Article Text

Statistics from Altmetric.com
Adenomas of the stomach are histologically classified into tubular, villous and mixed (tubulovillous) adenoma. In the literature, in two previous studies, only six cases of serrated adenoma of the stomach have been reported. In this communication, we report a newly identified case. The patient presented with gastric complaints. The endoscopic examination showed a pediculated protruding tumour localised in the gastric corpus. Biopsies were reported as tubular adenoma with high-grade dysplasia. A surgical local excision of the tumour was performed. The histological examination revealed elongated fronds with lateral crenated, saw-tooth-like notches as a result of scalloped epithelial indentations. Areas with high grade dysplasia but without invasive carcinoma were demonstrated. This seems to be the first case of serrated adenoma localised in the gastric corpus in the literature.
Rubio1 reported the first case of serrated adenoma of the stomach (cardia) in the literature. Since then, five additional cases in the cardia have been described by the same author.2 In this report, we describe the first case of serrated adenoma localised in the gastric corpus.
The patient was an otherwise healthy woman in her 50s. For the preceding 2 years, she had experienced upper abdominal pain and anorexia.
Barium x ray examination revealed a protruding tumour in the gastric corpus (fig 1). The endoultrasonography showed a pediculated tumour in the greater curvature without infiltration of the gastric wall. Biopsy specimens were reported to have tubular adenoma with high-grade dysplasia.

Barium x ray examination of the stomach showing an ulcerated protruding tumour in the gastric corpus.
Owing to the non-infiltration of the gastric wall, the surgeon decided to perform a local excision. After 2 years, the patient is well, without local recurrence or metastasis.
The surgical specimen comprised a tumour, measuring 9 cm, composed of finger-like fronds giving it a shaggy appearance.
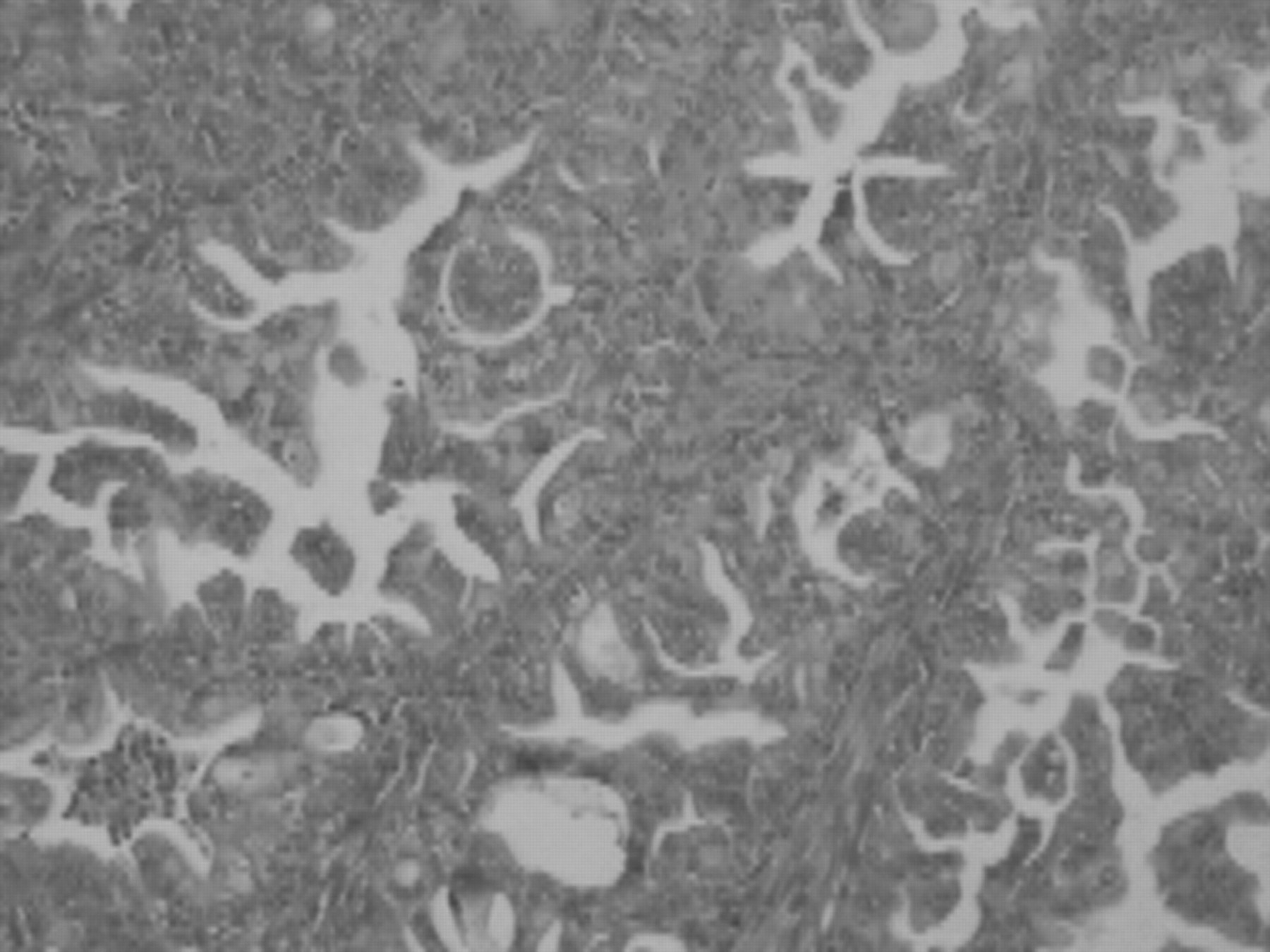
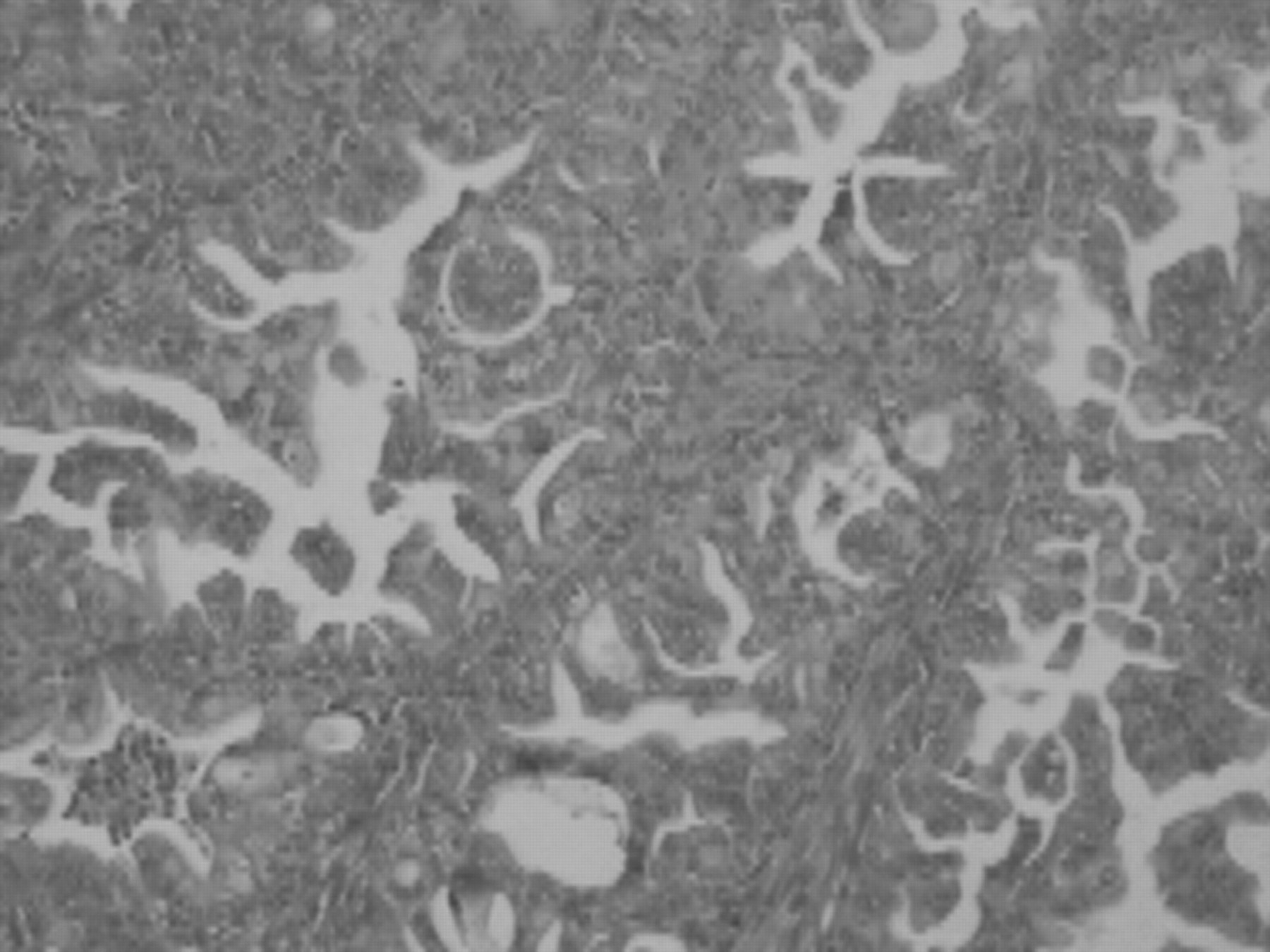
Histological examination revealed a lesion composed of elongated fronds with lateral crenation caused by scalloped epithelial indentations. The nuclei covering the serrated glands were irregular and stratified (fig 2). Mitotic figures were increased. No invasive carcinoma could be demonstrated.
{kind=link}
{kind=link}
Lesion showing serrated, indented dysplastic epithelium with stratified nuclei (H&E; original magnification, ×250).
Discussion
The World Health Organization classification is the generally accepted histological classification of gastric adenomas of the stomach. It divides them into three subtypes: tubular, villous and tubulovillous. Serrated adenomas have not been found in the above-mentioned classification.
In 2001, Rubio1 reported one case of serrated adenoma of the cardia. Since then, five additional cases have been found at his department.2 Except for these six cases, no other case of serrated adenoma of the stomach has been reported. It is conceivable that, in other series, similar cases have been classified as villous adenomas. It is possible that this type of lesion is of rare occurrence in the gastric mucosa although, in a span of 2 years, Rubio found four cases.2
The majority of gastric adenomas are localised in the antral region.3 On the other hand, the six serrated adenomas reported by Rubio were localised in the cardia.1,2 Our report seems to be the first to describe the case of gastric serrated adenoma localised in the corpus.
Nakamura4 found cancerous changes in 15.4% of 911 gastric adenomas. Rubio found that invasive carcinoma was already present at the time of diagnosis in five of six serrated adenomas.1,2 Thus, gastric serrated adenomas behave in an aggressive fashion. Rubio thinks that the propensity to evolve into invasive carcinoma seems to depend on size.2 However, despite the big size of the tumour, no invasive carcinoma was demonstrated.
In conclusion, serrated adenomas of the stomach seem to have distinct location and morphological features, at variance with other histological adenoma phenotypes. It is possible that this type of lesion is of rare occurrence in the gastric mucosa. But, we think that its frequency is underestimated as similar cases may have been classified as villous adenomas.
Footnotes
-
Competing interests: None.