Article Text

Statistics from Altmetric.com
Metastatic localisation of extracanial tumours inside a primary central nervous system (CNS) neoplasm is a rare, but well documented event usually involving meningiomas.1,2 Although metastases to the sellar region are usually found in patients with advanced neoplastic disease, tumour to tumour phenomena in this site are rare and usually involve pituitary adenomas.3,4
This report describes a case of pulmonary adenocarcinoma metastatic inside a pituitary craniopharyngioma and the associated pathological and neuroradiological findings. It also suggests an aetiopathogenetic hypothesis for this event.
A 53 year old man underwent right pulmonary bilobectomy because of a non-small cell carcinoma. Pathological examination showed a pT2 N0 pulmonary adenocarcinoma with vascular invasion. Clinical and instrumental findings were negative for metastatic disease.
Eight months later, the patient presented a visual field defect, diabetes insipidus, and headache. Cerebral computerised tomography (CT) and magnetic resonance imaging (MRI) showed an intrasuprasellar, partially cystic lesion measuring 4 cm in the craniocaudal axis (fig 1). The lesion appeared to be well demarcated, with a partially calcified wall, and presented calcifications and areas of hyperintesity that were taken for haemorrhagic areas. The neoplasm showed an intrasellar and suprasellar component, with chiasmal stretching. Preoperative neuroradiological diagnosis was craniopharyngioma.
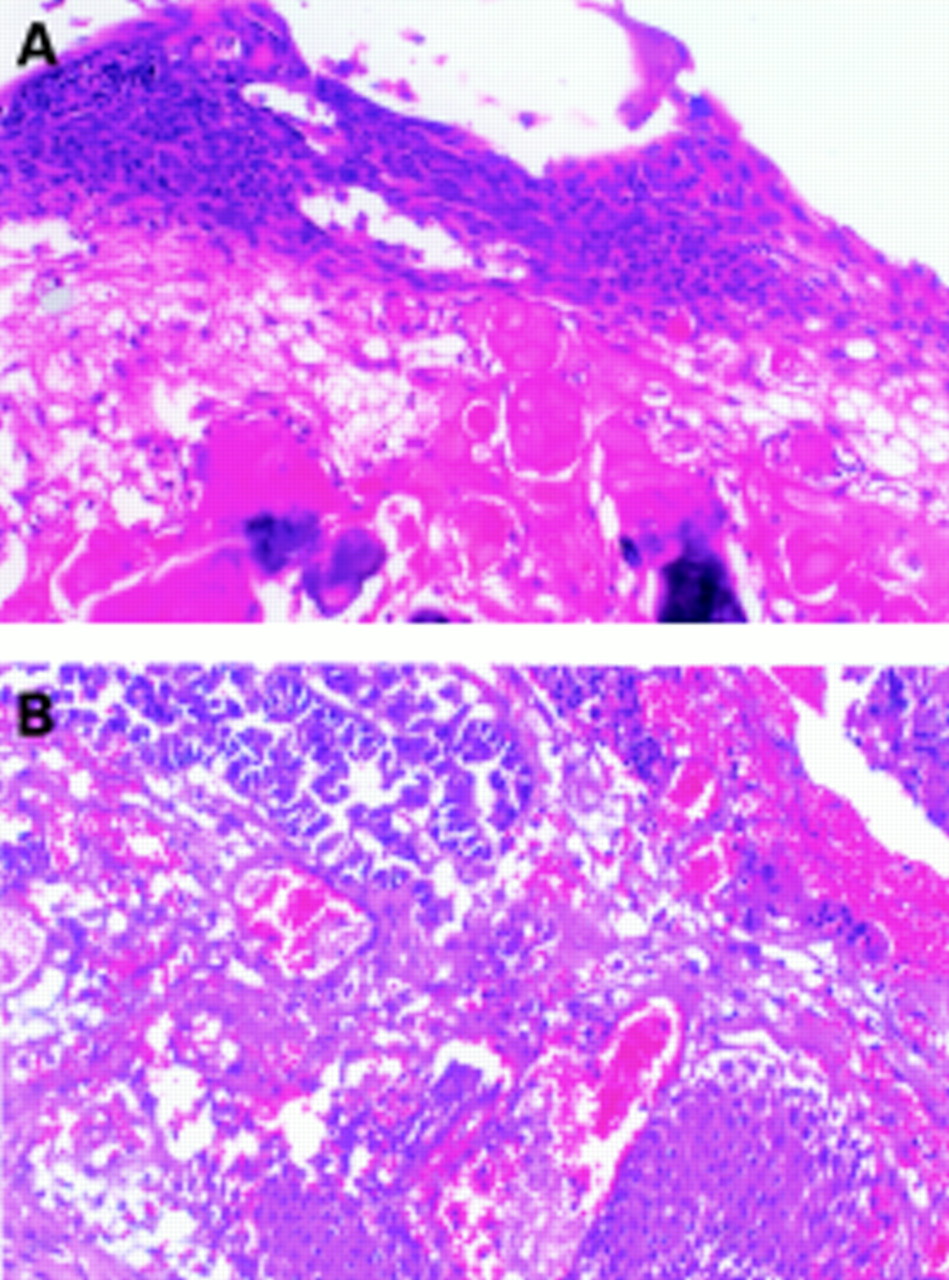
The patient underwent tumorectomy through the right pterional approach. Grossly, the lesion was partially cystic and contained a thick oil-like fluid. Histology showed a moderately differentiated adenocarcinoma with necrotic areas (fig 2) that were histologically similar to the previously removed pulmonary carcinoma. The carcinomatous proliferation was intermingled with a cystic structure. The latter was covered by benign appearing squamous epithelium with masses of keratin with ghost cells, extensive accumulation of cholesterol clefts, and calcifications suggestive of pituitary craniopharyngioma (fig 3A and B).
Immunohistochemical study using antibodies to low and high molecular weight cytokeratin confirmed the epithelial nature of the squamous and glandular component. Although the squamoid component contained low and high molecular weight cytokeratins, the glandular component preferentially expressed low molecular weight cytokeratins .
The histological findings and neuroradiological features supported the diagnosis of an adenocarcinoma metastatic inside a pituitary craniopharyngioma. Clinical history and histological similarities suggested that the lung was the primary site of the carcinomatous component.
Metastases to the sellar region are common in patients with advanced neoplastic disease, and the lung is one of the most common primary sites.3,5 Lesions can be asymptomatic or associated with clinical manifestations.6 In some cases, the metastatic pituitary tumour can be the initial presentation of an unknown primary malignancy.7
Metastatic localisation of extracerebral carcinoma inside a primary CNS neoplasm is a rare, but well documented event. Meningiomas are the most frequent reported host CNS neoplasm,1,2 whereas metastases to a pituitary tumour are extremely rare and usually involve pituitary adenomas.3,4,8 To our knowledge, the present case is the first example of pulmonary adenocarcinoma metastatic to a pituitary craniopharyngioma.
In our case, preoperative neuroradiological findings, namely cranial CT and MRI, led to the diagnosis of craniopharyngioma. The metastatic lesion was evident on haematoxylin and eosin sections, which showed atypical glandular structures intermingled with a cystic structure covered by benign appearing squamous epithelium. The coexistence of a Rathke cyst was ruled out because of the lack of ciliated columnar epithelium. Keratinous masses with ghost squamous cells, calcification, and the accumulation of cholesterol clefts led us to exclude the diagnosis of epidermoid cyst,3 and squamous differentiation within a metastatic pulmonary carcinoma suggested the diagnosis of pituitary craniopharyngioma. The definitive histological diagnosis was adenocarcinoma metastatic inside a craniopharyngioma. The clinical history and histological similarities suggested that the lung was the primary site of the carcinomatous component.
This case underlines once again that unusual neuroradiological findings should be assessed scrupulously. It has been suggested that the possibility of a tumour to tumour phenomenon should be taken into account when faced with unusual CT and MRI findings, especially when there is a clinical history of a carcinoma.2,9,10 Our case presented unusual radiological features in craniopharyngioma, namely areas of hyperintesity that we regarded as bleeding.
It is still unclear why a neoplasm can be the host for a secondary neoplasm. Although primary, multiple benign or malignant tumours in the same patient are present in 2–8% of all patients with cancer, tumour to tumour metastasis is extremely rare.10 Some authors suggested that this phenomenon is not merely casual and different hypotheses have been proposed. Intense vascularisation of the host tumour might provide an increased chance of circulating cancer cells being caught by the host tumour. Thus, the vascular network might act as a filter to metastatic emboli from the bloodstream.2 Studies on the expression of hormone receptors or oncogenes have suggested a biological affinity between metastatic and host tumour.1
However, our present case presented no apparent biological affinity between pulmonary adenocarcinoma and craniopharyngioma; moreover, craniopharyngioma is not a richly vascularised neoplasm and therefore a vascular influence on the genesis of the tumour to tumour metastasis cannot be postulated. Thus, we cannot rule out the possibility that the metastatic spread to the intracranial tumour was merely coincidental.
In conclusion, we underline that: (1) tumour to tumour phenomena do occur, albeit rarely. (2) Craniopharyngioma should be included in the list of CNS tumours able to host a second neoplasm. (3) Unusual neuroradiological, pathological, or laboratory findings always warrant close attention to achieve the correct diagnosis and therefore the best therapeutic approach. (4) Biological affinity between neoplasms may be a predisposing factor of this occurrence. However, the pathogenesis is still unclear and the possibility of an unusual combination of events cannot be ruled out.

T1 weighted magnetic resonance image revealing an intrasuprasellar, partially cystic neoplasm with areas of hyperintensity in the sellar portion.

Haematoxylin and eosin sections showing adenocarcinoma with necrotic areas.

{kind=link}
{kind=link}
{kind=link}
Cystic structure covered by a benign appearing squamous epithelium with masses of keratin with ghost cells and calcification, suggestive of craniopharyngioma (A). Islands of benign appearing squamous cells intermingled with the carcinomatous proliferation (B).