Article Text

Statistics from Altmetric.com
Severe combined immunodeficiency (SCID) describes a group of rare genetic disorders characterised by deficient or absent T cell immunity, with an estimated incidence of 1 in 50 000 to 1 in 500 000.1 SCID is considered a paediatric emergency, but early clues, such as lymphopenia, are often not noted.2 As a result, the UK Primary Immunodeficiency Network (UK PIN) recommends that children under 2 years of age with an absolute lymphocyte count (ALC) below 3000/μl must be screened for SCID.3
A retrospective audit was carried out in our hospital to determine whether lymphopenia was noted by clinicians and to assess the feasibility of implementing UK PIN guidelines. Infants with lymphopenia under 3 months of age were identified from laboratory records between 2000 and 2002 and their records were reviewed for features of possible SCID (table 1).
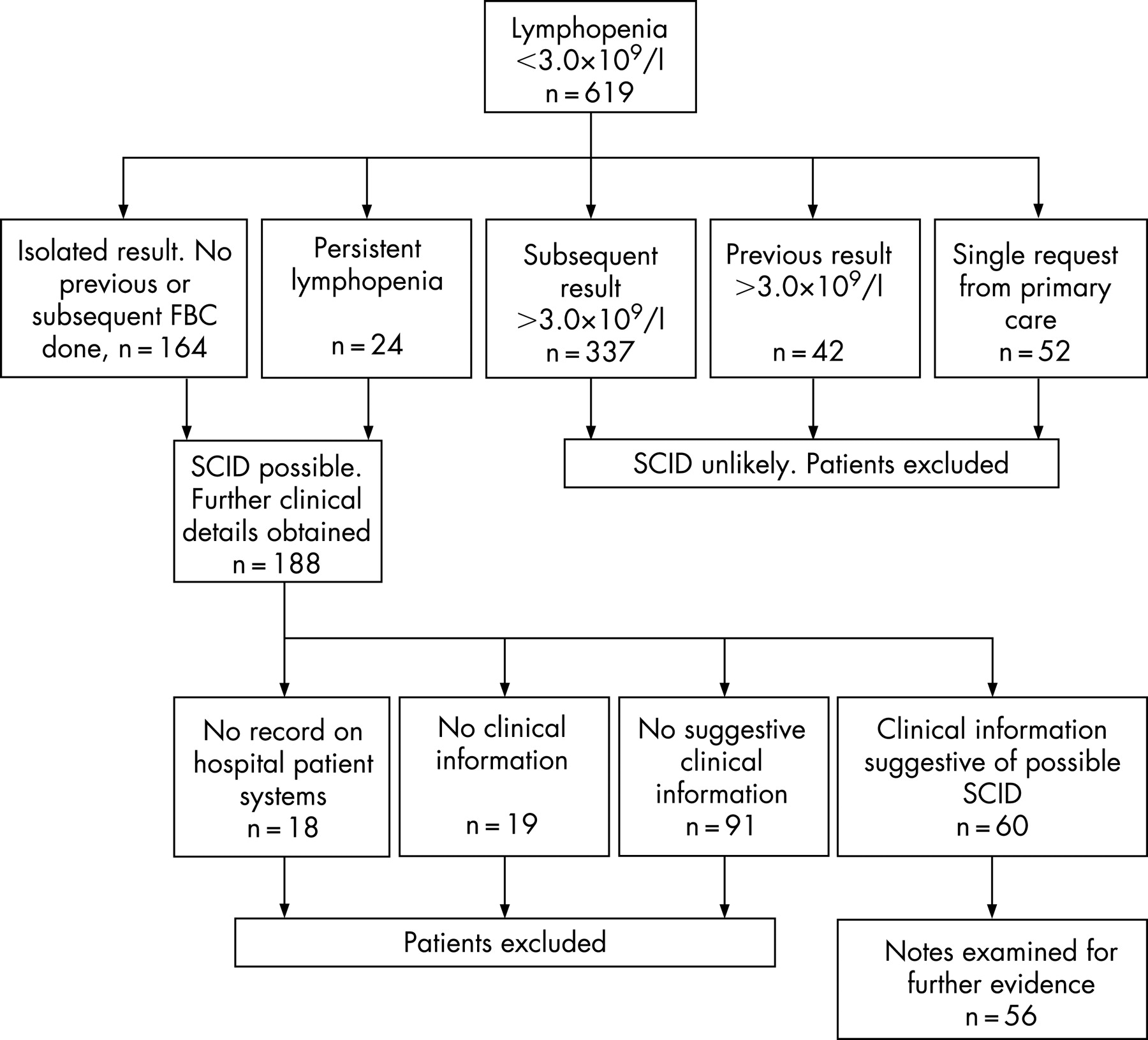
Lymphopenia was identified in 691 (3%) of the infants tested (fig 1). Those with only primary care records, infants with previous or subsequent normal lymphocyte counts and those who died of unrelated causes were excluded. There was no evidence that SCID was considered or investigated in any of the 56 written records finally examined. The presence of lymphopenia was documented by clinicians in only one case. Nine patients had three or more features suggesting possible SCID.
{kind=link}
No clear missed cases of SCID were identified for the period examined, which is unsurprising given the rarity of the disease. However, we have demonstrated that lymphopenia almost always passes unnoticed by clinicians, even when other features are present that should prompt further investigation.
If UK PIN guidelines were strictly implemented, all 619 cases would have been investigated for SCID. Recommended investigations include enumeration of lymphocyte subsets and in vitro functional studies of lymphocyte proliferative responses.3 These highly labour-intensive tests are carried out only in specialised laboratories with input from immunologists. The guidelines state that these investigations should be performed in infants up to 2 years of age, which would increase the workload substantially.
Lymphopenia is a common finding but is rarely noted by clinicians. Given that SCID is a rare condition, it may be not be cost effective to strictly implement UK PIN guidelines for investigation of SCID in all lymphopenic children in this age group. We therefore recommend that routine haematology reports should highlight the finding of lymphopenia in infants less than 2 years of age, and suggest discussion with an immunologist to exclude SCID in appropriate cases.
Footnotes
Competing interests: None.