Article Text

Statistics from Altmetric.com
Approximately 75% of gastric mucosa associated lymphoid tissue (MALT) lymphomas can be cured by Helicobacter pylori eradication.1 It would be very useful to identify, at the time of diagnosis, the 25% of cases of gastric MALT lymphoma that will not respond to H pylori eradication. In general, lymphomas at stage IIE or above do not respond to H pylori eradication.2–4 However, the prognostic value of staging in stage IE cases is very limited, although tumours that involve the muscularis propria or serosa (stage IE2) show a higher failure rate than those restricted to the mucosa and submucosa (stage IE1).2–4 Paradoxically, the majority of gastric MALT lymphomas at diagnosis are at stage IE but 20% of these cases will not respond to H pylori eradication.
In a previous study, we have examined the value of t(11;18)(q21;q21) in prediction of the response of gastric MALT lymphoma to H pylori eradication. Among the 111 cases of gastric MALT lymphoma studied, t(11;18)(q21;q21) was present in 42/63 (67%) non-responsive cases, including 26/43 (60%) at stage IE.5 In contrast, translocation was detected in only 2/48 responsive cases and the two translocation positive cases showed a temporary response to H pylori eradication.5 Based on the same series of cases, we examined the value of t(1;14)(p22;q32)/IGH-BCL10 in prediction of the response of gastric MALT lymphomas to H pylori eradication.
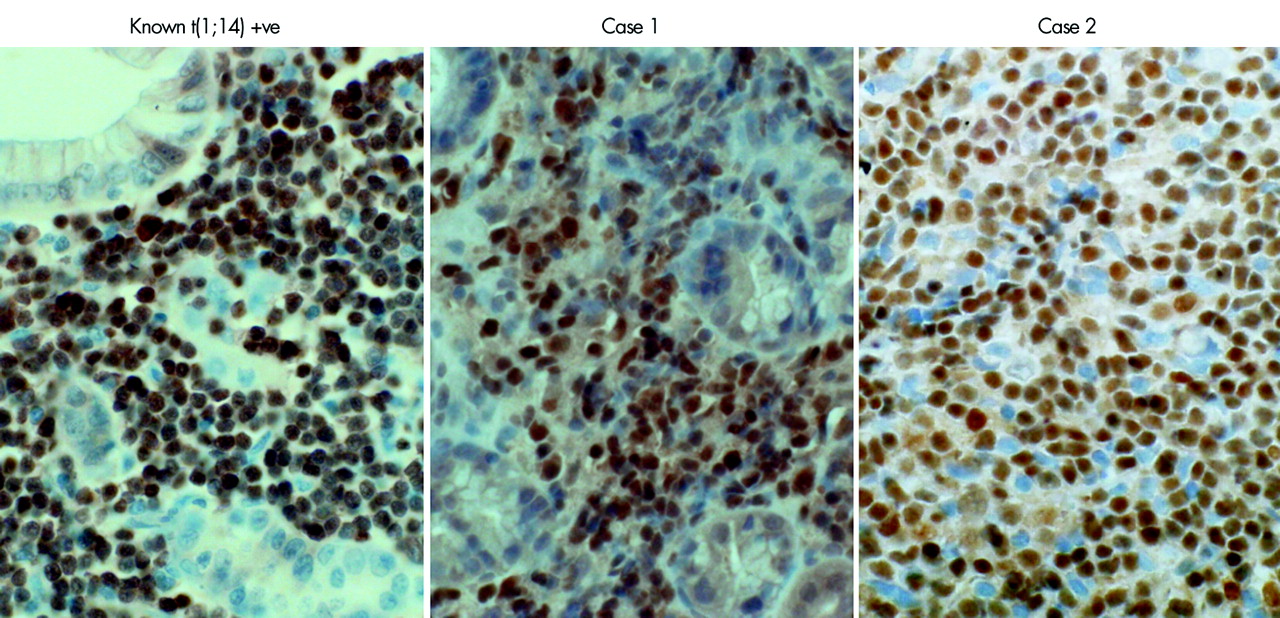
Of the 111 cases examined, 75 including 35 from the complete regression group and 40 from the non-responsive group, had adequate tissue specimens for evaluation of BCL10 staining. Two cases showed strong BCL10 nuclear staining in virtually all tumour cells (fig 1), similar to that seen in t(1;14)(p22;q32) positive cells,6 while the remaining cases displayed either weak cytoplasmic or weak nuclear staining. Both cases with strong BCL10 nuclear staining were from the H pylori eradication non-responsive group; one case (case No 1) had stage IIE disease and showed no response 12 months after H pylori eradication while the other (case No 2) had stage IE disease and showed no response eight months after H pylori eradication. As shown in our previous study, both cases were t(11;18)(q21;q21) negative.5
{kind=link}
BCL10 immunohistochemistry. Both cases 1 and 2 show strong BCL10 nuclear staining in virtually all tumour cells, similar to that seen in tumour cells with t(1;14)(p22;q32).
To ascertain whether the two cases that showed strong BCL10 nuclear staining were positive for t(1;14)(p22;q32) or variant, interphase fluorescence in situ hybridisation (FISH) with BCL10 break-apart dual colour probes, IGH break-apart probes, IGκ break-apart probes, and BCL10/IGH dual colour dual fusion translocation probes were performed.6,7 Both cases failed to show evidence of BCL10 gene break or amplification. Case No 2 showed an IGH break, but FISH with BCL10/IGH dual colour dual fusion translocation probes failed to show evidence of BCL10/IGH translocation. To further investigate these cases, we performed real time quantitative reverse transcription-polymerase chain reaction of BCL10 mRNA. Unfortunately, adequate tissue materials were available only in case No 2. The level (ΔCt = 3.4) of BCL10 mRNA expression in this case was compatible with that in MALT lymphoma with t(1;14)(p22;q32) (mean 1.60 (SD 2.37)), well above that in those without the translocation (6.94 (1.72)).6
To further assess the impact of t(1;14)(p22;q32) on the clinical behaviour of MALT lymphoma, we retrospectively reviewed the clinical presentation of 11 cases, including six from the stomach with known BCL10 involved translocation (table 1). Of these cases, nine including all those from the stomach, were at stage IIE or above. Although clinical presentation and follow up data were not available in each case, three cases (Nos 1, 2 and 7) presented unusual wide dissemination, including pleural effusion, and blood and bone marrow involvement (table 1).
Clinical feature of mucosa associated lymphoid tissue (MALT) lymphoma with t(1;14)(p22;q32) or variants
Taken together, our results suggest that gastric MALT lymphomas with strong BCL10 nuclear expression or t(1;14)(p22;q32) are mostly likely resistant to H pylori eradication.
Acknowledgments
This study was supported by research grants from Leukaemia Research Fund, UK and Deutsche Krebshilfe. The authors thank J Audouin, L Bedenne, O Bouche, Marie-Christine Copin, Y Bouhnik, J Fournet, A De Mascarel, Ph Moreau, J Lafon, A Pariente, and F Piard of the Groupe d’ Etude des Lymphomes Digestifs (GELD), France; T. Thomas and PL Zinzani of Università degli Studi di Bologna, Italy; and M Stolte of Institut fur Pathologie, Klinikum Bayreuth, Germany, for contribution of part of the specimens used for this study.
References
Footnotes
-
Conflict of interest: None declared.