Article Text

Abstract
We assessed a population-based cohort of patients diagnosed with oropharyngeal squamous cell carcinoma in Southeast Scotland over 13 months. p16 and human papilloma virus (HPV) expression were determined, and correlated with stage, treatment, smoking and alcohol history, and disease outcomes. Retrospective analysis was performed on 60 patients. p16 immunohistochemistry and HPV genotyping were performed on formalin-fixed paraffin-embedded tissues. HPV infection (as defined by p16 positivity and/or HPV PCR positivity) was identified in 57% of samples, while dual positives were detected in 45% of cases. HPV16 was most prevalent of the HPV types and was associated with 90% of positive samples. Cause-specific 1-year and 2-year survivals were 82.5% and 78.2%, respectively. The p16-positive and HPV-positive groups demonstrated significantly increased cause-specific survival in comparison with their negative counterparts.
- HEAD AND NECK CANCER
- HPV
- PAPILLOMA VIRUSES
- IMMUNOHISTOCHEMISTRY
Statistics from Altmetric.com
Introduction
Squamous cell carcinoma of the head and neck (HNSCC) is the sixth commonest cancer in Scotland, with an incidence of approximately 1200 patients per annum.1 From 2001 to 2011, the incidence increased in Scotland by 4.2%.1 Recent data from the Scottish Cancer Registry show that oropharyngeal cancer had the greatest rate of increase of any cancer type from 1988 to 2006; with 2.9-fold and 2.4-fold increases in men and women, respectively (European Age-Standardized Rate).2
Recently, human papilloma virus (HPV) has been shown to have strong association with a subset of oropharyngeal cancers.3 The optimal diagnostic method for HPV-associated oropharyngeal squamous cell carcinoma (OPSCC) is debatable and, currently, there are no internationally defined accepted standards for testing. Strong, diffuse expression of p16 by immunohistochemistry (IHC) provides indirect evidence of transcriptionally active HPV in tumour cells, whereas direct evidence of HPV infection can be provided by PCR or in situ hybridisation-based techniques. A combination of p16 and molecular HPV testing has been proposed as the most effective way of confirming HPV status.
The incidence of HNSCC is increasing in America and Europe, relating to a rise in HPV-associated cancers.4–8 Patients with HPV-positive HNSCC often present at a younger age8 and have a favourable overall prognosis.9 A retrospective cohort with OPSCC in Southeast Scotland by Junor et al10 showed an increase in HPV-associated tumours from 41% to 63% between two cohorts: 1999–2001 and 2003–2005. This study revealed an HPV-positive and p16-negative group, constituting a separate subclass, who may particularly benefit from chemotherapy.
In Scotland, current data are lacking to determine whether HPV-associated OPSCC continues to increase and whether relative proportions of HPV to p16 positivity are consistent. Consequently, this study determines a more contemporary depiction of HPV-associated OPSCC from the same population base.
Materials and methods
Patient cohort
The cohort comprised all patients diagnosed with OPSCC treated in the Edinburgh Cancer Centre from June 2011 to June 2012. Sixty patients were identified.
Following diagnosis, all cases were discussed at a single central multidisciplinary meeting. Based on disease stage, comorbidities and individual patient factors, patients were offered surgery, chemoradiotherapy with or without neoadjuvant chemotherapy, radiotherapy alone, radiotherapy with cetuximab, palliative chemotherapy or best supportive care. Neoadjuvant chemotherapy consisted of two cycles of cisplatin and 5-fluorouracil, with or without docetaxel. Radiotherapy was CT-planned and conformal, using predominantly intensity-modulated radiotherapy (IMRT). Prescribed doses were 68 Gy in 34 daily fractions over 6.5 weeks or 65 Gy in 30 fractions over 6 weeks (IMRT).
Patients were categorised into current smokers, ex smokers or never smokers, and their alcohol intake into heavy, past heavy, moderate or none. Heavy intake was over 14 and 21 weekly units for women and men, respectively.
IHC and HPV genotyping
Residual tumour tissue was available for p16 IHC and HPV genotyping in 56 samples. HPV PCR-based detection genotyping by the Multimetrix HPV Genotyping Assay11 was performed on nucleic acid derived from 10 µm sections of formalin-fixed and paraffin-embedded tissue from the relevant block. The HPV assay detects 24 HPV genotypes including all high risk HPV types. p16 staining was carried out on 3 -µm sections using a monoclonal antibody to p16 (CINtecHistology, mtm Laboratories) on a Leica Bond III automated immunostainer (figure 1A, B). p16 IHC was considered positive if strong and diffuse nuclear and cytoplasmic staining was present in >70% of the malignant cells.12

(A) Typical high-grade basaloid morphology of a tumour subsequently shown to be p16 and human papilloma virus positive. (B) Strong diffuse nuclear and cytoplasmic p16 staining in >70% of cells, and thus scored as positive for p16.
Statistical analysis
Survival was defined as the time from diagnosis to death or last appointment with secondary care, censoring in July 2014. The Kaplan–Meier method was used to calculate actuarial estimates of overall and cause-specific survival (CSS). Comparisons of survival distributions between groups were made using the log-rank test. All statistical analyses were performed using SPSS (V.22).
Results
Sixty cases of OPSCC were identified. Baseline characteristics by HPV and p16 status are shown in table 1.
Baseline clinical characteristics stratified by human papilloma virus (HPV) and p16 status (concordant p16/HPV cases only, n=49)
HPV status was unknown or invalid in three samples whereas p16 status was unknown in one sample. Twenty-nine samples showed evidence of HPV infection on PCR; an overall prevalence of 50.9% (29/57, 95% CI ±11.8%). Of HPV-positive cases, 25/29 were infected by a single HPV type and 4/29 by more than one type. HPV16 was most prevalent, equating to 90% of positive samples. HPV18 was positive in three cases and was always associated with HPV16 co-infection. A single case of HPV35, HPV51 and HPV82 co-infection was found. p16 was positive in 28/59 samples (47.4%, 95% CI ±11.5%) and 25/56 (44.6%, 95% CI ±11.3%) were both HPV and p16-positive.
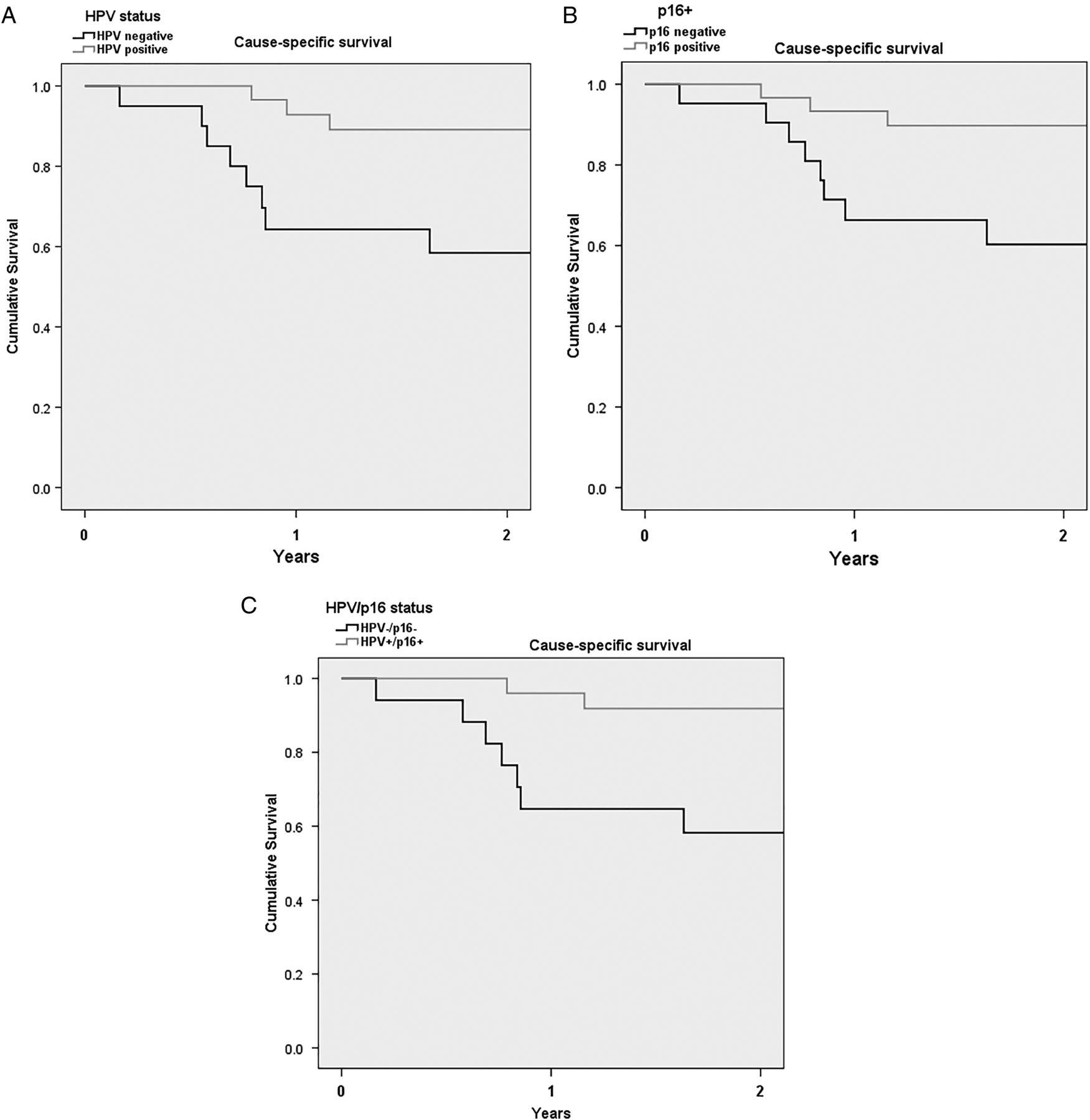
The median survival for the 52 radically treated patients was 25 months. Cause-specific 1-year and 2-year survivals were 82.5% and 78.2%, respectively (table 2). The p16-positive and HPV-positive groups demonstrated significantly increased CSS in comparison with their negative counterparts. Dual p16 and HPV positivity showed a higher CSS than either alone (figure 2). Numbers in the p16/HPV discrepant groups were too small to derive firm conclusions regarding survival.
Clinicopathological characteristics and cause-specific survival

{kind=link}
{kind=link}
(A) Kaplan–Meier survival analysis by human papilloma virus (HPV) (p=0.001). (B) Kaplan–Meier survival analysis by p16 status (p=0.015). (C) Kaplan–Meier survival analysis by HPV and p16 status (p=0.008).
On univariate analysis, smoking and drinking were significantly associated with survival, with current smokers (p=0.017) and current drinkers (p<0.001) displaying worst outcomes. T-stage was strongly associated with survival (p=0.006) but nodal staging was not (p=0.132). Multivariate analysis was performed on the 49 radically treated patients with known HPV status, including variables of age, sex, T-stage, N-stage, smoking and drinking status in the model. The only variable significantly associated with survival was HPV status (HPV-positive HR 0.173, 95% CI 0.042 to 0.713, p=0.015). T4 stage was associated with worse outcomes, though not significantly (HR 3.653, 95% CI 0.906 to 14.726, p=0.069). After adjustment for smoking and drinking, no factors were significantly associated with survival.
Discussion
HPV infection defined by positive p16 on IHC and/or HPV DNA was identified in 57.1% (32/56) in this 2011–2012 cohort—with 44.6% displaying both HPV and p16 positivity. This rate is consistent with other UK series, including the Welsh study by Evans et al,13 who reported a dual HPV/p16-positive prevalence of 55%. The prevalence of HPV-positive/p16-positive cases in the 2011–2012 cohort was also similar to the 41.8% observed in the combined 1991–2001 and 2003–2005 cohort treated at the same Scottish centre.10 Local data indicate a slowly rising incidence of OPSCC in SE Scotland, and longitudinal HPV annotation will help determine how much of this burden is HPV driven.
Two-year CSS was calculated for the HPV and p16 positive group, and was 91.8%, similar to that associated with p16 positivity 89.7% and HPV positivity 89.1% indicating that in this contemporary population, the different measures of HPV infection were associated with very similar outcomes.
Notwithstanding the issues around small numbers, data were stratified into four subsets according to p16 and/or HPV status and compared with the previous work of Junor et al10 (table 3). HPV and p16 co-positivity was found in 44.6% (25/56) in the current study compared with 41.8% (77/184) in the previous cohorts. Of note, the HPV-positive/p16-negative subclass was significantly lower (7.1% vs 30.4%, p=0.0002, Fisher's exact test), while there was a small increase (5.3% vs 2.1%, p=0.4, Fisher's exact test) in the number of HPV-negative p16-positive samples. This possibly reflects a change in the assay used or could represent a change in the pattern of disease. To investigate this more thoroughly, clinical outcomes according to p16/HPV subgroups will be assessed in a larger sample.
Comparison of human papilloma virus (HPV) and p16 subclasses between 2011–2012 and 1999–2001/2003–2005
Limitations of this study include its retrospective and observational nature, and small sample size. Nevertheless, it represents a true population-based approach, including all cases managed by a centre with a catchment population of 1.25 million.
Take home messages
Human papilloma virus (HPV) infection (HPV and or p16 positive) was identified in 57% of this Scottish cohort.
The proportion of cases positive for both p16 and HPV were similar to previous Scottish cohorts, while the proportion of HPV-only cancers reduced.
HPV16 was the most prevalent infection representing 90% of infections.
Patients with HPV-associated cancers demonstrated significantly better survival.
Acknowledgments
Thanks to staff at the Scottish HPV Reference Laboratory for support with practical work and to the Lothian NRS Bioresource for support with sample capture annotation and governance.
References
Footnotes
Handling editor Cheok Soon Lee
Contributors LARW collected clinical and survival data. BC performed immunohistochemistry. SP performed statistics. LARW and KC wrote the manuscript. BC, KC and EJJ edited the manuscript.
Competing interests None declared.
Ethics approval Lothian NRS Bioresouce (SR091).
Provenance and peer review Not commissioned; externally peer reviewed.