was 100% (8/(8 + 0) = 1 × 100 = 100%) and its specificity was 40% (6/(6 + 9) = 0.40 × 100 = 40%). When stratified by grade, p63 positive myoepithelial cells were seen in 100% of grade I, 40% of grade II, and 50% of grade III IDC cases.

p63 immunocytochemistry highlighting myoepithelial cells overlying tridimensional malignant clusters. (A) Photomicrography showing a fine needle aspiration of a ductal carcinoma in situ with the typical distribution of p63 positive myoepithelial cells. (B) Similar findings in an invasive ductal carcinoma. Note the presence of intracytoplasmic lumens/vacuoles (arrows). Streptavidin–biotin–peroxidase/diaminobenzidine stain; original magnification: A, ×200; B, ×400.
A remarkable feature seen in our present study was the presence of scattered (< 5%) p63 positive neoplastic cells in eight cases (three cases of DCIS and five of IDC) (fig 2A). In two of these cases, up to 5% of the neoplastic cells also showed positivity for anti-p63 antibody applied to histological sections (fig 2B), whereas in six no p63 positive neoplastic cells were seen in the histological samples.

{kind=link}
{kind=link}
p63 positive invasive ductal carcinoma not otherwise specified. (A) Note the presence of malignant cells with p63 positive nuclei. (B) Histological section of the same case showing a grade III invasive ductal carcinoma with scattered p63 positive cells. Both streptavidin–biotin–peroxidase/diaminobenzidine stain; original magnification, ×200.
DISCUSSION
Currently, the treatment of breast carcinomas is tailored according to a constellation of clinical and pathological findings. The presence or absence of invasion is one of the major characteristics that determine whether or not a patient will be submitted to axillary dissection or even to neoadjuvant chemotherapy.3
Several groups have searched for specific cytological criteria that may guide pathologists in determining the presence or absence of invasion.2,3,6–10 Several criteria have been described, including tumour cell dissociation, the presence of tubular/glandular structures, cytoplasmic lumens/cytoplasmic vacuoles, fibroblastic proliferation, infiltration of fat/mammary stroma by neoplastic cells, and the presence of myoepithelial cells overlying malignant cell clusters.2,3,6–10 McKee and colleagues2 emphasised that to diagnose invasion, pathologists need look for the presence of stromal fragments or fat tissue invaded by neoplastic cells, because these findings are seen only in IDC and not in DCIS; in the absence of these criteria, the presence of cytoplasmic lumens/vacuoles and tubule formation suggest invasion.2 It should be noted that these criteria are not seen in all cases, and even in the series of McKee et al,2 only 72% of IDCs displayed definitive stromal or fat tissue invasion; moreover, in our opinion, the identification of stroma/fat tissue invasion in cytological preparations is very far from straightforward.
In contrast, the identification of certain cytological features may suggest the absence of invasion, pointing towards a diagnosis of DCIS. In the series of McKee et al,2 the most important criterion to suggest DCIS was the presence of myoepithelial cells overlying tumour cell clusters. However, myoepithelial cells are frequently misidentified, because in FNAB smears some of their usual cytomorphological features are distorted and they may be confounded with apoptotic cells, stromal cells, epithelioid macrophages, or even cancer cells with a spindle cell phenotype.2,6,7,10,11
“Most importantly, p63 does not crossreact with secretory cells, breast stromal cells, smooth muscle cells, endothelial cells, pericytes, and neural cells”
In this study we evaluated p63 expression in FNABs from eight cases of DCIS and 15 cases of IDC. Based upon our results and on those previously reported,2,7,9 myoepithelial cells overlying malignant cell clusters were significantly more frequent in DCIS than in IDC cytological samples (100% of DCIS cases v 60% of IDC cases; p = 0.0375); however, in contrast to published results,2,7,9 we found these cells in 60% of IDC samples (specificity, 40%). This discrepancy is most probably related to the high sensitivity of p63 for myoepithelial cells, but we cannot exclude the possibility that it could be related to the small number of samples evaluated in our study. Another possible explanation could be the presence of an associated DCIS in those cases diagnosed as IDC, although even after a review of the histological samples of all IDC cases included, no DCIS component was found. However, we cannot rule out the possibility that the neoplastic areas selected at gross examination, which were submitted to histological analysis, and reviewed herein failed to identify the foci of DCIS. It should be noted that because many IDCs are associated with DCIS, the specificity of p63 positive myoepithelial cells overlying malignant cell clusters may putatively be lower in diagnostic cytopathology practice than that obtained in our present study.
It has been shown that p63 is a reliable myoepithelial cell marker12–15 and that it overcomes the problem of myoepithelial cell cytoplasm fragmentation during fine needle aspiration, because it is expressed in the nuclei of myoepithelial cells in contrast to all of the other myoepithelial markers,11–15,18 which decorate either the cytoplasm or the cytoplasm and nucleus of myoepithelial cells. Most importantly, p63 does not crossreact with secretory cells, breast stromal cells, smooth muscle cells, endothelial cells, pericytes, and neural cells.12,13,15 However, we must emphasise that scattered p63 positive neoplastic cells might be seen in up to 34.8% of cases. According to our previous result,14 these might reflect a partial myoepithelial/basal cell differentiation of some breast carcinomas.12,15 It is noteworthy that these p63 positive cells did not pose a problem in the final diagnostic interpretation.
Take home messages
-
p63 consistently stained the nuclei of myoepithelial cells, either overlying malignant cell clusters and/or admixed with malignant cells
-
p63 positive myoepithelial cells were seen in all ductal carcinoma in situ (DCIS) cases and in nine of the 15 cases of invasive ductal carcinoma (IDC); in addition, scattered p63 positive epithelial malignant cells were seen in three cases of DCIS and five of IDC
-
Thus, although p63 positive myoepithelial cells are found more frequently in DCIS they are present in up to 60% of invasive cases and cannot be used as a criterion to rule out invasion in breast fine needle aspirates
In conclusion, the presence of myoepithelial cells overlying malignant cell clusters is a very frequent finding in DCIS,2 but it is also found in up to 60% of IDC samples. We stress that the identification of myoepithelial cells is easy using p63 antibodies in Papanicolaou stained slides. Our results indicate that the presence of myoepithelial cells either overlying malignant cell clusters or admixed with neoplastic cells is not a useful criterion to rule out invasion (or suggest the presence of DCIS) in diagnostic cytopathology practice.
Acknowledgments
This study was partially supported by a PhD grant from the Portuguese Science and Technology Foundation (FCT) (reference SFRH/BD/5386/2001 - JSRF) and Programa Operacional Ciência, Tecnologia e Inovação (POCTI) do Quadro Comunitário de Apoio (QCA) II.