Article Text

Statistics from Altmetric.com
The original British Society of Gastroenterology (BSG) guidelines for the initial biopsy diagnosis of suspected chronic idiopathic inflammatory bowel disease (CIIBD) were published in 1997 in the Journal of Clinical Pathology and by the BSG, and were followed by a supplementary document, also published by the BSG.1–3 The guidelines were comprehensive and evidence-based, and included text, figures, proformas and tables.
A need for revision and update of these guidelines has been identified. New clinical and pathological entities have been described, new approaches to diagnosis and management have been adopted, and there has been sufficient time for pathologists to assess the value of the various elements of the original guidelines. Standardisation of reporting has become more prevalent, encouraged by the publication of cancer reporting guidelines and other CIIBD reporting guidelines.4 Also, the proportion of gastrointestinal (GI) pathology reported by pathologists with a specialist interest has increased.
As an initial step towards revision, an audit of UK GI pathologists’ use of the guidelines was performed in late 2005. The audit aimed to assess awareness of the guidelines, determine their use, identify problems with their application, and gauge support for their revision.
Materials and methods
A one-page questionnaire with a series of questions, and two to four possible replies to each question, was e-mailed to 147 members of the Pathology Section of the BSG, with a reminder 2 months later. Free text replies were also encouraged; 35% of recipients responded. The results were collated and presented by the author to the Pathology Section at the Annual Meeting of the BSG in Birmingham, UK, in March 2006.
Results
Use and value of the guidelines
More than 95% of respondents were aware of the guidelines, and over 95% found them either very useful or quite useful. Regarding specific uses, a majority stated that the guidelines helped with classification, definitions and terms, and teaching, while a minority considered them useful for audit (fig 1).

Proportion of respondents who found the guidelines useful for various aspects of their work.
Suggested clinical and histopathology reporting proformas were published in the original guidelines. The clinical proforma was never used, while the pathology proforma was used by only one respondent.
A “star” system for the value of various histological features was used in the guidelines. This allocated 0–3 stars to a feature according to the strength of the evidence for its diagnostic value. The system was useful to more than 70% of respondents. A suggested flow chart of diagnostic categories for biopsies was used by only 25% of respondents.
The term “indeterminate colitis” was used by 27% for biopsies and by 86% for resections (fig 2). Text responses indicated inconsistent use of this term and some confusion about its meaning. There were pleas for clarification.

Percentage of respondents who used the term “indeterminate colitis” when reporting biopsies and when reporting resections.
Reporting practice
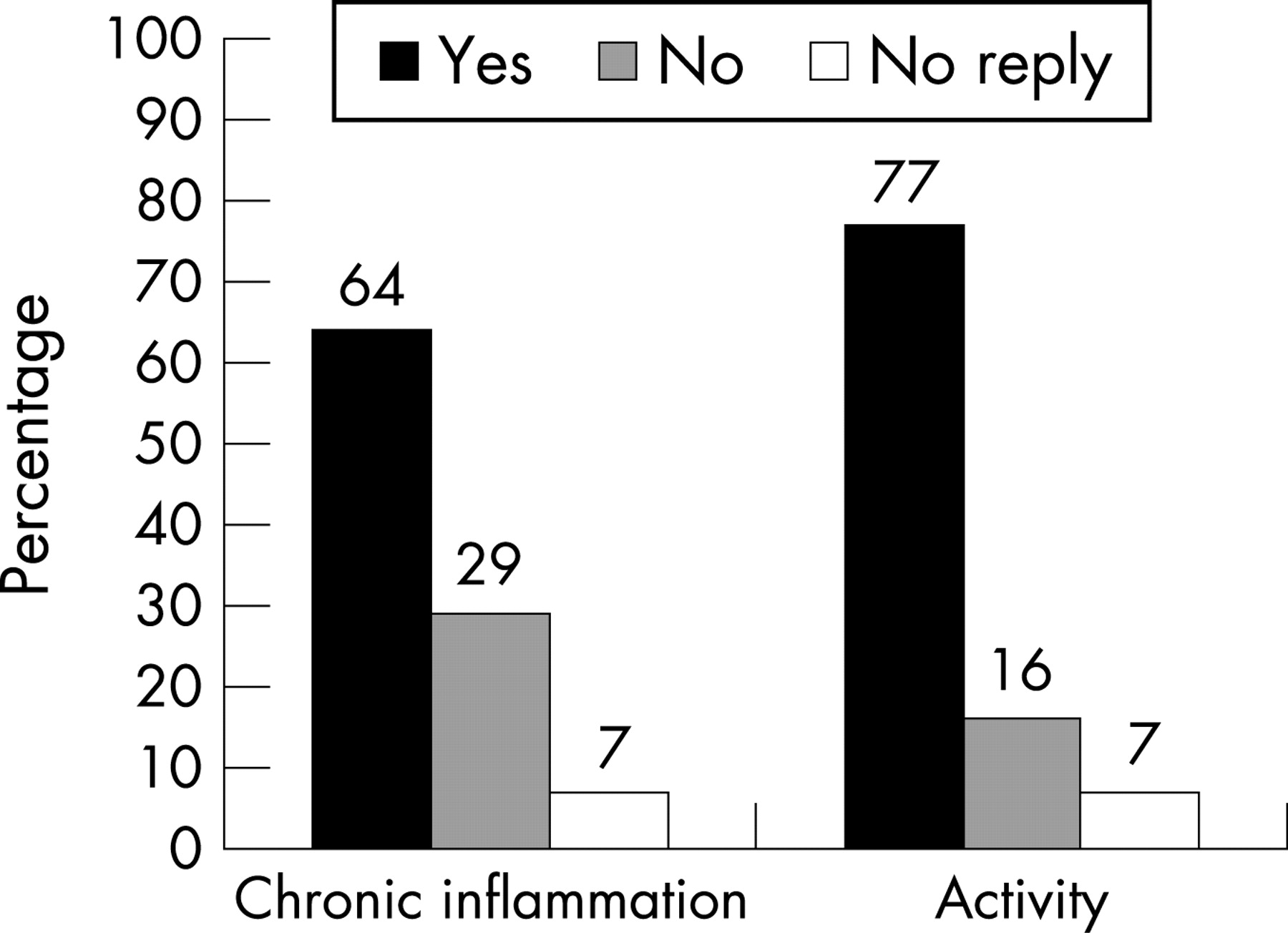
When reporting biopsies, 64% of respondents allocated a grade to chronic inflammation and 77% to activity (fig 3). However, free text replies indicated that pathologists’ approaches differed, which is not surprising given the absence of an agreed grading scheme. For example, some pathologists included chronic inflammation in their assessment of activity, while many did not. It was acknowledged that histological activity, however measured, correlates poorly with clinical and endoscopic activity.4
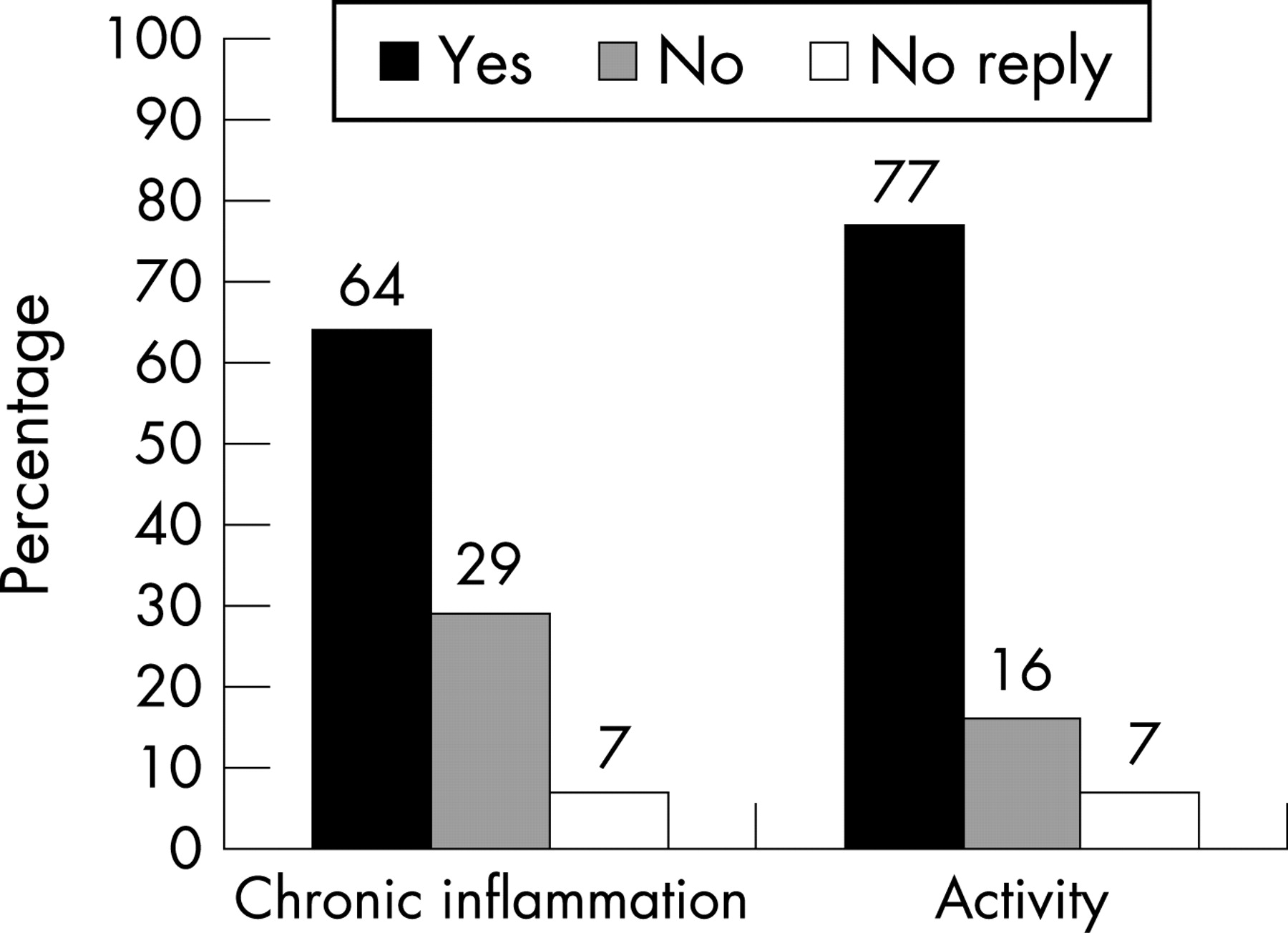
Percentage of respondents who graded chronic inflammation and activity.
Clinicopathological correlation
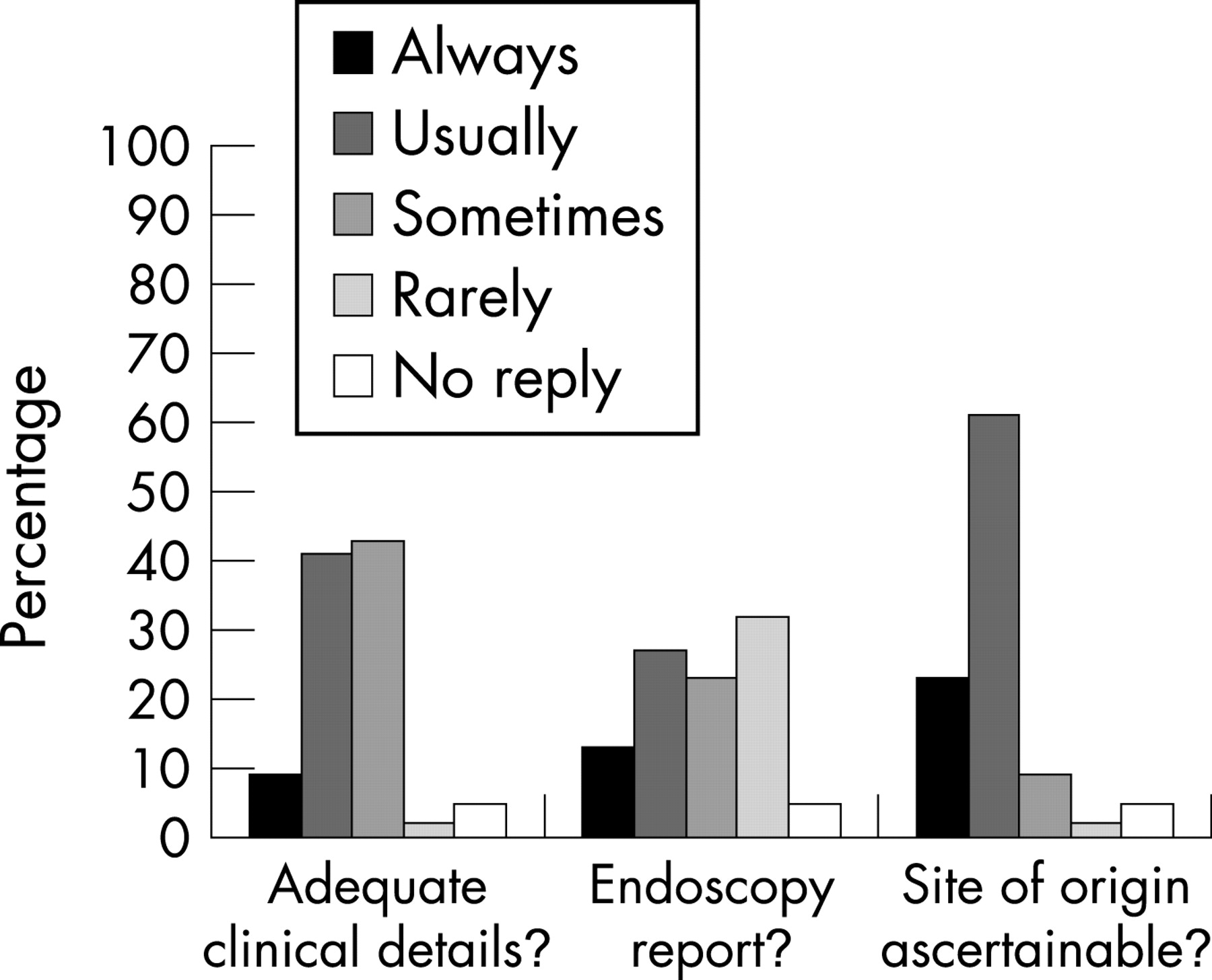
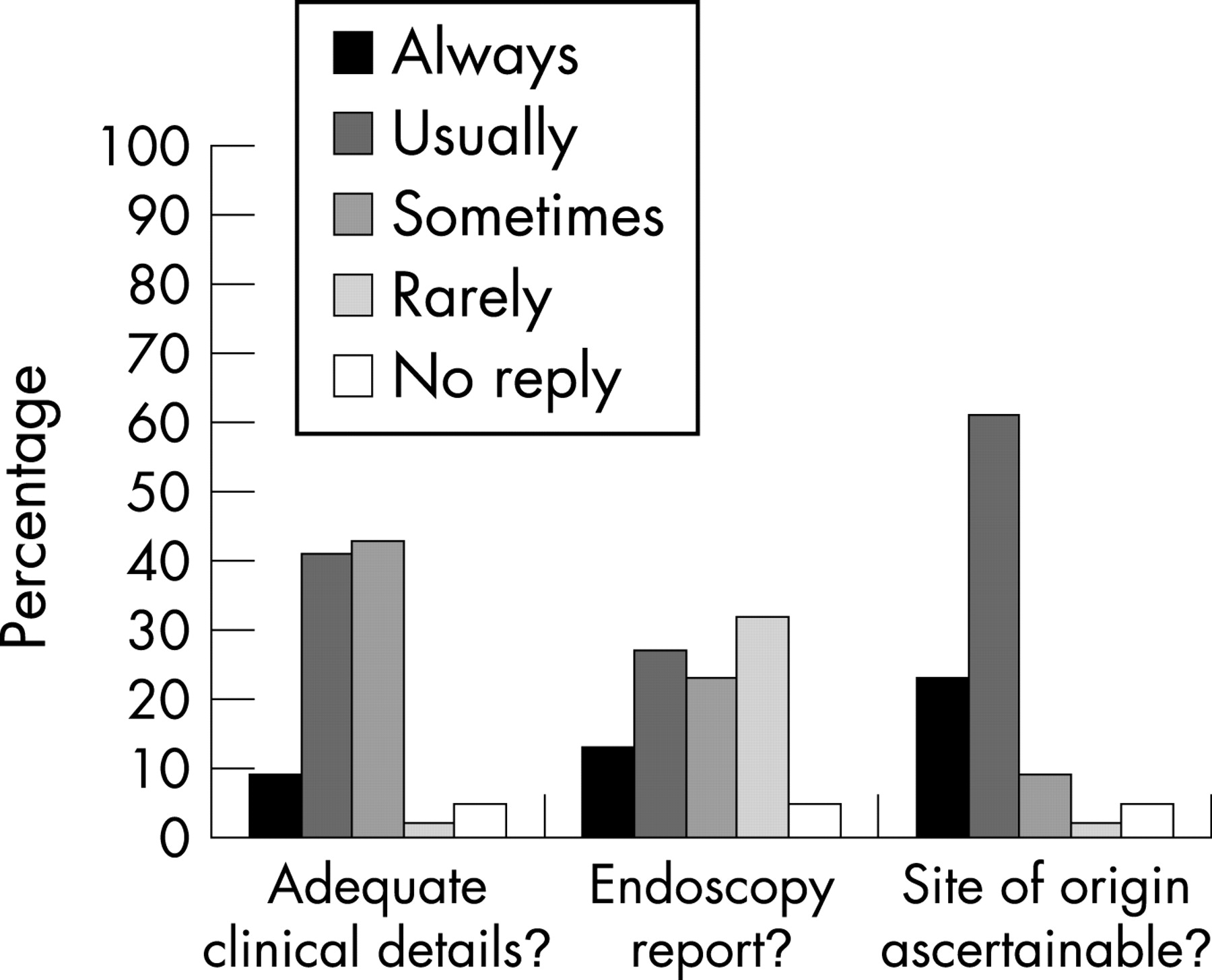
There was considerable variation between respondents in the quality of clinical details received and in the use of the endoscopy report as a request form. Most respondents were always or usually able to ascertain the site of origin of the colorectal biopsies they received (fig 4). For 11% of respondents, there were no opportunities for clinicopathological discussion. Free text comments were supportive of multidisciplinary meetings for non-neoplastic disease as well as for cancer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of respondents who received adequate clinical details and who received a copy of the relevant endoscopy report.
Revision of guidelines
Seventy three per cent of respondents supported a revision of the guidelines, but specific suggestions for the content were diverse. The topics most frequently identified as needing attention were: the effects of treatment on histological patterns of CIIBD; diverticular colitis; diversion colitis; indeterminate colitis; grading of inflammation; approach to the expression of the degree of certainty of a diagnosis/use of the words “suggestive” and “highly suggestive”; and appropriate terminology for inflammation with no specific features. There was support for the idea of a wider audit of consistency of reporting.
Conclusion
The following recommendations were made at the audit meeting:
-
An update is needed, which should take account of guidelines from other groups.
-
The “star” system, indicating the diagnostic value of histological features, is worth retaining.
-
Proformas should be abandoned or completely redrafted.
-
Guidelines for grading of inflammation and for expressing the likelihood of a particular diagnosis would be useful.
-
Recommendations for the use of the term “indeterminate colitis” would be helpful.
Acknowledgements
The author is very grateful to the members of the BSG Pathology Section who participated and to Professor Neil Shepherd for constant support and encouragement.
REFERENCES
Footnotes
-
Competing interests: None.